Assessing cost-effectiveness
– what is an ICER?Incremental analysis
Usa Chaikledkaew, Ph.D.
Outline
How to conduct health economic
evaluation results?
What is an Incremental costeffectiveness ratio (ICER)?
2
What is health economic evaluation?
Refers to a study that
considers both the
comparative costs
associated with two or
more health care
interventions, and the
comparative clinical
effects, measured either
in clinical units, health
preferences, or monetary
benefit
Costs
$
Outcomes
LYGs
QALYs
$
Source: Drummond et al, 2005
3
What Counts As An Economic
Evaluation?
COMPARISON
OF TWO OR
MORE
ALTERNATIVES?
COSTS (INPUTS) AND CONSEQUENCES
(OUTPUTS) EXAMINED?
No
Yes
No
Outcome
Cost
Cost-outcome
description
description
description
Yes Outcome
analysis
Source: Drummond et al, 2005
Cost analysis Full economic
evaluation
4
Economic Evaluation Methods
Methods
Cost
Cost-Minimization
Analysis (CMA)
฿
Cost-Benefit
Analysis (CBA)
฿
Outcome
Usually clinical values
(Assume to be
equivalent in
comparable groups)
฿
Results
Cost per case
Net benefit
Benefit-to-cost ratio
Return on investment
(ROI)
Cost-Effectiveness
Analysis (CEA)
฿
Clinical values
Life year gained (LYG)
ICER (cost per LYG)
Cost-Utility
Analysis (CUA)
฿
Quality-adjusted life
years (QALYs)
ICER (cost per QALY)
5
Incremental cost-effectiveness ratio (ICER)
(cost of treatment A) – (cost of treatment B)
(clinical success treatment A) – (clinical success treatment B)
Or
(cost of treatment A) – (cost of treatment B)
(LYG A – LYG B)
Or (cost of treatment A) – (cost of treatment B)
(QALY A – QALY B)
The cost that on average needs to be sustained to
obtain “an additional success”
6
Cost-effectiveness threshold or WTP
UK: < £30,000 per QALY gained
USA: < $50,000 per QALY gained
Countries in the World: < 3 x GDP per DALY
averted
Thailand: < 1.2 GNI per capita per QALY
gained (160,000 THB)
Source: (1) Devlin, N. and Parkin, D. Health Economics, 2004; 13: 437-452.
(2) Towse, A., Devlin, N., Pritchard, C (eds) (2002) Cost effectiveness thresholds: economic and ethical
issues. London: Office for Health Economics/King's Fund.
(3) Thavorncharoensap et al. Assessing a societal value for a ceiling threshold in Thailand. 2013.
Health Intervention and Technology Assessment Program (HITAP), Ministry of Public health, Nonthaburi,
Thailand.
7
How to conduct health
economic evaluation
results?
8
PE/HEE Study Designs
9
1. Prospective: alongside clinical trial
2. Model based
Combining different sources e.g. a model, based
on input from clinical trials, retrospective data,
expert opinion.
1.1 Decision trees
1.2 Markov models
9
How to conduct HEE results?
Define the problem
Identify the alternative interventions
Identify and measure cost and outcomes
Value costs and effectiveness
Interpret and present results
10
Example
Source: Thavorn et al. Tobacco Control 2008;17:177–182. doi:10.1136/tc.2007.022368
11
Define the problem
Perception of the
problem
•
•
•
•
Specific intervention
Specific strategy
Specific drug
Specific surgical
procedure
12
Define the problem
Selection of objectives
• A decision must be
made about how costeffectiveness will be
evaluated.
