Click here to this slideshow
advertisement

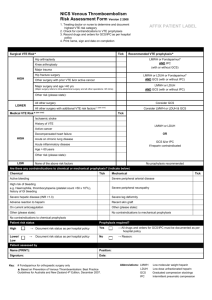
Prevention Of Venous Thromboembolism In The Cancer Surgical Patient A K Kakkar Barts and the London School of Medicine and Thrombosis Research Institute, London UK Incidence Of VTE In Cancer Surgical Patients VTE no malignancy (%) VTE malignancy (%)* Neurosurgery 0.5–2.3 2.0–3.6 Head and neck 0.1–0.2 0.2–1.4 Gastrointestinal 0.2–1.6 0.9–2.6 Urological 0.3–1.0 0.4–3.7 0.3 1.2–2.3 0.2–2.4 0.9–3.1 Surgical procedure Gynaecological Orthopaedic *Symptomatic VTE at 91 days in patients after surgery. Adapted from White et al. Thromb Haemost. 2003;90:446-55. Impact Of Cancer On PE Frequency Cancer No Cancer OR Surgical (%) 2.34 0.36 6.7 Non surgical (%) 0.73 0.10 7.3 Total 1.84 0.27 6.8 Adapted from Huber et al. Arch Surg 1992;127:310-3. Prognostic Risk Factors For VTE In Cancer Variable Age Previous VTE Anaesthesia Stage Bedrest No. of patients VTE / non-VTE Effect ≥ 60 yrs: 42 / 1,516 ≥ 60 vs < 60 years < 60 yrs: 8 / 807 Yes: 5 / 36 Yes vs no ≥ 2 vs < 2 hours Advanced vs No: 45 / 2,287 ≥ 2 hours: 48 / 1,762 < 2 hours: 2 / 561 OR 95 % CI 2.6 1.2–5.7 6.0 2.1–16.8 4.5 1.1–19.0 2.7 1.4–5.2 4.4 2.5–7.8 Advanced: 38 / 1,078 not advanced ≥ 4 vs < 4 days Adapted from Agnelli et al. Ann Surg 2006; 243:89-95. Non advanced: 12 / 1,245 ≥ 4 days: 25 / 346 < 4 days: 25 / 1,977 Prophylaxis Against Fatal PE With Low-dose UFH International Multicenter Trial 4121 patients undergoing major surgery Primary end point: fatal PE Randomized: control or UFH (5000 IU 2 hours before surgery and every 8 hours postoperatively for 7 days) 180 patients died during the postoperative period: 100 in the control group and 80 in the UFH group Rate of autopsy was 72 % in control group and 66% in the heparin group Adapted from Kakkar et al. Lancet 1975;2:45-51. Prophylaxis Against Fatal PE With Low-dose UFH P<0.005 18 16 Number of patients with fatal PE 16 14 12 10 8 6 4 2 2 0 Control Adapted from Kakkar et al., Lancet 1975;2:45-51. UFH Fatal Post-operative PE In Patients With Cancer Patients with PE, % 23% (n = 953) underwent operation with malignant disease Adapted from Kakkar et al. Lancet 1975;2:45-51. Heparin Prevents Death After Surgery 21% reduction in total surgical mortality 68% reduction in fatal PE 67% reduction in asymptomatic DVT Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration of subcutaneous heparin Adapted from Collins et al. New Engl J Med 1988;318:1162-73. Death From PE But Not From Bleeding “Other” deaths PE 191 (3.0%) (1.7%) 109 Fatal bleeds (0.9%) (0.3%) 7 Adapted from Collins et al. N Engl J Med 1988;318:1162-73. 6 Low Dose vs. LMW Heparin Canadian Colorectal DVT Prophylaxis Trial Incidence of Outcome Event 16.9% P=0.05 N=234 13.9% N=241 1.5% 2.7% N=653 N=643 VTE (Cancer) Adapted from McLeod et al. Ann Surg 2001;233:438-44. Major Bleeding (All) Thromboprophylaxis In Cancer Surgery P=0.001 LMWH once daily – Dalteparin 2500 IU vs 5000 IU daily – Total duration 7 days Therapy commenced preoperatively DVT in Patients With Malignancy (%) Prospective, randomized, doubleblind multicenter trial 2070 patients randomized 67% (1303/1957) malignancy Bleeding