A collaboration led by
Interact2:
Background and Rationale
Acute intracerebral haemorrhage (ICH)
Accounts for:
~10-15% of strokes in Western countries
(Feigin et al 2003)
~20-40% in African, Asian & Latin American
populations (Zhang et al 2003, Saposnik et al 2003)
The most lethal type of stroke
No proven effective medical treatment
Continued controversy over role of surgery
Hypertension in ICH
Most important risk factor for both
incident and recurrent ICH
Consistent determinant of poor outcome
Uncertain benefits of therapeutic blood
pressure (BP) lowering
Emerging evidence of safety and
potential efficacy
Near linear BP – ICH outcome associations
in a Japanese clinical cohort
n = 1097
Okumura et al, J Hypertension 2005; 23: 1217-23
Systolic BP levels strongly associated with death
and disability in ICH; reverse for ischaemic stroke
Ischaemic stroke
(n=2178)
Zhang et al. J Hypertension 2008; 26: 1446-52
ICH stroke
(n=1760)
Theoretical adverse effects of rapid BP
lowering in the brain
Impaired cerebral blood
flow autoregulation
Adverse effects on
perihaematoma ‘ischaemia’
Less potential hazard of rapid BP lowering in
ICH compared with ischaemic stroke
Perihaematoma oedema is not an ischaemic penumbra
Imaging studies indicate perihaematoma oedema is
plasma derived
Various cerebral perfusion studies confirm
safety of BP lowering on cerebral circulation
PET
Powers et al
Neurology 2001
TCD
Dyker, A. G. et al
Stroke 1997
Xe-CT
Butterworth et al
Cerebrovasc Dis 2001
Willmot et al
Hypertension 2006
INTERACT – Pilot Study
Lancet Neurology 2008; 7:391-399
INTERACT
Aimed to determine if early intensive BP lowering is:
feasible
safe
attenuates haematoma expansion
Sample size (n=400) provided 80% power to detect
17% (≥60% reduction in relative risk) minimum
absolute difference in proportional mean haematoma
growth between randomised groups, assuming 30%
(SD60) mean growth in guideline group.
Blood Pressure Management
Study evaluated a management policy and NOT of
a single agent
Pragmatic approach to treatment
Agents used are those available in hospitals
Agents that are approved for clinical use
Lower study costs versus packaging and use of placebo
BP management protocols provided to
standardise therapies across countries
INTERACT1 Protocol Schema
Acute spontaneous ICH
onset < 6 hours
SBP ≥ 150 and ≤ 220 mmHg
No definite indications or contraindications to treatment
Able to be actively managed
Provide informed consent
R
Standard
best
practice
stroke unit
care
Intensive BP lowering
Target systolic BP 140 mmHg
within 1 hour and for 24+ hrs
Standard BP management
AHA Guideline-based
(treatment if systolic BP >180 mmHg)
Repeat CT scans 24 and 72 hrs
Vital signs and BP over 7 days
In-person 28 day and 3 month follow-up
Measurement of haematoma parameters
Repeat CTs at 24 and 72 hrs
DICOM digital CT images sent
to central core lab (Sydney)
Multi-slice planimetric
technique using MIStar 3.2
software (Melbourne, Aust)
Analysed by 2 neurologist
readers blind to clinical, centre,
treatment and time of CT data
Inter-reader on 10% of CTs
(ICC 0.97 ICH volume)
INTERACT Patient Flow
Patient characteristics
Standard
(n = 201)
Intensive
(n = 203)
3.4 (2.5-4.5)
3.4 (2.5-4.5)
62 13
63 12
Gender (male)
69%
61%
China
95%
95%
Systolic BP (mean SD)
182 19
180 18
Diastolic BP (mean SD)
105 15
101 14
79
79
9 (5-16)
9 (5-14)
14 (12-15)
14 (13-15)
History of hypertension
74%
74%
Use of antihypertensives
45%
42%
Deep location of hematoma
84%
83%
Time to randomization,
hr:min median (IQR)
Age (mean SD), yrs
Heart rate
NIHSS, median (IQR)
GCS, median (IQR)
Therapies and management
Standard
(n = 201)
Intensive
(n = 203)
Any blood pressure lowering
74%
98%
Method - bolus
48%
58%
66%
73%
34%
66%
9%
7%
Intravenous fluids
98%
98%
Fever treated
39%
36%
