Ertapenem for the Treatment of Osteomyelitis: A Retrospective Analysis
of the Bone And Joint Infection Organization (BAJIO) Database.
Medina Stella MD¹, Gnoni Martin MD¹, Mariko Cheick CRC¹, Harting Julie PharmD¹,³, Newman David PharmD², Kelley Robert PhD¹,Christensen Diana MD¹,², and Julio Ramirez MD¹².
¹Division of Infectious Diseases, University of Louisville, ²Robley Rex Veterans Affairs Medical Center, ³Sullivan College of Pharmacy all in Louisville, Kentucky. Bone And Joint Infection
Organization (BAJIO) Group.
ABSTRACT
Background: There is limited data regarding ertapenem in the treatment
of osteomyelitis. The objective of this study was to analyze data from
patients receiving ertapenem for the treatment of osteomyelitis to further
characterize clinical outcomes and adverse effects associated with
ertapenem-prolonged therapy.
Methods: This was a retrospective study of adult patients with diagnosis
of osteomyelitis treated with ertapenem at the UofL Hospital and the VA
Hospital in Louisville, KY. All patients from December 2010 to February
2013 with diagnosis of osteomyelitis treated with ertapenem for ≥ 2 weeks
were reviewed. The diagnosis of osteomyelitis was confirmed using
radiographic or histopathologic criteria, or positive bone culture. The
microbiological diagnosis was confirmed with positive bone culture, deep
tissue culture, or blood culture. A patient was a candidate for ertapenem if
the osteomyelitis was polymicrobial.
Results: A total of 33 patients were reviewed (79% males). Nine diabetic
foot infections, 19 other locations, 3 PJI and 2 Septic arthritis. Median
ertapenem days were 40 (18-76). Median follow up was 114 days (20547). Seventeen and 16 patients received 2 grams Q24 and 1 gram Q24
respectively. The success rate was 85%. Minor adverse effects were seen
in 33% and were not related with the dose.
Conclusion: ertapenem appears to be effective in the treatment of
osteomyelitis. It possesses a favorable safety profile even with high doses.
These findings warrant further research describing ertapenem use in bone
infections.
INTRODUCTION
• Ertapenem is FDA approved for the treatment of complicated intraabdominal infections, complicated skin/skin structure infections,
including diabetic foot infections without osteomyelitis, communityacquired pneumonia, complicated urinary tract infections (including
pyelonephritis), acute pelvic infections (including postpartum
endomyometritis), septic abortion, and postsurgical gynecologic
infections and prophylaxis of surgical site infection following elective
colorectal surgery. [1]
• Ertapenem is a broad-spectrum carbapenem with a long
half-life permitting once-daily dosing.
• Ertapenem has activity against the most invasive bacterial pathogens
except for methicillin-resistant Staphylococcus aureus (MRSA),
Enterococci, Pseudomonas aeruginosa, and Acinetobacter baumannii.
[2]
• A prior study has shown 12 cases of osteomyelitis treated with
ertapenem as the primary antimicrobial with a success rate of 50%
among patients who received an average of six weeks of ertapenem.[2]
• There are few case reports with ertapenem for the treatment of
osteomyelitis.[3,4]
• A study of obese patients with vertebral osteomyelitis suggests that 1gr
q 24 hs is suboptimal/sub therapeutic.[5]
• There are limited data regarding ertapenem in the treatment of
osteomyelitis.
• The objective of this study was to analyze data from patients receiving
ertapenem for osteomyelitis to further characterize clinical outcomes
and adverse effects associated with ertapenem-prolonged therapy.
MATERIALS AND METHODS
Study Design:
• This was a secondary analysis of the BAJIO database examining
osteomyelitis cases treated with ertapenem.
• The database included patients from the University of Louisville
Hospital and the Robley Rex Veterans Affairs Medical Center
both in Louisville, Kentucky.
Inclusion Criteria:
• ≥18 years of age
• Confirmed osteomyelitis:
1. Osteomyelitis confirmed by x-rays, computed tomography,
magnetic resonance imaging, and/or nuclear medicine studies.
1. Suggestive radiologic indices augmented by histologic evaluation
of bone and/or positive cultures for bacteria in bone biopsy
specimens.
• A patient was a candidate for ertapenem if the osteomyelitis was
polymicrobial either by culture or clinical suspicion.
RESULTS (Cont’d)
RESULTS
• For the primary endpoint of clinical success, 27/30 evaluable patients
(90%) achieved success, 3 patients were lost to follow-up.
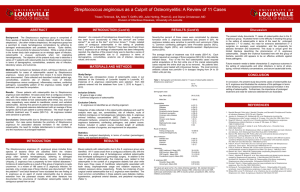
Table 2: Pathogenic isolates from clinically evaluable patients with
osteomyelitis.
___________________________________________________________________________________________________________________________
• A total of 33 patients were evaluated for adverse events and
discontinuations of ertapenem
Organism (s)
No. (%)
(n = 36)
___________________________________________________________________________________________________________________________
Enterobacteriaceae
Enterobacter cloacae
Escherichia coli
Klebsiella
Serratia marcescens
Citrobacter
Proteus mirabilis
13/36 (36%)
5
3
2
1
1
1
• The incidence of adverse events between the 1g and 2g dosing strategies
did not differ statistically.
