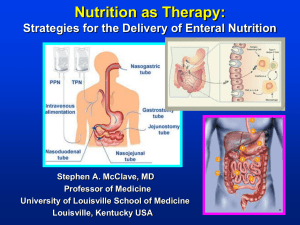
for the critically ill patient who requires nutrition support therapy.
advertisement

Objectives • Understand at least 3 steps to consider when implementing a change to dietitian’s practices in the hospital setting. 1 ASPEN/SCCM Guidelines A2. Nutrition support therapy in the form of enteral nutrition (EN) should be initiated in the critically ill patient who is unable to maintain volitional intake. (Grade: C) 2 JPEN 2009; 33:277-316 ASPEN/SCCM Guidelines A3. EN is the preferred route of feeding over parenteral nutrition (PN) for the critically ill patient who requires nutrition support therapy. (Grade: B) JPEN 2009; 33:277-316 3 ASPEN/SCCM Guidelines A4. Enteral feeding should be started early within the first 24-48 hours following admission. (Grade: C) The feedings should be advanced toward goal over the next 48-72 hours. (Grade: E) JPEN 2009; 33:277-316 4 Timing: Window of Opportunity • Early feeding in critically ill patients • Early defined as <36 hours from admission to ICU or post-op • Early EN group outcomes: Lower incidence of infection (p=0.0006) Reduced LOS by 2.2 days (p=0.004) Decreased mortality (not significant) 5 Marik P et al. CCM 2001; 29: 2264 Timing: Window of Opportunity • Compared early EN vs NPO in GI surgery pts • Early defined as <24 hours post-op GI surgery • Early fed (EN or PO) group outcomes: Reduced risk of anastomotic dehiscence (p=0.08) Reduced infections (p=0.036) Reduced LOS by 0.8 days (p=0.001) Reduced mortality (p=0.15) 6 Lewis SJ et al. BJM 2001; 323:1-5 ASPEN/SCCM Guidelines A7. Either gastric or small bowel feeding is acceptable in the ICU setting. Critically ill patients should be fed via an enteral access tube placed in the small bowel if at high risk for aspiration or after showing intolerance to gastric feeding. (Grade: C) Withholding of enteral feeding for repeated high gastric residual volumes alone may be sufficient reason to switch to small bowel feeding (the definition for high gastric residual volume is likely to vary from one hospital to the next, as determined by individual institutional protocol). (Grade: E) JPEN 2009; 33:277-316 7 Process Before Using Electromagnetic Technology 8 Time Delays with C-arm Placement • 5 month data collection of feeding tube placements in the ICU showed 13.4% (n=29) placement delays • Reasons for delays included: 6.9% other procedures on pt caused FT to be postponed 34.5% order entered incorrectly in EHR 58.6% scheduling issues/prioritizes within radiology 9 Radiation Exposure • 2010 FDA Press Release “The U.S. Food and Drug Administration have announced an initiative to reduce unnecessary radiation exposure from three types of medical procedures: computed tomography (CT), nuclear medicine studies, and fluoroscopy.” • FDA working with CMS to incorporate the initiative into regulations and guidelines 10 http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm200085.htm Radiation Exposure • Average placement time with fluoro is 3.7 minutes • Random sample of 1 month showed 20% exceeded 5 minutes • Average dose is120 mrem • 300 mrem is the average annual dose in Minnesota • A chest film is 2 mrem • Rooms in ICU are not leaded, scatter field near patient is 4.5 mrem/min 11 Process of Implementation • Gather data Time delays Radiation exposure Patient Safety/Transport Staffing time/costs Scope of practice considerations 12 Dietitian Standards of Practice • Academy Standard 3: Nutrition Intervention RDs identify and implement appropriate, purposefully planned actions designed with the intent of changing a nutrition-related behavior, risk factor, environmental condition, or aspect of health status for an individual, target group or the community at large. • Dietitians in Nutrition Support 3.10 Carries out the plan for nutrition support