Presentation
advertisement

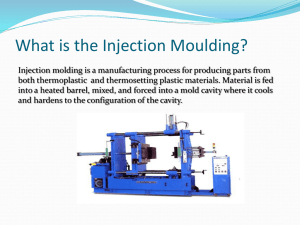
Kiddie-Caudals Caudal Epidural Analgesia in Everyday Pediatric Practice Sabine Kost-Byerly, MD, FAAP Associate Professor and Director, Pediatric Pain Management Department of Anesthesiology/Critical Care Medicine Johns Hopkins University, Baltimore, Maryland Objectives Upon completion of this lecture, the attendee will be able to: • Appreciate the technical aspects of caudal analgesia • Select appropriate local anesthetic solutions for caudal analgesia • Recognize and manage complications of caudal epidural analgesia Disclosures • I have no relevant financial relationships with manufacturers of any commercial products or providers of commercial services discussed in these slides. Caudal Epidural Analgesia thoracic Advantages: lumbar caudal Easy to perform High success rate Usually no hemodynamic changes Caudal Epidural - Indications • Surgeries: – Urologic – Orthopedic – general • Locations: – lower abdomen – lower extremities • Regional Alternatives to consider: – Peripheral nerve block – Truncal block – Extremity blocks Anesth Analg 2012;115:1353-64 Demographics for 13,725 patients in the Pediatric Regional Anesthesia Network (PRAN) database. Single Injection Caudal Placement by Age by age. Polaner D M et al. Anesth Analg 2012;115:1353-1364 Caudal Block in Children: Technique • Position: lateral decubitus, knees flexed • Landmarks: sacral cornuea at sacral hiatus • Needle position: 45°-60° angle to coronal plane • “pop” : piercing the sacro-coccygeal membrane • Reduce angle to 10°-20° and advance a few mm Kiddie- Caudal - Single Injection • Needle: – 22-g needle – 22 – g angiocath • (risk: epidermal-cell graft tumor – but: no reports) – 22-g short-beveled, styletted needle Caudal Block Identification of Landmarks Post sup iliac spines Sacral cornu Caudal Block Placement of Cannula Caudal Block in Children No Touch Technique Distance to Caudal Space Location, location…is your needle where it should be? Clinical Assessment Technical Aides • • Ultrasound The “pop” – the sacrococcygeal membrane – No visible/palpable subcutaneous – Experience, assistant injection • The whoosh (air) test – Risk: patchy block, venous air embolus • The swoosh (NS) test – Risk: dilution of LA Tiffterer l et al. Br JAnaesth 2012;108;670-4 Testdose – sometimes the caudal IV is the easiest… • Aspiration • Avoid patient simulation • Dose – Epinephrine 0.5 mcg/kg in 0.1 mL/kg of LA • Continuous ECG monitoring – T-wave changes >25% increase – HR increases – BP increases • Inject rest of LA dose slowly in increments Results: 742 pediatric epidural blocks 644 caudal 284 single caudal injections 42 (5.6%) Intravascular injection 3.8% with single caudal injections Detection: 6 immediate aspiration of blood 30 HR increases >10 bpm 25 T-wave amplitude increases 29 ECG changes in T-wave or rhythm Amide Local Anesthetics • Lidocaine • Sodium channel blockers • Protein binding – 65% (lido.) – 95% (bupiv., ropiv.) • Bupivacaine – Α1 acid glycoproteine (AAA), albumin • Neonate low AAA: ↑ free fraction of LA • Metabolism: – cytochrome P450 system • Ropivacaine • CYP3A4 for bupivacaine and lidocaine – Bupiv. at 1 mo 1/3 of adult, at 6 mo 2/3 • CYP1A2 for ropivacaine – Max for ropiv not reached till age 5 Choice of LA Bupivacaine: Ropivacaine: • Slower onset, longer duration • Cardiac toxicity>CNS toxicity • Duration similar • Less motor block at lower concentrations • Less toxicity • Single dose – 1 mL/kg of 0.25% bupivacaine – max <2.5 mg/kg • “Ideal”: concentration – 0.125 - 0.175% comparable duration of analgesia, less motor block • Single dose – 1 mL/kg 0.2% ropivacaine Choice of LA Lidocaine: Chloroprocaine: • Short onset, medium duration • CNS toxicity>cardiac toxicity • Short onset, short duration • Advantageous toxicity profile • Single dose • Single dose – up to 5-7 mg/kg – up to 14 mg/kg - or more Epidural Additives – improved and prolonged analgesia The Common The Rare Opioids • Continued concerns of safety • Inpatients only – Fentanyl 2 mc/kg – Morphine 12-50 mcg/kg • Pruritis, emesis, respiratory depression Clonidine for neuroaxial use: – preservative, ph, neurotoxicity • Ketamine 0.25 – 1 mg/kg • Neostigmine 2 mcg/kg – Emesis common • Alpha -2-agonist • Midazolam 50 mcg/kg • Single dose • Dexmedetomidine 1-2 mcg/kg – Risk: bradycardia, apnea in young infants – Increasing sedation with higher doses 2mcg/kg – Analgesia similar to clonidine • Tramadol 2 mg/kg 1- Caudal single Injection – Volume • Correlation between cranial level and volume • Exact prediction of level not possible • Volumes < 1 ml/kg not likely to reach higher than L2 • Speed of injection does not matter Brenner L et al. Br J Anaeth 2011; 107:229-35; Tiffterer l et al. Br JAnaesth 2012;108;670-4 Thomas L< et al. Paediatr Anaesth 2010;11:1017-21 • Volume for injection: – 0.5 ml/kg for perineal surgery – 1.0 ml/kg for lower abdominal surgery – 1.25 ml/kg for upper abdominal surgery Volume versus Concentration • RCT • Bupivacaine with epi O.8 mL/kg 0.25% B vs 1 ml/kg 0.2 % B • Lower GA requirement with higher volume • Maybe better postop analgesia with higher volume Vergehese ST et al. Anesth Analg 2002;95:1219-23 Complications Common: Rare, but serious • Pruritis • Systemic toxicity • Nausea & emesis • Sedation • Urinary retention – Inadvertent IV injection • Overdose – Inadvertent IT injection • Infection/Hematoma/Neuro pathy Risk of Systemic LA Toxicity Pediatric Anesthesia 2010;20:1061-1069 • 10,098 epidurals – 8493 caudals – 7 with transient ECG changes – no treatment ASRA Recommendations – Prevention of LAST Neal JM et al. Reg Anesth Pain Med 2010;35:152-61 • Lowest effective dose of local anesthetic • Incremental injection of local anesthetics • Aspirate the needle or catheter before each injection • Use of an intravascular marker (epinephrine) is recommended. • Ultrasound guidance may reduce frequency of intravascular injection – Effectiveness remains to be determined ASRA - recommended LAST -Management Neal JM et al. Reg Anesth Pain Med 2010;35: 152-61 • ABC’s • Seizures: • – Benzodiazepines, small dose propofol – avoid large dose propofol for risk of CV compromise – Succhinylcholine or other NDMB , small doses to minimize acidosis and hypoxemia Cardiac arrest Lipid emulsion therapy – ACLS , but Consider administering at the first signs of LAST, after airway management • epinephrine - small initial doses (10mcg to 100 mcg boluses in the adult) preferred • Vasopressin not recommended 1.5• mL/kg 20% lipid emulsion bolus Calcium channel blockers and A-adrenergic receptor blockers – avoid 0.25 per minutearrhythmias, of infusion, continued for at(lidocaine least or 10procainamide) mins after • mL/kg Amiodorone for ventricular treatment with local anesthetics not recommended circulatory stability is attained – Lipid emulsion therapy -Consider administering at the first signs of LAST, after airway management • 1.5 mL/kg 20% lipid emulsion bolus Consider rebolus if circulatory stability is not attained and increase infusion to 0.25 mL/kg perminute minute of infusion, continued for at least 10 mins after circulatory stability30 is attained 0.5• mL/kg per (up to 10 mL/kg lipid emulsion within mins) • Consider rebolus if circulatory stability is not attained and increase infusion to 0.5 mL/kg per minute (up to 10 mL/kg lipid emulsion within 30 mins) Propofol is not a substitute for lipid emulsion – – Propofol is not a substitute for lipid emulsion Cardiopulmonary bypass • failure to respond to lipid emulsion and vasopressor therapy • notify the closest facility capable of providing it when CV compromise is first identified during an episode of LAST. Intralipid for LA-induced Cardiotoxicity in infants • 2-day-old 3.2 kg term infant – Caudal, 1 mL/kg 0.25% bupivacaine, with US guidance and confirmation – VT, cardiovascular collapse – 20% Intralipid 1 ml/kg – recovery Lin EP et al. Pediatric Anesthesia 2010; 20:955-7 • 40-day-old, 4.96 kg infant – Caudal, 0.9 mL/kg 0.25% bupivacaine – Tachycardia, T-wave inversion hypotension – Epinephrine 2 mcg/kg x2, 20mL 55 albumin – no change – 20% Intralipid 2 ml/kg – recovery Shah S et al. J Anesth 2009; 23:430-41 Adverse Events and Complications TD DP VP AB FB C R N Other Total Events Total Procedures % Caudal 18 5 38 71 26 1 0 0 13 172 6011 (97%) 2.9 Lumbar 0 2 0 2 0 0 0 0 1 5 103 4.9 Thoracic 0 1 0 1 0 0 0 0 0 2 13 15.4 Subarachnoid / / 0 2 2 1 0 0 1 6 83 7.2 Total 18 7 38 76 28 2 0 0 15 184 6210 3.0 TD: DP: VP: AB: FB: C: R: N: positive test dose dural puncture vascular puncture abandoned block failed block cardiovascular respiratory neurological NO significant complications in caudal group! 93% of caudal blocks placed without technical aids or imaging 3% with ultrasound guidance Summary Caudal anesthesia and analgesia is: • An easy technique to supplement general anesthesia • Requires few resources • Easy to learn • Provides several hours of postoperative analgesia • Is overall a very safe analgesic technique Thank You Questions?