complications in patients operated on for malignant disease occurred in 3.6% of those receiving dalteparin 2500 IU and 4.6% of those receiving dalteparin 5000 IU (P=NS). Adapted from Bergqvist et al. Br J Surg. 1995;82:496-501. Thromboprophylaxis In The Cancer Surgical Patient LMWH better UFH better Asymptomatic DVT Clinical PE Clinical thromboembolism Cancer Death Non-cancer Major hemorrhage Total hemorrhage Wound hematoma Transfusion 0 Adapted from Mismetti et al. Br J Surg 2001;88:913–30. 1.0 2.0 3.0 4.0 Effects Of Compression Methods of Thromboprophylaxis On DVT Category (a) No. of Deep venous trials thrombosis with data Compression Control Compression (monotherapy) Graduated 9 compression stockings Intermittent 19 pneumatic compression Footpump 2 30 99% or 57/665 (8.6%) 112/1108 (10.1%) 11/61 (18.0%) 180/1834 (9.8%) 95% confidence intervals 133/627 (21.2%) 268/1147 (23.4%) 34/65 (52.3%) Stratified statistics O–E Variance Odds ratio and confidence interval (compression : control) % odds reduction (SE) –39.7 37.2 66% (10) –76.3 71.0 66% (7) –10.7 7.3 77% (19) 435/1839 –126.7 115.5 (23.7%) 67% (6) 2p < 0.00001 0.0 0.5 1.0 Compression better 1.5 Compression worse Treatment effect 2p < 0.00001 Adapted from Roderick et al. Health Technology Assessment 2005; Vol. 9: No. 49. 2.0 Effects Of Compression Methods of Thromboprophylaxis On PE Category No. of Deep venous trials thrombosis with data Compression Control (a) Compression (monotherapy) Graduated 3 compression stockings Intermittent 8 pneumatic compression(2.4%) Footpump 1 12 99% or 0/123 (0.0%) 14/590 (2.9%) 0/28 (0.0%) 4/90 (4.4%) 18/618 14/741 (1.9%) 22/740 (3.0%) 95% confidence intervals Stratified statistics O–E Variance –1.8 0.9 –1.6 7.6 –3.4 8.5 Odds ratio and confidence interval (compression : control) % odds reduction (SE) 0/32 (0.0%) 0.0 33% (28) 2p > 0.1; NS 0.5 1.0 1.5 Compression Compression better worse Treatment effect 2p = 0.006 Adapted from Roderick et al. Health Technology Assessment 2005; Vol. 9: No. 49. 2.0 Combined Mechanical and Pharmacological Prophylaxis Intervention 6 studies LDH (n=451) LDH+GCS (n=439) RR (95%CI) DVT n (%) 83 (18) 35 (%) 0.47 0.33-0.69 Adapted from IUA Consensus statement Int Angiol 2006. Prevention Of Fatal PE In Surgical Patients P=NS Low-dose heparin t.i.d. Adapted from Haas et al. Thromb Haem. 2005;94:814-9. LMWH o.d. Cancer Patients Are At Higher Risk For PE Surgical Population All Patients* Cancer (n=6,124) No Cancer (n=16,954) P Value Death (%) 192 (3.1) 120 (0.7) 0.0001 Fatal PE (%) 20 (0.33) 15 (0.09) 0.0001 Nonfatal PE (%) 5 (0.08) 4 (0.02) *Receiving UFH or LMWH. Adapted from Kakkar et al. Thromb Haemost. 2005;94:867-71. PE Occurs After Hospital Discharge In-hospital PE (n=80) After-discharge PE (n=24) 0 4 8 12 16 Adapted from Huber et al. Arch Surg 1992;127:310-3. 