therapy 3.10D With specialized training, demonstrated competency, and delineated clinical privileges may place nasoenteric access devices JADA 2008:108 (10);1538-1542 13 NCP 2007:22;558-586 Dietitian Scope of Practice • State Board Subd. 10. Nutrition care services. "Nutrition care services" means: (1) assessment of the nutritional needs of individuals or groups; (2) establishment of priorities, goals, and objectives to meet nutritional needs; (3) provision of nutrition counseling for both normal and therapeutic needs; (4) development, implementation, and management of nutrition care services; or (5) evaluation, adjustment, and maintenance of appropriate standards of quality in nutrition care. 14 www.dieteticsnutritionboard.state.mn.us/ Academy Decision Analysis Tool • Part A: General Review Describe the activity or service to be performed Review the practice expectations (job description, policies and procedures) and core competencies for your level (DTR, RD, or RD Specialty/Advanced Practice) to determine whether the service or act is permitted. Review the Code of Ethics, Standards of Practice in Nutrition Care, and Standards of Professional Performance for your practice level to determine whether the service or act is permitted. Review any licensure laws to determine whether the activity is allowed or not explicitly restricted. 15 Academy Decision Analysis Tool • Part B: Education, Credentialing, Privileging • Part C: Existing Documentation • Part D: Advisory Opinions • Part E: Obtaining an Advisory Opinion • Part F: Performing the Service or Activity 16 Process of Implementation • PEC • TAC • Med Exec • Critical Care • Nursing Leaders • Risk • HR 17 Training • Policies – Feeding Tube Placement, Bridle • Observe 3 FT placements with fluoro • Review training video • 10 successful placements with a radiologist • Annual competency 18 Learnings and Re-implementation • Communication TEAM STEPPS • Order set for providers to ensure correct equipment used • Indications for when to stop 19 Historical Data • 2008 – 579 placed via fluoro (324 bedside or SPR) • 2009 – 656 placed via fluoro (401 bedside or SPR) • 2010 – ~680 placed via fluoro (~416 bedside or SPR) • 2011 – ~688 placed via fluoro ( ~330 bedside or SPR), 91 placed by dietitians Jan - March • 2012 – 454 placed via fluoro, 414 placed by dietitians 20 Current Process with Cortrak • Feeding Tube Team consists of 3 dietitians • Additional 4 dietitians in process of training • Schedule of 1 week coverage rotation (FT, Obs, Relief) • Scrubs worn during FT coverage • No RNs placing tubes at this time • No standardized weekend coverage with Cortrak 21 2012 Feeding Tube Placement Data 100 90 80 70 60 # tubes placed with fluoro all units 50 # tubes placed by dietitians ICU only 40 30 20 10 0 Jan 22 Feb March April May June July August Sept Oct Nov Dec 2012 Feeding Tube Placement Data 18 16 14 12 10 8 6 4 2 0 Bridles June 23 July August Sept Oct Nov Dec 2012 Feeding Tube Placement Data 50 45 40 35 30 # tubes placed with fluoro in ICU 25 # tubes placed by dietitians in ICU 20 15 10 5 0 Oct 24 Nov Dec 2012 Feeding Tube Placement Data Tubes Placed per Unit in 2012 180 160 140 120 100 80 60 40 20 0 MICU 25 SICU CVICU 2012 Feeding Tube Placement Data 100% 80% % successful post pyloric radiology 60% % successful post pyloric dietitians 40% % successful total RD placements(including gastric) 20% 0% Jan 26 Feb March April May June July August Sept Oct Nov Dec 2012 Feeding Tube Placement Data 7 6 5 4 3 2 1 0 27 Time from CPOE to FT Placement 2012 Feeding Tube Placement Data 60% 50% 40% 30% Length of Time to Place Tube 20% 10% 0% 15 min 28 30 min 45 min 60 min 29 30 31 Benefits At Fairview Using Electromagnetic Technology • Reduced radiation exposure • Improved time to placement • Reduced need for replacements due to “kinks” 32