Staphylococcus aureus
Methicillin-resistant
Methicillin-susceptible
4/36 (11%)
3
1
• Ertapenem was discontinued in 5 patients due to an adverse event.
Discontinuations between the 1g and 2g groups did not differ statistically.
Staphylococcus coagulase negative
5/36 (14%)
Streptococcus species
Streptococcus viridans
Streptococcus anginosus group
Other streptococcal species
7/36 (20%)
2
1
4
Anaerobic bacteria
Bacteroides fragilis group
1/36 (3%)
1
Enterococcus faecalis
Vancomycin resistant
3/36 (8%)
0
Other GNR
3/36 (8%)
• Dosing regimens for ertapenem were 1g administered once daily (n = 16),
or 2g administered once daily (n = 17). Mean length of treatment was
39.3 days (18-76).
• Approximately 27% experienced some adverse event. Nausea and
vomiting 3 (8%), eosinophilia 3 (8%), neutropenia 1(3%),
hyperbilirubinemia 1 (3%), and diarrhea 1 (3%).
Table 1: Demographic and laboratory data for 33 cases of
osteomyelitis treated with Ertapenem
_________________________________________________________________________________________________________________________
Exclusion Criteria for Primary Outcome:
Variable
• Those not receiving ≥2 continuous weeks of ertapenem
_________________________________________________________________________________________________________________________
Study Definitions and Outcomes:
1- Primary outcome:
- Clinical success = resolution of disease measured clinically and
with decreased ESR and CRP, without need for alteration in
antibiotic therapy or repeat surgical intervention
2- Secondary outcomes:
- Adverse events = enumerated and compared by dosing strategy
(1g daily versus 2 g daily) = side effects or laboratory aberrations in
patients on ertapenem
Statistics:
• Fisher’s exact test or Chi-squared test, as appropriate, for
comparisons between ertapenem dosing groups
• Clinical success was described as the number (%) of those
clinically evaluable who were coded as successes.
• Microsoft Excel™ 2010 was used for all calculations.
• P-values ≤0.05 were considered significant.
No./%ª
(n = 33)
Demographic data
Age, mean (SD)
49.6 (33)
Male sex
26 (79%)
Caucasian
25 (76%)
African-American
8 (24%)
Comorbidities
Hypertension
18 (55%)
Current smoker
12 (36%)
Diabetes
11 (33%)
Orthopedic hardware
10 (30%)
Peripheral neuropathy
8 (24%)
Peripheral arterial disease
6 (18%)
Chronic renal disease
2 (6%)
Current alcohol use
3 (9%)
Coronary artery disease
3 (9%)
Current steroid use
3 (9%)
Cirrhosis
1 (3%)
Site of Infection/Surgical intervention
Diabetic foot
9 (27%)
Other site
19 (57%)
Mandible
9 (27%)
PJI
3 (9%)
Septic arthritis
2 (6%)
Laboratory data upon diagnosis
WBC (cells/mm³), Median (IQR)
11.6 (3.5-21.9.)
ESR (mm/hr), Median (IQR)
62.82 (0-140)
CRP (mg/dl), Median (IQR)
8.91 (0.09-32.59)
Procalcitonin, Median (IQR)
0.77 (0.05-3.7)
--------------------------------------------------------------------------------SD: standard deviation; WBC: white blood cell count; IQR: interquartile range; ESR:
erythrocyte sedimentation rate; CRP: C-reactive protein.
ªAll values are given as No. (% of total patients) unless otherwise specified.
ªAll values are given as No. of a given isolate (% of total bacterial isolates).
CONCLUSIONS
•
Ertapenem appeared to be efficacious for the treatment of polymicrobial
osteomyelitis.
•
Ertapenem possesses a favorable safety profile, even with high doses.
•
These findings warrant further research describing ertapenem use in
bone infections.
REFERENCES
[1] http://www.invanz.com/ertapenem_sodium/invanz/hcp/index.xhtml
[2] Goswami ND, et al. Ertapenem for the treatment of osteomyelitis. BMC Research
Notes 2011, 4:478. http://www.biomedcentral.com/1756-0500/4/478
[3] Ramos A, Berbari E, Huddleston P. Diagnosis and treatment of Fusobacterium
nucleatum discitis and vertebral osteomyelitis: case report and review of the literature.
Spine . 2013 Jan 15; 38(2).
[4] Lee CH, Su LH, Lin WC, Tang YF, Liu JW. Refractory vertebral osteomyelitis due to
CTX-M-14-producing Escherichia coli at ertapenem treatment in a patient with a
coexisting urinary tract infection caused by the same pathogen. Int J Infect Dis. 2010
Sept; 14 (3).
[5] M. Chen, A et al. Comparative Pharmacokinetics and Pharmacodynamic Target
Attainment of Ertapenem in Normal-Weight, Obese, and Extremely Obese Adults.
Antimicrobial agents and chemotherapy, Apr. 2006, p. 1222–1227.