“Growing Pains”
Injury and Skeletal Immaturity
Ken Knecht, PT, MS, SCS, CSCS
Understanding the Population
Children are not
“Little Adults”
Understanding the Population
“What’s the Difference?”
Skeletal Maturity
Physiology
Strength (and the Ability to Develop It)
Psychological Maturity
Understanding the Population
“What’s the Difference?”
Skeletal Maturity
Physiology
Strength (and the Ability to Develop It)
Psychological Maturity
Growth & Development of the
Young Athlete
Middle Childhood (6-9 yrs)
Maturation of Throwing and Kicking Patterns
Entry Level Sports (soccer, baseball/softball)
Males and females can still compete with parity
Males slightly Stronger; Girls better Balance
Running gait and speed are fairly equal
Late Childhood to Early Adolescence (10-15 yrs)
Onset of Puberty
“Growth Spurt” – Tanner Stage 3
Differences emerge between sexes
Skill Acquisition and Development Easiest
Growth and Development of the
Young Athlete
Late Adolescence/Adulthood (16-20 yrs)
Increases in Strength & Size become more gradual
“Late Bloomers” may continue to lag behind
Skeletal maturity
Growth and Development
Anatomic Changes Associated with Puberty
Boys
Girls
(Mean Age)
Peak Height Velocity (14 yrs)
Peak Height Velocity (12 yrs)
Skeletal Maturity (16 yrs)
Skeletal Maturity (14 yrs)
**Introduction of Sex hormones
(Athl Ther Today 2002)
Growth and Development
Significance of Peak Height Velocity
The “Growth Spurt”
~ Tanner Stage 3
Bone growth rate can exceed soft tissue
accommodation
Hamstrings, Hip flexors, Quadriceps, and Plantarflexors
Decreased Coordination
Tightness can affect growth centers
Growth and Development
Significance of Tanner Staging
5 stages of Physical development
Stage 1 = Early Development
Stage 5 = Full Maturity
Correlation between Tanner stage and
physeal closure.
Same Chronologic age ≠ Bone Age
Assists with the differential diagnoses
Growth and Development
Tanner Stage 5
Signals end of growth
Marked by full development of secondary
sexual characteristics
Males will have full facial hair
Females will have final breast development
Skeletally Immature Distinctions
Growth “Tissues”
Physis
Apophysis
Articular Cartilage
Issues:
Susceptibility to injury
Bone weakest link
Surgical Challenges
“Growth Tissue”
Physis
(Growth Plate)
Responsible for longitudinal growth of bone
Growth centers close distal to proximal
Growth centers begin to close in females
approximately 18 – 24 months following
menarche
Skeletal Maturity Completed
~18 yrs females;
~21 yrs males
Injury to Physis could create growth
disturbance (early closure or bony bridging)
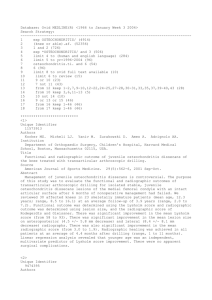
Anatomical Review
http://www.davidlnelson.md/images/Physis_normal_annotated4.jpg
Salter-Harris Fractures
Type I:
Fracture line extends across the physeal plate.
Often undetected on X-ray
Type II:
Fracture line extends through the physeal plate and
metaphysis
Type III:
Fracture line extends from the joint surface through
the epiphysis and across the physis causing a portion
of the epiphysis to become displaced
Type IV:
Fracture line extends from joint surface through the
epiphysis, physeal plate and metaphysis causing a
fracture fragment
Type V:
Crush injury to the growth plate
Salter Harris Fractures
Separated
Above
Lower
Through
E Rammed
Salter Harris Fracture
Distal Fibula
Usually an inversion/supination injury
Type I-II are the most common
Type I often misdiagnosed as ankle sprain
Salter Harris Fracture
Key Finding on Physical Exam:
Point of Maximal Tenderness
Usually PTP at ATFL also
Salter Harris Fracture
Boot immobilization (casting)
Depending on Type; 2-3 weeks +
Types III & IV require surgery
Pain free weight bearing status
Rehabilitation for post immobilization
ROM, strength, balance & proprioception
Sport specific training
Little League Shoulder
Epiphysiolysis of proximal
humerus
Rotational forces
Distractional forces
Overuse injury associated
with pitching
Quantity
Intensity
Age
Phases of Throwing
www.hughston.com/hha/b_16_1_1a.jpg
Little League Shoulder
Clinical Findings
Lateral, proximal shoulder pain
Weak & painful EROT and Abd
Palpable tenderness over physis
Radiographic widening of physis?
Little League Shoulder
Treatment
Aggressive rest to allow physeal healing
Address any ROM imbalances & Scapular dysfunction
Rotator cuff strengthening
Review of throwing mechanics
GIRD, posterior capsule
Sick Scapula
Scapular stabilization & strengthening
Return to throwing progression
Modification of throwing volume (pitch counts)
May need to alter position
Address entire kinetic chain
Core strengthening
Lower extremity strength/flexibility and proprioception
“Growth Tissue”
Apophysis
Cartilaginous structure usually located at the
end of long bones
Attachment site for musculotendinous unit
Tensile forces can create inflammation =
Apophysitis
Susceptible to Avulsion Fracture
Apophysitis
Overuse injury
Often during periods of rapid growth
May remain symptomatic until closure of
apophysis
Possible to result in an avulsion fracture
Sever’s Disease
aka: Calcaneal Apophysitis
Common During Growth
Spurt
Heel pain
Tight gastroc/soleus
Foot pronation
Running/jumping athletes
+ Squeeze Test
Sever’s Disease Treatment
Activity modification
Aggressive rest
Stretching!!!
