1 - Human muscular dystrophies and oxidative damage - 2012 - R Renjini - OxidativeDamageinMuscularDystrophyCorrelateswithth[retrieved 2016-11-06]
advertisement

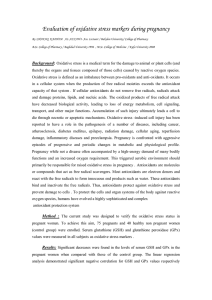
Neurochem Res (2012) 37:885–898 DOI 10.1007/s11064-011-0683-z ORIGINAL PAPER Oxidative Damage in Muscular Dystrophy Correlates with the Severity of the Pathology: Role of Glutathione Metabolism R. Renjini • N. Gayathri • A. Nalini M. M. Srinivas Bharath • Received: 1 December 2011 / Accepted: 20 December 2011 / Published online: 5 January 2012 Ó Springer Science+Business Media, LLC 2012 Abstract Muscular dystrophies (MDs) such as Duchenne muscular dystrophy (DMD), sarcoglycanopathy (Sgpy) and dysferlinopathy (Dysfy) are recessive genetic neuromuscular diseases that display muscle degeneration. Although these MDs have comparable endpoints of muscle pathology, the onset, severity and the course of these diseases are diverse. Different mechanisms downstream of genetic mutations might underlie the disparity in these pathologies. We surmised that oxidative damage and altered antioxidant function might contribute to these differences. The oxidant and antioxidant markers in the muscle biopsies from patients with DMD (n = 15), Sgpy (n = 15) and Dysfy (n = 15) were compared to controls (n = 10). Protein oxidation and lipid peroxidation was evident in all MDs and correlated with the severity of pathology, with DMD, the most severe dystrophic condition showing maximum damage, followed by Sgpy and Dysfy. Oxidative damage in DMD and Sgpy was attributed to the depletion of Electronic supplementary material The online version of this article (doi:10.1007/s11064-011-0683-z) contains supplementary material, which is available to authorized users. R. Renjini M. M. Srinivas Bharath (&) Department of Neurochemistry, National Institute of Mental Health and Neurosciences (NIMHANS), P.B # 2900, Hosur Road, Bangalore 560029, Karnataka, India e-mail: bharath@nimhans.kar.nic.in N. Gayathri Department Neuropathology, National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore 560029, Karnataka, India A. Nalini Department Neurology, National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore 560029, Karnataka, India glutathione (GSH) and lowered antioxidant activities while loss of GSH peroxidase and GSH-S-transferase activities was observed in Dysfy. Lower GSH level in DMD was due to lowered activity of gamma-glutamyl cysteine ligase, the rate limiting enzyme in GSH synthesis. Similar analysis in cardiotoxin (CTX) mouse model of MD showed that the dystrophic muscle pathology correlated with GSH depletion and lipid peroxidation. Depletion of GSH prior to CTX exposure in C2C12 myoblasts exacerbated oxidative damage and myotoxicity. We deduce that the pro and antioxidant mechanisms could be correlated to the severity of MD and might influence the dystrophic pathology to a different extent in various MDs. On a therapeutic note, this could help in evolving novel therapies that offer myoprotection in MD. Keywords Muscular dystrophy Duchenne muscular dystrophy Dysferlinopathy Sarcoglycanopathy Oxidative stress Glutathione Cardiotoxin Abbreviations NMD Neuromuscular disease MD Muscular dystrophy DMD Duchenne muscular dystrophy Sgpy Sarcoglycanopathy Dysfy Dysferlinopathy GSH Glutathione SOD Superoxide dismutase MDA Malondialdehyde 3-NT 3-Nitrotyrosine GCL Gamma glutamyl cysteine ligase GPx Glutathione peroxidase GR Glutathione reductase GST Glutathione-s-transferase CTX Cardiotoxin 123 886 ROS MTT DNPH PN Neurochem Res (2012) 37:885–898 Reactive oxygen species 3-(4,5-Dimethylthiazol-2-yl)-2,5diphenyltetrazolium bromide Dinitrophenyl hydrazine Peroxynitrite Introduction Neuromuscular diseases (NMDs) are myopathic disorders which arise due to defects in nerves, neuromuscular junctions or in the muscle fibers that they innervate [1]. Among these, muscular dystrophies (MDs) comprise the most frequently encountered genetic diseases that display loss of muscle integrity. The structure and function of the human skeletal muscle are critically dependent on the intactness of the sarcolemma which in turn is stabilized by several protein complexes [2]. The Dystrophin-Glycoprotein Complex (DGC) tethered to the sarcolemma is a transmembrane complex consisting of dystrophin, dystroglycans, sarcoglycans, syntrophins and other proteins [3]. The absence of specific proteins in the DGC compromises the sarcolemmal integrity thus causing muscle damage and MD. While recessive mutations in the dystrophin gene leading to the absence of dystrophin in the DGC cause Duchenne muscular dystrophy (DMD) (an X-linked disorder), Sarcoglycanopathies (Sgpy) are autosomal recessive limb girdle muscular dystrophies (LGMDs) resulting from deleterious mutations in the sarcoglycan genes (a,b,c and d). Similarly, mutations in Dysferlin, a transmembrane protein involved in membrane trafficking and repair, cause