13
Define the problem
Perspective
•
•
•
•
•
•
Patient
Provider
Third Party Payer
Healthy System
Public/Government
Societal
14
Cost
Category Subcategory
Direct
medical
Direct
non
medical
Indirect
Other
sectors
P.15
Patient
Treatment/
health care:
Study setting
Other health
facilities
Personal
facilities
charge
Travel
Food
House
Time loss
Informal care
Personal care
Morbidity cost
Mortality cost
Welfare
charge
charge
charge
income loss
income loss
charge
income loss
income loss
travel/food/
fee/material
travel/food/
fee/material
Education
charge
charge
Valuation by perspective
Provider 3rd -party Health
Public/
Societal
payer
system government
cost
Reimburse
cost
cost
Copay
premium
-/+
charge
charge
charge
reimburse
charge
-
-/+
reimburse
-/+
reimburse
-
cost
charge
charge
charge
Productivity cost
Productivity cost
charge
Productivity cost
Productivity cost
cost
-
cost
cost
Identify the alternative interventions
16
Choice of comparator(s)
•An intervention should be compared to the comparator (s) which is
most likely to be replaced by the intervention in real practice
•Current practice may be :
•The most effective clinical practice
•The most used practice
•May not always reflect the appropriate care that is
recommended according to evidence-based medicine
•Minimum clinical practice
•A practice which has the lowest cost and is more effective
than a placebo.
•“doing nothing” or no treatment
17
Identify the costs
Sources of cost data
• Hospital (charges, unit
cost)
• Ministry of Public
Health website
• DRG
• Reimbursement list
• Standard costing menu
18
Example of cost estimates
19
Identify the outcomes
20
Quality Adjusted Life Years (QALYs)
Integrate mortality, morbidity, and
preferences into a comprehensive index
number
Related to outcomes
• Life duration
• Quality of life
Allows comparisons of the cost-effectiveness
results with other medical interventions
21
Quality-Adjusted Life Years (QALYs)
QALYs = number of years lived x utility*
Patient 1:
• Utility = 0.9
• Number of years = 10
• QALYs = 0.9 x 10 = 9 QALY
Patient 2:
• Utility = 0.5
• Number of years = 10
• QALYs = 0.5 x 10 = 5 QALYs
Quantity or life
Quality weight
that represents
HRQOL
* Utility can be ranged from 0 (worst health state) to 1
(best health state/healthy)
22
Valuing costs and outcomes
Model based
• Decision tree model
• Markov model
Discounting to
present value if its
been more than one
year
Uncertainty analysis
23
What is an Incremental
cost-effectiveness ratio
(ICER)?
24
25
Interpretation and presentation of
results
Incremental cost-effectiveness ratio (ICER)
(cost of treatment A) – (cost of treatment B)
(clinical success treatment A) – (clinical success treatment B)
Or
(cost of treatment A) – (cost of treatment B)
(LYG A – LYG B)
Or (cost of treatment A) – (cost of treatment B)
(QALY A – QALY B)
The cost that on average needs to be sustained to
obtain “an additional success”
25
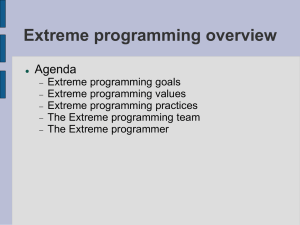
The need for incremental thinking
Marginal analysis: requires
assessment of relative costs and
benefits of each marginal addition
or reduction in production or
consumption
26
Number
Numberofoftest
test
1
2
3
4
5
6
1
2
3
4
5
6
Number
Numberofoftest
test
1
2
3
4
5
6
1
2
3
4
5
6
Total
casescases
Total
detected