Immobilization may be necessary
Can continue to play if pain is mild (no limp)
Typically resolves in several weeks (months?)
Footwear or insert
Osgood-Schlatter’s Disease (OSD)
Apophysitis of the
Tibial Tubercle
Traction Injury
Commonly seen
Boys aged 10 –15
Girls aged 8 –13
Osgood-Schlatter’s Disease (OSD)
Palpable tenderness
X-rays may be positive
for displacement
In severe cases tubercle
can avulse
Osgood-Schlatter’s Disease (OSD)
Sinding-Larsen-Johansson (SLJ)
Apophysitis of the inferior
patellar pole
Anterior knee pain with
impact activities
Commonly seen
Boys aged 10 –15
Girls aged 8 –13
Sinding-Larsen-Johansson (SLJ)
Palpable tenderness
Inferior pole sometimes
patellar tendon
May have quadriceps lag
X-rays may be positive
for displacement
Differential diagnosis
Patellar sleeve fracture
Treatment for OSD and SLJ
Activity modification
Stretching quads and hams
Strengthening progression
Plyometric training to work on soft landings
May not have complete resolution of symptoms
In OSD permanent bump is likely
Apophysitis of Hip/Pelvis
7 sites at the femur and pelvis
During phase of rapid growth
Pain and inflammation at
ossification centers
Iliac crest (common)
Pain with resisted trunk rotation/side
bend and/or hip abduction
Seen in Runners, Football, and
occasionally Baseball pitchers
Apophysitis of Hip/Pelvis
Treatment
Rest
Activity modification
Trunk and pelvis flexibility
Core and hip strengthening
Treat the entire kinetic chain
Technique adjustment
Running gait
Avulsion Fractures
Same areas affected as apophysitis
Occur with sudden, forceful contraction or stretching
Bone is the weakest link
Common sites include ASIS and Ischial tuberosity.
Often misdiagnosed as pulled muscle
Radiographic evaluation necessary for accurate diagnosis
Surgery if displacement is greater than 2-3cm (???)
Avulsion Fractures
AIIS avulsion fracture in a 14 yr old soccer player
Little League Elbow
Traction apophysitis of Medial epicondyle of Humerus
Overuse injury
Valgus stress during late
cocking/acceleration
Flexor pronator muscle group
Volume
Velocity
Increased mound to plate distance
Breaking Pitches?
UCL?
Clinical presentation
Medial elbow pain
Diminished throwing speed and accuracy
Poor or altered throwing mechanics
Little League Elbow
Treatment
RICE: Make rest your friend
Activity modification 6-12 weeks
Stretching
GIRD is Probable; Assess and address!!!
Strengthening
No pitching or overhand throwing
Forearm, posterior cuff, core, contralateral leg
Assess throwing mechanics
Functional progression to throwing program
Identify and correct training errors
“Growth Tissue”
Articular Cartilage
Infrastructure similar to Physis
Increased Cellular activity
Not yet “Adult” solidity
Repetitive Injury or Excessive shearing forces
may result in Osteochondritis Dissecans
(OCD)
Osteochondritis Dissecans (OCD)
Impact and shear forces cause bone bruising
Cause is usually repetitive trauma
Genetic predisposition?
Subchondral bone death
Secondary damage to overlying cartilage
“Lesion of dissection” vs dessication
May affect any joint
Most frequently seen at knee, elbow, ankle
Osteochondritis Dissecans (OCD)
Risk Factors
Age: Occurs most often in people between the ages
of 9 and 18
Sex: Males are 2-3X more likely than females.
Sports participation: Sports that involve rapid
changes in direction, jumping or repeated throwing
may increase your risk
Osteochondritis Dissecans (OCD)
ICRS Classification of OCD
Grade I – Stable with continuous but
softened area with intact cartilage
Grade II – Stable with partial
discontinuity
Grade III – In situ lesions with
complete discontinuity
Grade IV – Empty defects with
dislocated or loose fragments
Osteochondritis Dissecans (OCD)
Epiphyseal microtrauma with
osteochondral separation
Commonly Lateral aspect of Medial
femoral condyle
Etiology is multifactorial
Trauma, ischemia, hereditary,
idiopathic (?)
Under debate
Osteochondritis Dissecans (OCD)
OCD of Femoral Condyle
Clinical presentation
Insidious onset of pain aggravated by
activity
Intermittent joint effusion
Giving way, catching, or locking
Symptoms suggestive of PFPS
Confirmed with diagnostic imaging
OCD of Femoral Condyle
Conservative Management
Immobilization
Weight bearing restriction
Activity restriction
Surgical intervention
Extent depends on Grade
Debridement /drilling
Refixation
Loose body removal
Operative resurfacing
ACI
Clinical Summary
Bone weakest link in pre pubescent
Same Chronological age ≠ Bone Age
Tanner staging helps differential
Protect Growth centers
THANK YOU!!!
Ken Knecht PT, MS, SCS, CSCS
Board Certified Sports Clinical Specialist
The Sports Medicine & Performance Center at
CHOP Specialty Care Center at
Virtua Health and Wellness Center, 2nd Floor
200 Bowman Drive, Suite D260
Voorhees, NJ 08043
856-719-9932; Fax: 267-425-5416
knecht@email.chop.edu