Nasogastric feeding
21%
20%
Intravenous mannitol
86%
82%
Neurosurgery intervention
7%
7%
Use of FFP or vitamin K
5%
3%
Use of rFVIIa
3%
6%
- infusion
Single iv agents
Intubation
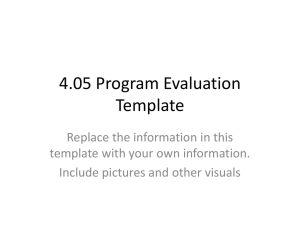
INTERACT - Mean (95%CI) systolic BP
differences between randomised groups
0-1 hr
1-24 hrs
2-7 days
28 + 90
days
Δ 14 mmHg at 1 hour (P<0.0001)
Δ 10.8 mmHg 1-24 hours (P<0.0001)
15m 145m
6h
18h 24h 2d
3d
4d
5d
6d
7d
28d
90d
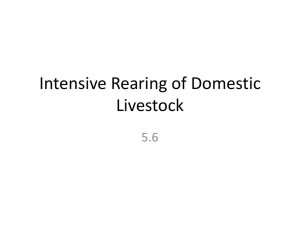
INTERACT – Adjusted* mean (95%CI) values for
absolute and relative increase in haematoma volume
6
P=0.13
P=0.06
20
4
ml
30
10
2
%
0
0
Δ-1.7ml
-2
Δ-10%
-5
*Adjusted for age, sex, haematoma location, baseline haematoma volume, time from onset to CT.
Anderson et al. Lancet 2008; 7: 391-399
INTERACT - Effects of early intensive BP lowering on haematoma
(n=296) and perihaematoma oedema (n=270) over 72 hours
Anderson et al. Stroke 2010; 41: 307-321
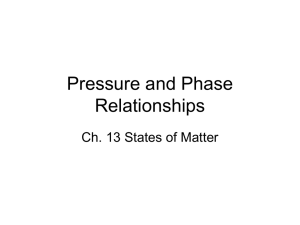
INTERACT - Absolute increase in haematoma
volume for tertiles of systolic BP, by baseline and
achieved levels
Absolute increase (ml)
8
8
6
6
4
4
2
2
0
0
P trend=0.26
P trend=0.03
-2
-2
150 160 170 180 190 200 210 120 130 140 150 160 170 180
Baseline SBP (mmHg)
Achieved SBP (mmHg)
Adjusted for age, sex, haematoma location, baseline haematoma volume, time from onset to CT, and study treatment.
21
Arima et al. J Hypertension 2010; 56:852-858
INTERACT – Relative increase in haematoma volume for
Proportional increase (%)
tertiles of systolic BP, by baseline and achieved levels
50
50
40
40
30
30
20
20
10
10
P trend=0.12
P trend=0.03
0
0
150 160 170 180 190 200 210 120 130 140 150 160 170 180
Baseline SBP (mmHg)
Achieved SBP (mmHg)
Adjusted for age, sex, haematoma location, baseline haematoma volume, time from onset to CT, and study treatment.
Arima et al. J Hypertension 2010; 56:852-858
INTERACT: Reduction in absolute hematoma growth
over 72 hours according to time from onset to treatment
Time from onset Absolute growth
Time from onset
toto
treatment
IntensiveGuideline
Guideline
Intensive
treatment
Reduction
in
intensive guideline Volume
Favors Favors
<2.9h
-4.4 ml
2.1 ml
6.5 ml
2.9-3.6h
0.1 ml
3.4 ml
3.3 ml
3.7-4.8h
-1.1 ml
-0.2 ml
0.9 ml
≥ 4.9h
-0.2 ml
0.4 ml
0.6 ml
0
10
5
-5
15
Reduction in hematoma growth over 72h (ml)
Unpublished data
Interact: Reduction in relative hematoma growth over 72
hours according to time from onset to treatment
Time from
Time from onset
onset
to treatment
P for
Relative growth
Reduction
P for
In
trend
trend
intensive guideline
volume
Favors Favors
Intensive Guideline
<2.9h
-10%
10%
21%
2.9-3.6h
16%
31%
15%
3.7-4.8h
-6%
1%
7%
≥ 4.9h
19%
22%
4%
0
20
10
-10
30
Reduction in hematoma growth over 72h (%)
Unpublished data
0.02
Adverse effects (90 days)
Standard
(n = 201)
Intensive
(n = 203)
p
Neurological deterioration to 72 hrs
15
15
0.94
Serious adverse events
21
21
0.40
2
1
1
1
14
11
Renal failure
1
2
Non-vascular
10
8
Pneumonia
7
5
Other
2
3
Mild hypotension
0
1
Severe hypotension
2
1
Recurrent stroke
Other vascular event
Reported neurological deterioration
Clinical outcomes (90 days)
Standard
(n = 201)
Intensive
(n = 203)
p
Death or dependency
49
48
0.81
Death
12
10
0.51
Dependency
41
36
0.98
Modified Rankin Score, median
2
2
0.66
NIHSS, median
2
2
0.97
Barthel Index Score, median
95
95
0.77
MMSE, median
28
27
0.97
EuroQoL, EQ5D, median, %
78
75
0.97
Conclusion
INTERACT1 shows consistency of the BP lowering
treatment effect across various different analyses
BP lowering on haematoma growth at 24 and 72
hours
Haematoma rather than perihaematoma oedema
is the principle therapeutic target
Lower BP levels (140-150 mmHg) are likely to
produce greater benefits
Early BP lowering are likely to produce greater
benefits
Conclusion (cont.)