detected
65.9469 65.9469
71.4424 71.4424
71.9003 71.9003
71.9385 71.9385
71.9417 71.9417
71.9420
71.9420
Total
costs
($) ($)
Total
costs
Incremental
cases
Incremental
detected
cases detected
65.9469 65.9469
5.4956
5.4956
0.4580
0.4580
0.0382
0.0382
0.0032
0.0032
0.0003
Incremental
costs
costscosts
/
Incremental
costs Incremental
Incremental
($)
case ($)/ case ($)
($)
77.511
77.511 1,175
1,175
30.179
30.179 5.492
5,492
22.509
49.150
22.509
49,150
17.917
469.534
17.917
469,534
15.024
4.724.695
15.024
4,724,695
13.190
47.107.214
0.0003
77,511
107,690
130,199
148,116
163,141
176,331
Average
costs
($) ($)
Average
costs
77,511 1,175
107,690 1,507
130,199 1,811
148,116 2,059
163,141 2,268
176,331 2,451
13.190
1,175
1,507
1,811
2,059
2,268
2,451
47,107,214
Source: 1975 article from Neuhauser and Levicky: “what do we gain from
the sixth stool-guaic” (N Engl J Med) on stool tests do detect colonic 27
27
cancer
28
Interpretation and presentation of
results
Incremental cost-effectiveness ratio (ICER)
(cost of CPSC) – (cost of treatment of Usual Care)
(Life Years of CPSC) – (Life Years of Usual Care)
The cost that on average needs to be sustained to
obtain “one Life Year gained”
28
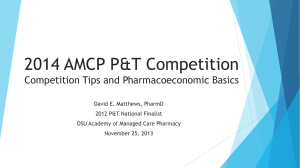
ICER of CPSC compared to Usual Care by Age and Sex
Gender/Age
Incremental
cost
Life years
gained
(year)
(THB)
(Years)
ICERs of CPSC
compared to Usual
Care
(THB per LY gained†)
-17,504
-16,356
-12,387
-21,500
-20,074
-14,889
0.181
0.152
0.121
0.244
0.205
0.161
-96,705 (Dominant)
-107,603 (Dominant)
-102,373 (Dominant)
-88,114 (Dominant)
-97,922 (Dominant)
-92,479 (Dominant)
Male, 40
Male, 50
Male, 60
Female, 40
Female, 50
Female, 60
*Negative ICER due to higher effectiveness and lower costs of CPSC
compared with Usual Care
29
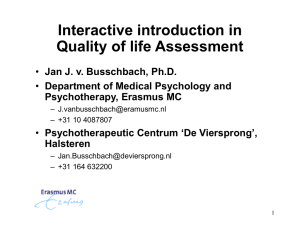
Cost-effectiveness plane
more costly
B
D
Intervention is more
effective and more costly
Intervention is less
effective and more costly
decrease in health effects
increase in health effects
C
A
Intervention is less
effective and less costly
Intervention is more
effective and less costly
30
less costly
Conclusions
31
Cost-effectiveness league table of selected interventions in Thailand
Health Interventions
Baht/QALY
(2008)
Coverage
Antiretroviral treatment vs. palliative care
26,000
Yes
Prevention of vertical HIV transmission (AZT + NVP) vs. null
25,000
Yes
Statin (generic) in men >30% CVD risk vs. null
82,000
Yes
Cytomegalovirus retinitis: Gancyclovir vs. palliative
185,000
Yes
Antidiabetic: Pioglitazone vs. Rosiglitazone
211,000
No
HPV vaccine at age 15 vs. Pap smear, 35-60 years old, q 5
years
247,000
No
Osteoporosis: Alendronate vs. calcium + vitamin D
296,000
No
Osteoporosis: Residronate vs. calcium + vitamin D
328,000
No
Peritoneal dialysis vs. palliative care included anyway cs ethic
issues/ surviability
435,000
Yes
Hemodialysis vs. palliative care included anyway cs ethic
issues/ surviability
449,000
Yes
Osteoporosis: Raloxifene vs. calcium + vitamin D
634,000
No
Osteoporosis: Calcitonin vs. calcium + vitamin D
1,024,000
No
HPV vaccine at age > 25 vs. Pap smear, 35-60 years old, q 5
years
2,500,000
No
Anemia in cancer patients: Erythropoitin vs. blood transfusion
2,700,000
No
Thank you, Any question?
33
usa.c@hitap.net