20 24 28 32 36 Days ENOXACAN II: Design 7 Days Enoxaparin (40mg sc od)* ® 21 Days Enoxaparin (40mg sc od) n= 165 Placebo n=167 Major abdominal surgery * Pre-op dose Adapted from Bergqvist et al., New Engl J Med 2002;346:97580. Bilateral venography ENOXACAN II: Results 332 patients undergoing surgery for abdominal or pelvic tumours received enoxaparin (40 mg daily) for 1 week followed by enoxaparin or placebo for another 21 days Venography was performed at 30day and 3-month follow-up At each follow-up, prolonged TP was associated with a 60% risk reduction for DVT 20 RRR, 60%; P=0.02 15 13.8% 12.0% 10 5 4.8% 5.5% 0 Day 30 3 month Follow-up Placebo (n=167) Adapted from Bergqvist et al., N Engl J Med 2002;346:97580. RRR, 60%; P=0.01 Enoxaparin (n=165) FAME: Design 7 Days ® Dalteparin (5000 IU sc od)* + TED 21 Days Dalteparin (5000 IU sc od) No further prophylaxis Major abdominal surgery *Pre-Op dose TED: graduated compression stockings Adapted from Rasmussen et al., J Thromb Haemost 2006 4: 2384–90. Bilateral venography (assessor-blinded) FAME: Results The ITT population consisted of 178 patients in the short-term prophylaxis group and 165 in the prolonged prophylaxis group Venography was performed on day 28 Prolonged TP was associated with a 55% risk reduction for VTE and 77% risk reduction for proximal DVT RRR, 55% P=0.012 20 RRR, 77%; P=0.009 16.3% 15 8.0% 10 7.3% 5 1.8% 0 VTE Proximal DVT Dalteparin 4 weeks 1 week Adapted from Rasmussen et al., J Thromb Haemost 2006 4: 2384–90. Extended Thromboprophylaxis: Meta Analysis 4 studies: 2 double-blind and 2 open 1,037 patients Bilateral venography 7–10 days DVT 15% 4–5 weeks p 6.5% < 0.0005 < 0.01 Proximal DVT 5% 1% Symptomatic DVT 1% 0.3% Adapted from Rasmussen et al. J Thromb Haemost 2005; 3 Suppl 1:P2213. 0.27 ESMO Clinical Recommendations Should Patients With Cancer Undergoing Surgery Receive Thromboprophylaxis? 1. Prophylaxis with LMWH (3400 - 5000 U once daily) or UFH (5000 U three times daily) is recommended. [I, A]*. 2. Cancer patients undergoing elective major abdominal or pelvic surgery should receive post-discharge prophylaxis with LMWH for up to 1 month after surgery [I, A]*. * Levels of evidence [I–V] and grades of recommendation [A–D] as used by the American Society of Clinical Oncology. ASCO VTE Guideline Should Patients With Cancer Undergoing Surgery Receive Thromboprophylaxis? 1. All patients undergoing major surgical intervention for cancer should be considered for thromboprophylaxis. 2. Patients undergoing laparotomy, laparoscopy, thoracotomy lasting greater than 30 minutes should receive pharmacological thromboprophylaxis with UFH or LMWH unless contraindicated. 3. Commenced preoperatively. ASCO VTE Guideline Should Patients With Cancer Undergoing Surgery Receive Thromboprophylaxis? 4. Mechanical methods may be added to pharmacological methods but should not be used as monotherapy for VTE prevention unless pharmacological methods are contraindicated because of active bleeding 5. Combined pharmacological and mechanical prophylaxis may improve efficacy especially in the highest risk patients 6. Prophylaxis should be continued for at least 7 - 10 days postoperatively. Prolonged prophylaxis for up to 4 weeks after major abdominal and pelvic surgery in patients with high risk features such as residual disease, obesity, and previous history of VTE Conclusions VTE common after cancer surgery. Prophylaxis with LMWH effective and safe. Extended prophylaxis should be considered for highest risk populations.