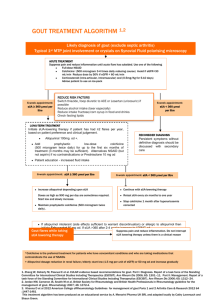
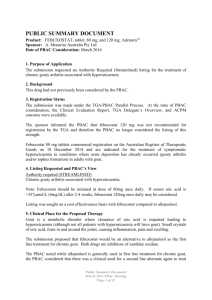
gout management flowchart
advertisement

Likely diagnosis of gout (exclude septic arthritis) Acute Treatment Treat pain and inflammation as soon as possible, continuing until acute flare has settled • Full dose NSAID (eg naproxen 500mg bd or diclofenac 50mg tid +/- PPI) or • Full dose oral Colchicine (500mcg 2-4 times daily) or • Cortico-steroid (oral prednisolone 30mg od for 5 days or IM methyl prednisolone 80-120mg. Where expertise is available consider IA methylprednisolone 40-80mg or triamcinolone 20-40mg) Advise patient to apply an ice pack periodically to affected joint (wrap in a towel to avoid ice burn) Review appointment (4-6 weeks) • Assess lifestyle factors, blood pressure, lipid profile and perform serum urate, kidney and liver function & glucose • Optimise weight, increase exercise, modify diet, reduce alcohol, treat underlying cardiovascular risk factors sUA ≥ 0.36mmol/l sUA <0.36mmol/l Reconsider diagnosis Long term treatment • Persistent symptoms without diagnosis should be referred to secondary care. Note that serum urate frequently falls during gout attacks, so it is important that serum urate is measured after resolution of the flare. • Initiate urate lowering therapy if patient has had ≥2 flares per year based on patient preference and clinical judgement • First line treatment Allopurinol, Second line Febuxostat, Third line Sulphinpyrazone • Co-prescribe low dose NSAID(eg naproxen 250mg bd or diclofenac 25mg TID) +/- PPI or low dose colchicine (500mcg 2 times daily) for at least 6 weeks Repeat sUA (2-4 weeks) sUA <0.36mmol/l Continue urate lowering therapy unless causing side effects Repeat convalescent serum urate in patients suffering recurrent attacks sUA ≥ 0.36mmol/l •Titrate up urate lowering therapy (please see separate flow chart for prescribing in renal impairment and details of drug dosage) • Maintain prophylactic colchicine for up to 6 months during dose titration Urate Lowering Therapy prescribing based on renal function Offer flare prophylaxis for at least 6 weeks with 500mcg colchicine od or bd if tolerated. Measure serum urate every 2-4 weeks and titrate therapy until target of serum urate <0.36mmol/l. Check compliance before assuming inefficacy. eGFR <10 eGFR 10-20 eGFR 20-50 eGFR >50 Start 50mg allopurinol od Start 100mg allopurinol od Start 100mg allopurinol od Start 100mg allopurinol od Maximum 100mg od Maximum 200mg od Maximum 300mg od Maximum 900mg od Intolerance or inefficacy of allopurinol eGFR <30 or Target urate achieved eGFR >= 30 Commence 80mg febuxostat od with 6 months colchicine 500mcg 1-2 tab daily if tolerated Escalate to 120mg febuxostat od after 2-4 weeks if target urate not achieved Intolerance or inefficacy of febuxostat eGFR <90 or Target urate achieved eGFR >=90 Start sulfinpyrazone 200mg od and titrate to maximum 800mg od Consider adding allopurinol if no contra-indication Intolerance/inefficacy of sulfinpyrazone or Target urate achieved +/- allopurinol Continue urate lowering therapy through any subsequent attacks Refer to secondary care for consideration of benzbromarone +/- further allopurinol titration Check convalescent serum urate in patients suffering recurrent attacks and escalate treatment if no longer at target Sulfinpyrazone dose may be reduced for maintenance