Use of clinical laboratory databases to
enable early identification of patients
at highest risk of developing endstage kidney disease
Dr David Kennedy
Dr Hugh Rayner
Dr Jessie Raju
Miss Kamaljit Chatha
Chronic kidney disease (CKD)
• CKD is common – est. 9% adults in England.
• Prevalence increased in older people, those with
diabetes and/or high blood pressure – upward trend.
• Majority have mild to moderate disease – asymptomatic.
• Minority progress to end-stage kidney disease (ESKD)
and require kidney replacement therapy (KRT) (dialysis).
• KRT = poor quality of life & costs £25K per patient per year.
• Early intervention can delay or halt progression to ESKD.
• Some patients remain undetected until very late.
Birmingham Heartlands Hospital
Good Hope Hospital
Solihull Hospital
eGFR test
estimated Glomerular Filtration Rate (eGFR)
• Calculated numerical result - marker of kidney function.
• Based on serum creatinine conc. in blood.
• Adjusted for age, gender and ethnicity.
• From 2006 all UK biochemistry labs have reported eGFR
for all creatinine tests requested for adults.
• HEFT – approx. 9000 creatinine requests per week.
• Results often looked at in isolation or compared to last 2-3.
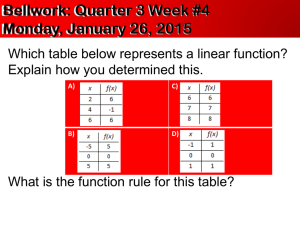
Objectives
• Develop software capable of creating cumulative graphs
of eGFR (up to 5 years data).
• Create a system for identifying patients at highest risk
of developing ESKD using data from the lab computer.
• Build on previous HEFT diabetes renal system.
• Monitor a large population (all clinics and community).
• Clinical Scientists review eGFR graphs.
• System must be capable of replication by other labs.
HEFT Kidney Function Monitor
• Oracle™ database updated daily with data from
Heartlands and Good Hope lab computers
• Generate lists of all patients from previous week
• Aged 65 years or less with eGFR 50 or less
• Aged > 65 years with eGFR 40 or less
• Exclude renal patients and in-patients
• Clinical Scientist reviews approx. 400 cumulative eGFR
graphs identifying patients with significant declining trend
or rapid deterioration.
• High risk patients - report containing eGFR graph and
information for further action sent to requesting doctor.
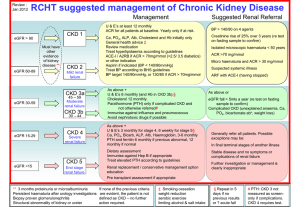
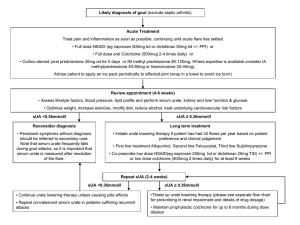
Heart of England Kidney Function Monitor
Patient
Date of Birth
Requesting
Clinician
Date/Time of
Test
ZZC00261281
17-Aug-1938
Dr K Arora
11-Apr-2012 04:13
Sex
Location
M
Perry Park 291 Walsall Rd
Estimated
GFR
35 (ml/min)
01/01/2010
01/01/2011
100
90
80
70
60
50
40
30
20
10
0
01/01/2008
Est GFR (ml/min)
01/01/2009
GFR if Af ro Caribbean
Other Tests From The Last 5 Years
Test
Highest
7.6 %
HbA1c
5.1 mmol/l
Serum K
144 mmol/l
Serum Na
12.4 mmol/l
Serum Urea
0.27 g/l
Urine Protein
Urine albumin:creatinine 30.5 mg/mmol
ratio
Marked as Inf orm Clinician
Date
27/02/2012
11/04/2012
15/09/2008
11/04/2012
15/09/2010
15/09/2010
01/01/2012
Marked as Urgent
Latest
7.6 %
5.1 mmol/l
134 mmol/l
12.4 mmol/l
0.07 g/l
1.7 mg/mmol
Date
27/02/2012
11/04/2012
11/04/2012
11/04/2012
27/02/2012
27/02/2012
Diabetic Status on Renal Database Not Diabetic
Dear Dr Arora,
This results for this patient have reviewed as part of our departments system for monitoring chronic kidney disease
using cumulative graphs of eGFR. Based on our criteria, agreed with the renal medicine department, this patient has
been identified as at increased risk of progression to end-stage kidney disease.
If you requirefurther advice or information for the management of this patient please contact Dr Hugh Rayner at
Birmingham Heartlands Hospital.
Email hugh.rayner@heartofengland.nhs.uk for a copy of 'CKD Made Easy'.
Please quote this patient's NHS number.
Results – 1
Testing using historical data
• Estimated 410 eGFR graphs to review per week.
• Time to review graphs & generate reports approx. 3 hrs.
• 15-20% of graphs reviewed by clinical scientists are
flagged high risk.
• Compared to the renal consultant - clinical scientists flag
more patients as high risk but successfully identify those
at highest risk.
Results – 2
Testing using historical data
• A random selection of patients were retrospectively flagged
as high or low risk for one week in 2008.
• Electronic data gathered in Jan / Feb 2012 (after 3.5 yrs).
• All cause mortality was higher after 3.5 years in patients
flagged as high risk compared to low risk.
• The number of patients with a significantly declining eGFR
over 3.5 years was higher for patients flagged as high risk
compared to low risk.
• The number of patients flagged at high risk who showed a
significant decline in eGFR but had no evidence of
specialist referral is estimated at up to 3% (780 per year).
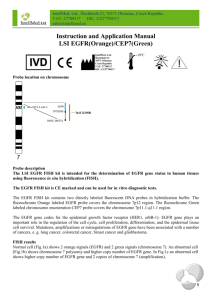
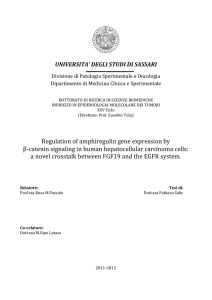
Estimated cost savings
CKD progresses over years – showing early cost savings
is thus impossible.
A study at HEFT using cumulative eGFR graphs showed a
significant fall in the number of diabetic patients requiring
KRT after 5 year - estimated saving £390K
Our monitoring system includes many more patients than the
initial study therefore estimated savings are even more.
Estimated cost of the new system at HEFT is £41K per year.
If 20 patients over the next 5 years are detected earlier
and KRT is delayed by a year net savings = £500K.
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
Number of diabetes patients starting KRT in HEKS
Diabetes patients starting dialysis or transplanted per year
50
45
40
35
30
P<0.001
25
20
15
10
5
Rayner et al. BMJ Qual Saf 2011
0
Future plans
• New system was introduced routinely at HEFT in April.
• Quality data is being gathered prospectively.
• Qualitative feedback (by questionnaire) of primary and
secondary care clinicians will be collected.
• Once embedded at HEFT, we plan to promote our new
system through the clinical biochemist community and
the West Midlands Renal Network.
• We plan to extend the concept of cumulative monitoring
of biochemical tests to other chronic diseases
− Preparing Health Innovation Challenge bid.
Conclusions
• We have developed a system for lab staff to review
cumulative eGFR graphs for a large population and
identify patients at highest risk of developing ESKD.
• We have tested the system using historical data and now
introduced it into routine practice.
• Reports with eGFR graphs are sent to clinicians
highlighting patients at an earlier stage so that appropriate
interventions to delay or halt deteriorating kidney function
can happen earlier.
• An smaller study at HEFT suggests this system may
significantly reduce the number of patients needing KRT
possibly saving £500K net after 5 years.