Yes - Imedex

Should We Treat Smoldering Myeloma?
YES!
Lymphoma Myeloma 2014
Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida
Joseph Mikhael, MD, MEd, FRCPC, FACP
Staff Hematologist, Mayo Clinic Arizona
Additional Disclosures
•
There is no such thing as Mikhael
James R. Berenson, MD Oncology
•
I am not incorporated
• I am just the average Joe…
President and CEO - James R. Berenson, MD, Inc.
Medical & Scientific Director - Institute for Myeloma
& Bone Cancer Research (IMBCR)
Chief Executive Officer - Oncotherapeutics
Background
•
Remember Myeloma is a unique cancer – defined by the presence of organ damage – not just pathology
•
Traditionally we wait until CRAB
•
But does that really make sense? Do we have to wait until damage is present to intervene??
What if your friend is walking towards a cliff?
•
Will you wait until they are falling to rescue them?
•
What if they are running?
•
What if they are enjoying the walk?
My Thesis – there are 3 groups within
Smoldering Myeloma
• Group 1: “Ultra” High Risk
• Plasmacytosis ≥ 60%
• Involved/Uninvolved Light Chains ≥ 100
•
1 or more focal lesions on MRI/PET
TREAT AS IF TRUE MYELOMA
•
Groups 2: High Risk (Defn to follow)
DEBATE: To Treat or Not to Treat
•
Group 3: Low Risk
DON’T TREAT
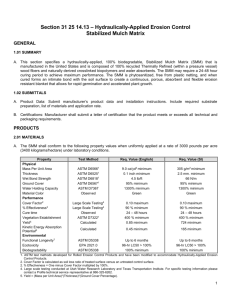
Smoldering Multiple Myeloma
Ultra-High Risk
• >60% BMPC
• FLCr >100
• >1 MRI focal lesions High-Risk SMM
25%/year
Low-risk SMM
5%/year
SMM Paradigm Shift
SMM 10% per year x 5 years
MGUS
~1% per year after 10 years
Ultra High Risk SMM = Active
Myeloma
Not CRAB but now SLiM CRAB
•
S (60%)
•
Li (Light chains I/U >100)
•
M (MRI 1 or more focal lesion)
•
C (calcium elevation)
•
R (renal insufficiency)
•
A (anemia)
•
B (bone disease)
Bone Marrow Plasma Cell ≥60%
Rajkumar SV et al. N Engl J Med 2011; N Engl J Med 2011; 365:474-475
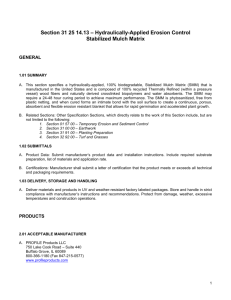
FLC Ratio >100 and Risk of progression to myeloma
>100
<100
Larsen J, et al. Leukemia advance online publication 27 November 2012; doi: 10.1038/leu.2012.296
Rajkumar SV, Merlini G, San Miguel JF. Nat Rev Clin Oncol 2012
High Risk SMM = Median TTP ~2 years:
• Mayo: SMM with M protein ≥3 gm/dL and ≥10% PCs
• Spanish: ≥10% PCs, Absence (<5%) of normal PCs by immunophenotyping and Immunoparesis of ≥1 immunoglobulins
•
Abnormal FLC ratio 8-100
•
Deletion 17p, t4;14, 1q amp
•
Evolving pattern
•
IgA SMM
• SMM with M protein ≥4 gm/dL
•
Increased circulating plasma cells
•
Increased plasma cell proliferative rate
Rajkumar SV, Merlini G, San Miguel JF. Nat Rev Clin Oncol 2012
Management of High Risk
SMM:
What does the data say?
Do we believe the Spanish
Trial?
Recall – Randomized, Phase 3
Trial of high risk SMM pts
Lenalidomide – dexamethasone vs observation
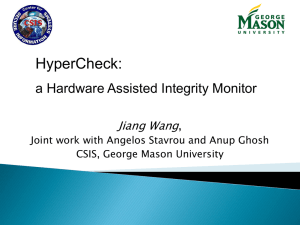
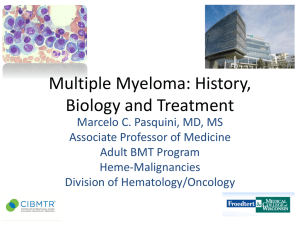
Len/Dex versus Observation in High Risk SMM: TTP
Mateos M et al. N Engl J Med 2013;369:438-447.
Len/Dex versus Observation in High Risk SMM: OS
Mateos M et al. N Engl J Med 2013;369:438-
447.
Issues with the Spanish Trial
1. Generalizability
– Mayo Criteria BMPC ≥ 10% and M-protein ≥ 30 g/L or
– Spanish Criteria BMPC ≥ 10% or M-protein ≥ 30 g/L and
– BM aPC/nPC > 95% and
– immunoparesis
– BUT note that 60% met Mayo Criteria!!
Mateos M et al. N Engl J Med 2013;369:438-447.
2. Tolerability
1.0
0.8
3. Consequences
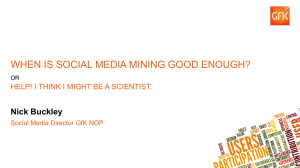
Len-dex vs. no treatment: TTP to active disease
(n = 119)
ITT analysis
Median follow-up: 32 months (range 12 –49)
Lenalidomide + dex
Median TTP: NR
9 Progressions (15%)
5 pts:early disc followed by PD
4 pts:symptomatic PD
0.6
0.4
0.2
No treatment
Median TTP: 23m
37 Progressions (59%)
20 patients: bone disease
7 patients: renal failure
0.0
0 5 10
Mateos. ASH 2012
HR: 6.0; 95% IC (2.9
15 20 25
Time from inclusion
30 35 40 45
–12.6); p < 0.0001
50
Spanish Trial Conclusions
•
Early intervention in high risk SMM
•
Prolongs TTP
•
Improves OS
•
Does not result in appreciable toxicity
•
Prevents irreversible damage to kidneys and bones that occur …
“on our watch!”
Conclusions
• Don’t forget new criteria ( SLiM CRAB ) for myeloma (Ultra High Risk SMM = Myeloma)
•
Low risk can be watched
•
High risk is complex
•
Recall 50/50 in 2 years
•
Consider therapy these patients in an individualized manner
•
Not limited to len-dex, but all active therapy