Systemic Lupus Erythematosus:
A Review and Update
4th Annual Advanced Pharmacology Conference
Innovation and Advancement for the Future
April 15, 2011
INTEGRIS Baptist Medical Center
Joe Rawdon, MS RN ACNS-BC
Objectives
• At the conclusion of this activity, participants
should be able to:
– Identify key concepts in the pathogenesis, diagnosis,
and symptoms of Systemic Lupus Erythematosus.
– Discuss matters related to sub-optimal responses or
failures of agents used in the treatment of Systemic
Lupus Erythematosus.
– Describe the basis for standard-of-care therapies
including dosing, efficacy, safety and tolerability
profiles.
– Outline effective strategies for disease management
using current therapies.
Types of Lupus
•
•
•
•
Drug-Induced Lupus (DILE)
Cutaneous Lupus Erythematosus
Systemic Lupus Erythematosus (SLE)
Overlap Syndromes
– UCTD, Rheumatoid Arthritis, Sjogren’s Syndrome,
APLS, Polymyositis, Dermatomyositis, Scleroderma,
ITP
Drug-Induced Lupus
• A side effect of certain medications:
Hydralazine, Isoniazid, Methyldopa,
Minocycline, Procainamide, Quinidine,
Chlorpromizine
• Symptoms include rash, joint and muscle pain,
arthritis, flu-like symptoms, inflammation of
heart/lungs.
• Symptoms resolve when medication is stopped
D
T
M
WHAT CAUSES LUPUS?
B
complement
Systemic LUPUS
Brain Eyes
Parotid glands
Thyroid
Heart, Lungs
Serous linings of Heart, Lungs, GI tract
Kidneys
Liver
Spleen
Special Complications of Pregnancy
Joints
Blood Vessels
and Blood Proteins
Inflammation vs.
Coagulation
Inflammatory multisystem disease
Skin
Highly variable from patient to patient
Waxing and Waning
Significant constitutional symptoms
Associated with characteristic autoantibodies
Serious Sequelae *
early: disease activity
late: therapy complications and disease damage
Antibiotics:
20th Century Miracle Drugs
Lupus
• Not an Infection
• There is no cure for SLE
• But there is one small population with lupus
we can cure!
Congenic Dissection of Lupus Pathogenesis
1 3
2
NZM2410
Lupus-prone
B6
Lupus-resistant
1
B6.Sle1
2
B6.Sle2
3
B6.Sle3
Loss in immune
B cell hyperactivity T cell activation and
tolerance to chromatin
decreased apoptosis
Mohan et al., J. Immunology, 1998
Mohan C, et al. J Clin Invest. 1998;101:1362-1372.
Re-assembly of Lupus Pathogenesis by
various combinations of congenic intervals
1
2 3
>90% Fatal
lupus
B6.Sle1,2,3
1
B6.Sle1
2
1 2
~15%
Fatal
lupus
Re-assembly of
congenic intervals
B6.Sle2
3
B6.Sle3
Morel et al. PNAS 97:6670-6675, 2000
B6.Sle1,2
1 3
~50% Fatal
lupus
B6.Sle1,3
2 3
B6.Sle2,3
0% Fatal
lupus
HUMANS ARE NOT MICE
20
12
IL10
15
IL8
10
8
6
10
4
Bioplex Units
5
2
0
0
P1
P2
P3
P4
P5
300
250
IFN ALPHA
200
150
100
50
0
P1
P2
P3
P4
P5
P1 P2 P3 P4 P5 P6
P6
P6
160
140
120
100
80
60
40
20
0
TNF ALPHA
P1 P2 P3 P4 P5 P6
Six Lupus Patients with “Arthritis”
D
INF alpha
B1
Make
antibodies
IFN-
Activate
other cells
Make
inflammatory
Proteins
B
T
Adapted from: Ramanujam M, Davidson A. Arthritis Research and Therapy 2004; 197
IMPROVED SURVIVAL IN SLE: 1955-1990
%
The Major Difference has been due to Steroids