Early rapid BP lowering is:
clinically feasible
not associated with excess hazard
appears to reduce haematoma expansion
However, some limitations:
single study, mainly Chinese participants
potential play of chance
no effect on clinical outcomes, as in rFVIIa
studies
Conclusion (cont.)
Recommendations
1.Until ongoing clinical trials of BP intervention for ICH are completed,
physicians must manage BP on the basis of the present incomplete efficacy
evidence. Current suggested recommendations for target BP in various
situations are listed in Table 6 and may be considered (Class IIb; Level of
Evidence: C). (Unchanged from the previous guideline)
2.In patients presenting with a systolic BP of 150 to 220 mmHg, acute lowering
of systolic BP to 140 mmHg is probably safe (Class IIa; Level of Evidence: B).
(New recommendation)
Summary
INTERACT shows that early intensive BP lowering
with careful monitoring is:
feasible, safe, and attenuates hematoma growth
As antihypertensive agents are inexpensive and widely
available
widespread adoption of a standard policy could
translate into high absolute benefits
A large-scale trial powered to evaluate modest but still
worthwhile effects on clinical endpoints is required to
influence clinical practice
Acknowledgements
Patients and families
Participating hospitals and staff
Many project staff in multiple countries
Funding:
National Health and Medical Research
Council of Australia
The George Institute for Global Health
Acknowledgements
Executive committee: Craig Anderson (Principal Investigator), John Chalmers (Chair),
Hisatomi Arima, Stephen Davis, Emma Heeley, Yining Huang, Richard Lindley, Bruce Neal,
Mark Parsons, Christian Stapf, Christophe Tzourio and Jiguang Wang.
China steering committee: Yining Huang, Jiguang Wang, Liying Cui, Shengdi Chen,
Zhenguo Liu, Chuanzhen Lu, Qidong Yang, En Xu, Jingfen Zhang, Chaodong Zhang,
Shizheng Wu and Xining Yan Chen
European advisory board: Austria – Ronny Beer, Erich Schmutzhard; Belgium – Patricia
Redondo; Finland – Markku Kaste, Lauri Soinne, Turgut Tatlisumak; France – Christian
Stapf, Christophe Tzourio, Eric Vicaut; Germany – Katja Wartenberg; Italy – Stefano Ricci;
Netherlands – Karin Klijn; Portugal – Jose´ Ferro; Spain – Angel Chamorro; Switzerland –
Marcel Arnold, Urs Fischer; UK – Tom Robinson.
Operations committee: Emma Heeley, Candice Delcourt.
International coordinators: Michelle Leroux, Tara Sasse, Jun Hata, Gouyjen, Tina
Cheung, Cathy Boreham, Sarah Leighton.
Regional coordinators: Americas – Alejandro Rabinstein; Argentina – Conrado J. Estol,
Mariana Zimmermann; Brazil – Gisele Silva, Joyce Marinho; Chile – Pablo Lavados; China –
Jian Sun, Nan Li, Zhao Yan, Chen Xiaoying; France – Sofiane Kabla, Cecile Dert; India –K
Mallickarjuna, Najam Hassan, Jeyaraj Pandian.
DSMB members: John Simes (Chair), Marie-Germaine Bousser, Graeme Hankey, Konrad
Jamrozik (deceased in 2010), Claiborne Johnston and Li Shunwei.
Statisticians: Laurent Billot, Stephane Heritier and Qiang Li.