Hyperkalemia
advertisement

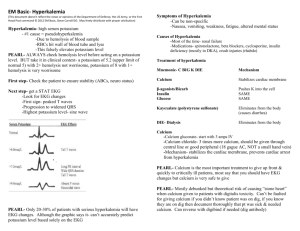
Hyperkalemia Objectives • • • • • • Definition Brief review of potassium regulation processes Causes Clinical Manifestations Therapy Proposals for standardized management Definition • Hyperkalemia = plasma K+ concentration > 5.0mmol/L • Critical hyperkalemia = plama K+ concentration > 6.5 mmol/L • UNM Lab Ranges: Normal 3.5-5.1 Critical 6.5 for women, 7 for men Potassium Regulation Review • Intracellular concentration about 150 mmol/L • The passive outward diffusion of K+ is the most important factor that generates the resting membrane potential. • Maintenance of steady state requires K+ ingestion = K+ excretion • Nearly all regulation of renal K+ excretion and total body K+ balance occurs in the distal nephron, via principal cells • Potassium secretion regulated by aldosterone and plasma K+ concentration Causes of Hyperkalemia I. Potassium release from cells II. Decreased renal loss III. Iatrogenic (Consider pseudohyperkalemia) Potassium release from cells • • • • • • • • • Intravascular hemolysis Tumor Lysis Syndrome Rhabdomyolysis Non-gap metabolic acidosis Hyperglycemia Severe Digitalis toxicity Hyperkalemic periodic paralysis Beta-blockers Succinylcholine; especially in case massive trauma, burns or neuromuscular disease Decreased renal loss • Renal failure • Decreased distal flow • Decreased K+ secretion Impaired Na+ reabsorption adrenal insufficiency adrenal enzyme deficiency hyporeninemic hypoaldosteronism drugs: ACEi, NSAIDS, heparin, K+-sparing diuretics, trimethoprim, pentamidine tubulointerstitial disease distal type 4 RTA Enhanced Cl- reabsorption Cyclosporine Gordon’s syndrome Clinical Manifestations • Weakness, which can progress to flaccid paralysis and hypoventilation. Secondary to prolonged partial depolarization from the elevated K+ , which impairs membrane excitability. • Metabolic acidosis, which further increases K+ Secondary to hyperkalemia impairing renal ammoniagenesis and absorption, and thus net acid excretion. • Altered electrical activity of heart, cardiac arrhythmias. ECG changes in order of appearance: Tall, narrow-based, peaked T waves Prolonged PR interval and QRS duration AV conduction delay Loss of P waves Progression of QRS duration leading to sine wave pattern Ventricular fibrillation or asystole Therapy 1. Determine needed approach – if emergent or not. Typically, potential fatal hyperkalemia occurs with K+ > 7.5 and associated with profound weakness. THIS CANNOT BE COUNTED ON; cardiac toxicity does not correlate well with plasma K+ concentration. MUST OBTAIN STAT ECG. 2. Determine underlying cause(s) once patient treated to maintain stability If K+ high and ECG normal, consider pseudohyperkalemia Usually, chronic hyperkalemia is due to impaired K+ excretion Review medications, oral and all IV therapies Evaluate effective circulating volume Patients with Kidney disease are highest risk of developing hyperkalemia. Consider the combination of: HCO3 <20, Cl- > 105, Cr > 1.5, diabetic as high risk for hyperkalemia. Emergent Therapy 1. 2. 3. 4. 5. 6. 7. 10 ml of a 10% solution calcium gluconate infused over 2-3 minutes. onset of action several minutes, lasts 30 – 60 minutes 10-20 units regular insulin with 25-50 g glucose IV onset action 15-30 minutes, lasts several hours. K+ drops 0.5-1.5 mmol/L. no glucose if patient hyperglycemic Nebulized or parental Beta-agonist onset action 30 minutes, lasts 2-4 hours. K+ drops 0.5 to 1.5 mmol/L. IV NaHCO3 as isotonic solution of 3 amps per liter 5% dextrose Ideally reserved for severe hyperkalemia associated with metabolic acidosis avoid in patients with ESRD; not tolerated and they seldom respond. Little medical evidence for use. Loop and thiazide diuretics if renal function adequate and not dehydrated Cation exchange resin, ie Kayexalate. 25-50 g mixed with 100 ml 20% sorbitol orally, or 30-60 min retention enema with 50 g resin in 150 ml H20. onset 1-2 hours and lasts 4-6 hours. K+ drops 0.5-1.5 mmol/L Dialysis Peritoneal is only 15% as effective as hemodialysis Algorithmic management of hyperkalemia. Sood M M et al. Mayo Clin Proc. 2007;82:1553-1561 © 2007 Mayo Foundation for Medical Education and Research Proposals for standardized management 1. 2. No treatment, other than kayexalate, for K 5.1 – 6 unless medical condition strongly predicts the value will continue to increase. Examples: acute oliguric renal failure, tumor lysis syndrome. Do repeat and f/u on potassium level. Policy that for any K+ > 6.0, order ECG. Consider stat repeat K+ if concern pseudohyperkalemia 3. 4. 5. 6. For persistent K+ > 5.1, order telemetry Policy if K+ <6.5 and no ECG changes present, treat with kayexalate and repeat K+ level and ECG in 4-6 hours. No need other interventions. Policy if K+ < 6.5 and ECG changes present, administer CaGluconate, Insulin/Glucose, Nebulizer Rx, and Kayexalate. Consider consult ICU team. Policy if K+ > 6.4, regardless of presence of ECG changes, administer CaGluc, Insulin/Glucose, Nebulizer Rx, and Kayexalate. Repeat ECG and K+ level in 1 hour. Consider consult ICU team. References 1. Harrisons Principles of Internal Medicine. 17th Edition. 2008. 2. Alfonzo, Annette V.M. Review paper: Potassium disorders-clinical spectrum and emergency management. Resuscitation (2006) 70, 10 -25. 3. Sood, Manish M. Emergency Management and Commonly Encountered Outpatient Scenarios in Patients With Hyperkalemia. Mayo Clinic Proc. 2007; 82(12): 15531561. 4. Tzamaloukas, A. Pathophysiology and Management of Fluid and Electrolyte Disturbances in Patients on Chronic Dialysis with Severe Hyperglycemia. Seminars in Dialysis. 2008; 21(5): 431-439.