Introduction to Thoracic Radiology
advertisement

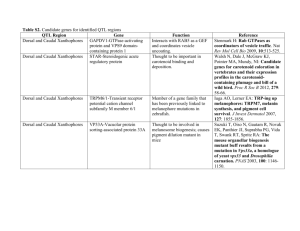
Introduction to Thoracic Radiology Dr. Meghan Woodland September 30, 2010. Indications • • • • Coughing Dyspnea / Tachypnea Heart Murmur, Collapse Primary or Secondary Neoplasia – Check for metastasis • Thoracic Trauma • Chest Wall Mass • Exercise Intolerance, Weight Loss Technical Factors • Potential for Movement – Respiration – Decrease mAs • High inherent contrast – High kVp • Collimation – Should include thoracic inlet to diaphragm • Center over the heart • Pull thoracic limbs forward Radiographic techniques: the dog By Joe P. Morgan, John Doval, Valerie Samii Determining the Phase of Respiration • Always expose at peak inspiration – Maximizes lung contrast – Better visualization of pulmonary parenchyma – Less compression of lungs by diaphragm • Inspiratory lateral view: – Caudodorsal aspect of lung is caudal to T12 – Increased aeration of accessory lung lobe – Separation of cardiac silhouette and diaphragm • Inspiratory VD/DV view: – Diaphragmatic cupola caudal to mid-T8 – Tips of lung caudal to T10 Inspiratory vs. Expiratory Lateral Notice size of triangle Inspiratory vs. Expiratory VD Easy to see the difference in well visualized lung DV vs. VD • DV – Best view to evaluate cardiac silhouette and caudal pulmonary vessels – Less stressful for the patient – Diaphragm rounded – See small amounts of pleural air • VD – – – – Best view to evaluate lungs Heart appears elongated Flat diaphragm – Mickey Mouse ears See small amounts of pleural fluid DV VD DV vs. VD Right vs. Left Lateral • Caudal Vena Cava enters the right diaphragmatic crus • Right Lateral – Better cardiac detail – R crus forward • See CVC go into it • Left Lateral – Heart appears round – L crus forward • See Cava go past Caudal vena cava Left or Right Lateral? Left or Right Lateral? The Effects of Lateral Recumbency • Lung lesions (mass, nodule, infiltrate) may only be seen on a single view • Only the non-dependent (up) lung can be critically evaluated – Dependent lung loses aeration (atelectasis) • Increased opacity • Silhouettes with lesions Sedation Induced Atelectasis Interpretation of Thoracic Radiographs • • • • • • • Systematic approach is crucial Heart (Cardiac Silhouette) Lungs Mediastinum Pleural space Chest wall Bones, Abdomen, Neck Normal Cardiac Silhouette • Size is subjective • Lateral views: – Dog = 2 ½ - 3 ½ intercostal spaces – Cat = 2 – 2 ½ intercostal spaces • VD/DV views: – 65% the width of the thorax • Objective: – Buchanan method • Vertebral heart scale Clock Face • • • • • • • 11-1 Aortic Arch 1-2 Main Pulmonary Trunk 2-3 Left Auricle 2-5 Left Ventricle 5-9 Right Ventricle 9-11 Right Atrium Centrally – Left Atrium Lateral View • Make a Plus sign • Bermuda triangle – Right atrium – Main pulmonary artery – Aortic Arch • Left atrium • Left Ventricle • Right Ventricle Thoracic and Pulmonary Vessels • Aorta • Caudal Vena Cava • Cranial pulmonary vessels – Proximal third rib • Caudal pulmonary vessels – Where crosses 9th rib • Veins are ventral and central – Artery, bronchus, vein – ABV’s Trachea, Bronchial Tree • Trachea ends at the carina • Then splits to the main stem bronchi followed by the lobar bronchi • Tracheal rings can mineralize (age) • Decreased tracheal diameter – Tracheal narrowing (stenosis, extramural compression) – Tracheal hypoplasia – Tracheal collapse Lungs • Normal anatomy 1 – Left • Cranial (cranial subsegment) 1 • Cranial (caudal subsegment) 2 • Caudal 3 – Right • • • • Cranial 4 Middle 5 Caudal 6 Accessory 7 4 2 5 3 6 7 The Mediastinum • Cranial, middle, caudal compartments • Routinely visible structures: – Cardiac silhouette, trachea, caudal vena cava, aorta, +/- thymus, +/- esophagus – Cranioventral mediastinal reflection – Caudoventral mediastinal reflection • Aka phrenopericardiac ligament • Left side on VD radiograph Mediastinal Reflection Caudoventral mediastinal reflection Extrathoracic Structures • • • • Sternum Vertebrae Ribs Adjacent soft tissues • Diaphragm The Diaphragm • Cupola – Cranioventral convex portion • Right and left crura – Attach to cranioventral border of L3 and body of L4 – May cause irregularity on these surfaces • Appearance depends on centering of X-ray beam The Diaphragm The End