YEARS
Wallace in Arthr and Allied Cond, 13th Ed V2, p1319 Koopman, ed
Epidemiologic Data Based on SLE Cause of Death
TLR inhibitors
D
INF alpha inhibitors
Riquent, Edritide
IFN-
B
Anti IL6
Cellcept
RITUXIMAB
Ocrelizumab
Epratuzumab
IDEC 131
Biogen product
ABATACEPT
Anti-ICOS
BENLYSTA, Other BLys and BLys/April inhibitors
TNF inhibitors
T
Treatment: Medications
• Non‐steroidal anti‐inflammatory drugs (NSAIDs)
• Topical steroids
• Systemic steroids
• Antimalarial drugs
•Plaquenil (hydroxychloroquine)
• Aralen (chloroquine)
•Atabrine (quinicrine)
Plaquenil (hydroxychloroquine)
• Used to treat malaria, lupus, and inflammatory arthritis
• Decreases autoimmune activity
• Helpful for rash, arthritis, and fatigue
• Typical dose is 200mg twice a day
• Baseline eye exam and exam every 6‐12 months
• GI upset is common
• May take months for full effect
Treatment: Medications
Disease Modifying/Cytotoxic Agents
•Imuran (azathioprine)
•Cellcept (mycophenolate mofetil)
•Rheumatrex or Trexall (methotrexate)
•Arava (leflunomide)
•Cytoxan (cyclophosphamide)
•Sandimmune and Neoral (cyclosprine)
BENLYSTA (belimumab)
• recognize and inhibit the biological activity of
B-lymphocyte stimulator (BLyS)
• 10 mg/kg at 2-week intervals for the first 3
doses and at 4-week intervals thereafter
• IV over 1 hour, no premedication necessary
SLE Classification: ACR Criteria
8 CLINICAL
Malar rash (rash on cheeks that spares the naso-labial folds)
Discoid rash (anywhere on body)
Photosensitivity
Oral or nasal ulcers
Arthritis (nonerosive arthritis of two or more peripheral joints,
with tenderness, swelling, or effusion)
Serositis (Pleurisy or pericarditis)
Renal Disorder (0.5 g protein in urine or cellular casts)
Neurologic Disorder (seizures or psychosis)
Definite diagnosis of SLE: 4 of 11 criteria present
SLE Classification: ACR Criteria
3 LABORATORY
Low blood cell counts
Leukopenia (<4000/ µl)
Lymphopenia (<1500/µl)
Hemolytic anemia
Thrombocytopenia (<100,000/µl)
Antinuclear antibodies
Specific autoantibodies
anti-DNA, anti-Sm, or antiphospholipid family
Definite diagnosis of SLE: 4 of 11 criteria present
Autoantibodies in SLE
• ANA
•
•
•
•
•
Seen in 95% of SLE
Not specific for SLE
Seen in many
inflammatory,
infectious, and
neoplastic diseases
Seen in 5% to 30% of
normal persons
Common is people over
60, liver disease,
changes frequently
from lab to lab.
ANA Titers in Normal Individuals
with no clinical consequence
1:40
20-30%
1:80
10-12%
1:160
5%
1:320
3%
Autoantibodies in SLE
• Anti-ds DNA
•
•
•
•
Seen as high as 60% of populations with SLE
Highly specific for SLE
Low titer rarely seen in other inflammatory
conditions
Strongest clinical association is with nephritis
• Anti-Sm (Smith)
•
•
Seen in 10% to 30% of SLE patients
Highly specific for SLE
WHAT TESTS HELP?
• CBC
– Leukopenia, lymphopenia, neutropenia,
– Thrombocytopenia
– Coombs + LHD (hemolytic anemia)
• CHEM SCREEN
– Renal (BUN, creatinine, albumin)
– Hepatitis (SGOT/SGPT)
• URINALYSIS
– Renal, urine prot/creat ratio
WHAT TESTS HELP?
