Branko N Huisa M.D.
Assistant Professor of Neurology
UNM Stroke Center
THE END!
CHANGABLE
NOT CHANGABLE
• Blood pressure
•Age
• Diabetes Mellitus
• Sex
• Hyperlipidemia
• Race
• Atrial fibrillation
• History of TIA or stroke
• Nicotine
• Family history of TIA/stroke
• Drug abuse
• Life style
Antihypertensive medication.
Diabetic control.
Tobacco cessation.
Antiplatelets.
Anticoagulants.
Statins.
Diet.
Exercise.
Education.
100%
78%
80%
65%
60%
48%
31%
40%
20%
0%
16%
6%
18-34
35-44
45-54
55-64
*Based on NHANES 19992000 data. Hypertension is defined as
blood pressure 140/90 mmHg or antihypertensive treatment.
Fields et al. Hypertension. 2004:44;398-404.
65-74
75+
Lancet 1990
BP
reductions
between
groups with
risks of
major
vascular
outcomes
and death
Lancet 2003
SBP difference between randomized groups (mm Hg)
Lancet 2002; 360: 1903–13.
Reduce 20mmHg systolic BP
Lancet 2002; 360: 1903–13.
Reduce 10mmHg diastolic BP
No severe hypertension. NNT=118
(DBP 90-110 mm Hg).
Moderate hypertension. NNT =52
(DBP at or below 115 mm Hg)
Severe hypertension. NNT=29
(DBP above 115 mm Hg)
Secondary prevention: NNT=110
(for patients with initial BP <160/90 mmHg and
reduction by 12/5 mm Hg) PROGRESS Lancet 2001
Aspirin
Aspirin Mechanism: (inhibits PG synthesis)
Inhibits PGH synthase pre- systemically.
Covalently acetylates Cyclo-oxygenase (irr.)
Inhibits platelet function by 1 hour.
Lasts entire platelet lifetime (~10d)
Efficacy is not in question.
Controversy:
o Dosage
o Aspirin resistance
Aspirin Dose No. of Trials OR (%)
500-1500 mg
160-325 mg
75-150 mg
<75 mg
34
19
12
3
19
26
32
13
Any aspirin
65
23
0
Odds Ratio
0.5
Antiplatelet Better
*Vascular events included nonfatal MI, nonfatal stroke, and death from vascular causes.
Treatment effect P<.0001.
Antithrombotic Trialists’ Collaboration. BMJ. 2002;324:71-86.
1.0
1.5
2.0
Antiplatelet Worse
Aspirin within 24hrs after CVA
CAST & IST:
Metaanalysis ~40,000 pts.
• ~99% of evidence from
randomized trials.
• Reduction of 9/1000 overall risk
of further
cva/ death in hospital.
• Reduction of 7/1000
ischemic cva. (p<0.000001)
* Starting ASA early reduces risk of
recurrent cva.
______________
Chen. Stroke 2000;31:1240.
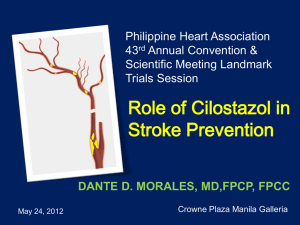
Clopidogrel
CAPRIE: (Clopidogrel vs ASA)
•Clopidogrel(75mg) ASA(325mg)
•19,185 pts. c h/o CVA/ MI/ PVD
•Incidence
5.83% (ASA)
5.32% (Clopidogrel)
* 8.7% (p=0.05) Relative RR.
______________
CAPRIE
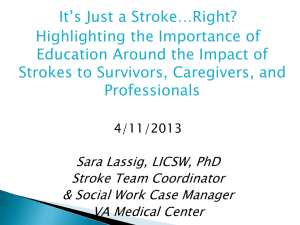
CAPRIE: Clopidogrel
Cumulative Event Rate
(Myocardial Infarction, Ischemic Stroke or Vascular Death)
8.7%*
Overall
relative
Risk
Reduction
p=0.043
Cumulative event rate (%)
16
ASA
(n=9,586)
12
Clopidogrel
(n=9,599)
8
4
0
0
3
6
9
12
15
18
21
24
27
30
33
Months of follow-up
*Intention to treat analysis
1. CAPRIE Steering Committee. Lancet 1996; 348: 1329–1339. 2. Antiplatelet Trialists'
Collaboration. BMJ 2002; 324: 71–86.
36
CAPRIE: Clopidogrel
Results:
•Overall safety = asa.
•Sl. more effective in
reducing end- points
(cva/mi/vasc.d)
•“all pt” result driven by
subset of PVD pts
______________
CAPRIE
CHARISMA
MATCH
Diener et al. Lancet 2004;364:331-337
Bhatt D et al. N Engl J Med 2006;354:1706-1717
Dipyridamole
30–325mg Aspirin and 200 Dipyridamole
BID versus 30-325mg Aspirin Alone
(ESPRIT)
n=2739 all with stroke or TIA
Dipyridamole stopped 470
ASA alone stopped 184
1% event reduction per year
ESPRIT Study Group. Lancet 2006;367:1665-1673.
•
•
•
ESPRIT is an un-blinded trial
• Patients and physicians were aware of applied
medication with potential bias
400 mg daily dipyridamole with different
formulations
• extended (modified) release
• immediate release
Aspirin dose from 30 to 325 mg
De Schryver et al. Cerebrovasc Dis. 2000;10:147-50.
PROFESS:
“There is no evidence to conclude superiority
of one antiplatelet therapy over other.”
“Antiplatelet therapy should be used for
secondary stroke prevention. NNT ≈ 100”
AHA Guidelines Stroke 2011
ACCORD NEJM 2008
ACCORD NEJM 2008
Tight Glucose control
Maybe
Tight BP control
YES!
UKPDS. BMJ 1998
Lower LDL cholesterol.
Modest increase of HDL cholesterol.
Improve endothelial dysfunction.
Increase NO.
Neuroprotective effect.
Anti‐inflammatory properties
Anti‐thrombotic effects
Immunomodulation
NEJM 2006
Huisa et al 2010
Based on SPARCL: NNT=46 in 5 years
High dose therapy with a reduction of
LDL>50% (NNT≈15 in 5 years)
16 trials on stroke prevention in AF (n=9874)
Warfarin reduced stroke by 62%
absolute reduction 2.7% for primary and 8.4% for
secondary prevention
Aspirin reduced stroke by 22%
absolute 1.5 and 2.5%
Hart RG, et al. Stroke 1999.
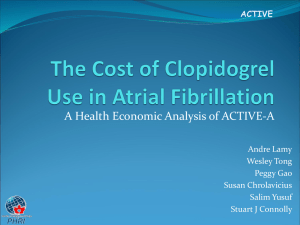
NEJM 2009
p=0.34
p<0.001
NEJM 2009
Schloten et al. Europace 2005
Patients who have AF but cannot take
warfarin
n=7,554
3.6 years
All received ASA
Major vascular events:
clopidogrel 6.8% / year, placebo
7.6% / year)
Stroke: clopidogrel 2.4% per
year, placebo 3.3% per year
Major bleeding: clopidogrel
2.0% per year, placebo 1.3%
per year
The ACTIVE Investigators. N Engl J Med 2009;10.1056/NEJMoa0901301
Cumulative Hazard Rates for the Primary Efficacy and Safety
Outcomes,According to Treatment Group
N Engl J Med 2011
Mediterranean
Low carbohydrate
Low Fat
EAT LESS LIVE LONGER!
N :322, BMI:31
Dietary
Intervention to
Reverse Carotid
Atherosclerosis
Shai et al. Circulation 2010
Morgestein et al. Ann Neurol 2009
RR(95% CI): 1.13 (1.02–1.25)
Average USA consumption
10.4 g of salt per mg
(CDC 2006)
Adult human body
requirements:
< 5.8 g of salt mg
(AHA 2010)
Ideal for stroke prevention
< 4 g of salt
Projected Annual Reductions in Cardiovascular Events Given
a Dietary Salt Reduction of 3 g per Day.
NEJM2010
NEJM2010
Eat more fresh foods, especially fruits and
vegetables
Purchase processed foods with low salt claims on
labels, or brands with the lowest % of daily sodium
intake on the food label.
Avoid heavily salted foods (pickled foods, olives,
salted crackers or snacks, process meats, etc).
Rinse canned foods with water before eating
Use less salt in home cooking and no added salt at
the table.
Antihypertensive medication.
Diet.
Statins.
Antiplatelets.
Exercise and body weight.
Tobacco cessation.
Diabetic control.
Anticoagulants for A-fib
Antithrombotics+high dose statins
+Diet&exercise+Tight BP control
Hackam, D. G. et al. Stroke 2007;38:1881-1885
Percentage of respondents unable to name
correctly 1 warning sign or risk factor.
Pancioli, A. M. et al. JAMA 1998;279:1288-1292
Copyright restrictions may apply.
Stroke 2011
Stroke 2011