• ANA
– Ro and La
– Sm and RNP
– Anti-dsDNA (anti-ssDNA, anti-histone)
• ANTIBODIES TO TARGET ORGANS
– Anti-phospholipid family
– white blood cells, brain, kidneys, placenta
THE COMPLEMENT STORY
Low C3
Low C4
Low CH50
Low C2
Y
YY
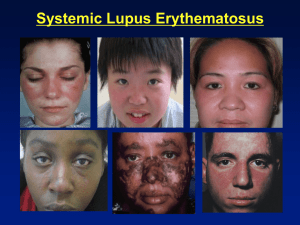
Systemic Lupus Erythematosus
• Clinical symptoms related to the degree of
inflammation in various organs
•
•
•
•
•
•
•
Skin and mucous membranes
Arthritis or arthralgia
Hematologic involvement
Kidneys
Fevers
30 - 60%
55 - 90%
50%
5%
5%
ACR recommends early referral after 1st signs
suggesting SLE.
Minimum recommended follow-up is every 3 months.
Disease Tracking
Disease Tracking
Lupus and pregnancy
• Fertility of lupus patients is similar to the general population
• Patients with lupus are considered high-risk
• Preferred - Lupus should be under control (ideally for 6 months) before getting pregnant
• Pregnancy does not increase the risk of lupus flares
• Neonatal lupus occurs in 1-2% of pregnancies
mild malar rash to heart block
•Ro and La Antibodies
•ACL antibodies –
•Hypertension, edema, pre-eclampsia, miscarriage, early delivery, low birth weight
• Some medications taken for lupus are probably safe to take during pregnancy
OC-SELENA trial http://www.nejm.org/doi/full/10.1056/NEJMoa051135
When to Consider a Diagnosis of SLE
•Women of childbearing age
who present with:
•
•
•
•
•
Constitutional symptoms of fever, weight loss,
malaise, and severe fatigue
Skin rash and/or stomatitis
Arthritis – most common presenting feature
Renal disease
Cytopenias
When to Consider a Diagnosis of SLE
• Genetic predisposition
– Most cases are sporadic but may cluster in families
– 5-12% have family member with SLE
– Lupus is polygenic (more that one gene responsible)
• Although 90% of patients are female, SLE can be seen at any age in
either sex
•
1,000,000 to 2,000,000 Americans have lupus
(.012-.05% of the population)
•
More common in African American and Asian populations
The End….or other slides if there’s
time.
Pericardial Involvement in SLE
25% incidence of evident pericarditis
50% incidence of pericardial effusion
80% incidence of pericardial abn at autopsy
Libman Sacks Endocarditis
in up to 43% of patients by TEE
(nonbacterial thrombotic endocarditis)
Prevalence of Lupus vs Other Diseases
( in USA x 1000)
JDRF Society
Nat Inst Neur Dis and Stroke
Lupus Foundation of America
Susan Komen Foundation
Disease-Specific Funding per Year
(normalized to patient numbers)
Millions/year/pt
www.nih.gov.news
Lupus in People From Different
Genetic Backgrounds: Risk is not Destiny
35
30
25
Caucasian
n=185
Native Amer
n=40
African Amer
n=67
20
15
10
5
0
anti- discoid
dsDNA
renal
SLE Genes: Ethnic Differences
GENE
CAUC
AFR
references
TNF alpha
X
Hum Immunol 65:622
16q12-13
X
X
X
E J Hum Gen 12:668
12q24
FcgRIIIa
FcgRIIa
11p13 (discoid)
NO synth prom
FasL 1q23
Am J Hum Gen 74:73
Rheum (Ox) 42:446
X
X
X
X
J Clin Invest 95:1348
J Inv Derm Sym 9:64
J Rheum 30:60
J Immun 170:132