Dysferlinopathy (Dysfy) (LGMD-2B/Miyoshi myopathy). Although these MDs have comparable endpoints of muscle pathology involving cell death, adiposis, fibrosis etc., the onset, severity and the course of the diseases vary [4]. While Dysfy has a later onset (30–40 years), DMD and sarcoglycanopathies have early onset. Further, DMD patients exhibit significantly higher severity of clinical symptoms and dystrophic pathology compared to Sgpy and Dysfy. This indicates that distinct mechanisms exist downstream of genetic mutations in MDs that might alter the course and severity of dystrophic pathology but these pathogenic mechanisms remain elusive. Oxidative stress is one such mechanism implicated in MD but the contribution of this phenomenon has not been completely understood. In MD patients, altered antioxidant enzyme activities [5, 6], lowered activity of mitochondrial complexes [7] and NFkappaB activation [8] have been demonstrated. Systemic [9, 10] and muscle-specific [11] oxidative damage and altered anti-oxidant function have been reported in the muscles of DMD patients [12]. The mdx mouse model of DMD displays impairment of redox-sensitive metabolic enzymes [13], alteration in antioxidant enzyme activities 123 [14] and increased oxidative damage [14, 15]. Previous research on chick [16] and hamster [17] models of MD indicated elevated oxidative damage in the muscle. However, such studies in the models and disease samples of Sgpy and Dysfy and their comparison with DMD are scarce. In the current study, we have analyzed the markers of oxidative stress and antioxidant function in the muscle biopsies of patients with DMD, Sgpy and Dysfy to investigate and compare the contribution of these markers in muscle pathology. We have also generated mouse and myoblast cell models of MD and analyzed the role of oxidative damage in muscle pathology. Materials and Methods Bulk chemicals from Merck & Co. Inc (Whitehouse Station, NJ, USA) and Sisco Research Laboratories (Mumbai, Maharashtra, India), fine chemicals, anti-3-NT and antidinitrophenyl polyclonal antibodies, cardiotoxin (CTX) from Naja mossambica mossambica and protease inhibitor cocktail from Sigma (Eugene, OR, USA), nitrocellulose membrane from Millipore (Billerica, MA, U.S.A.), monoclonal antibodies against Dystrophin (1,2,3), Sarcoglycans (a, b, c, d) and Dysferlin from Novocastra Laboratories Limited (Newcastle Upon Tyne, UK) and HRP conjugated secondary antibodies from NCL and Bangalore Genei (Bangalore, Karnataka, India) were procured. Tissue Samples and Extraction Patients (n = 55) with muscle diseases were evaluated at the neuromuscular disorders Clinic of the National Institute of Mental health and Neurosciences (NIMHANS), Bangalore, India. Detailed clinical history of the patients was recorded. After obtaining the informed consent, biopsies were conducted by a neurologist, under local anaesthesia for adults and general anaesthesia for young children. A moderately weak muscle (biceps/vastus lateralis) free from previous trauma was selected for uniformity and submitted for routine diagnosis to the Department of Neuropathology, NIMHANS. A fragment of the fresh biopsy was snap-frozen in isopentane that was pre-cooled in liquid nitrogen. Fifty five muscle samples included immunohistochemically confirmed cases of DMD (n = 15), Dysfy (n = 15), Sgpy (n = 15) and healthy paraspinal muscle samples from patients with spinal corrections (control) (n = 10) (Table 1). The study protocol was approved by the Institutional Ethics Committee. For preparation of muscle extracts, frozen muscle tissue (50 mg) was minced in 10 volumes of 19 PBS containing protease inhibitors, homogenized and sonicated on ice for 30 s. The extract was centrifuged (14,000g, 10 min) and Neurochem Res (2012) 37:885–898 887 Table 1 List of samples utilized in the current study Sl. No. Disease Age (year) Gender (M/F) Sample number (n) 1 Control 28 ± 5 7/3 10 2 DMD 08 ± 3 15/0 15 3 Sgpy 10 ± 4 7/8 15 4 Dysfy 29 ± 5 12/3 15 and Material Science, Europa, GmbH) according to the manufacturer’s instructions. Cell Treatment and Viability Assay DMD Duchenne muscular dystrophy; Sgpy sarcoglycanopathy; Dysfy dysferlinopathy the supernatant was subjected to different assays after protein estimation [18]. Histological and Immunohistochemical Analyses A portion of the skeletal muscle biopsy oriented transversely was flash frozen in isopentane that was pre-cooled in liquid nitrogen. 8 lM thick serial cryosections were subjected to routine Haematoxylin-eosin (HE) staining and immunostaining for Dystrophin (1,2,3), Sarcoglycans (a, b, c, d) and Dysferlin [19]. Cell Culture C2C12 mouse myoblast cell line was grown in DMEM supplemented with 10% foetal bovine serum, penicillin (100 units/ml), streptomycin (100 lg/ml) and maintained at 37°C in a humidified atmosphere of 5% CO2/95% air [20]. Cells were sub-cultured via trypsin treatment. Differentiation of C2C12 myoblast cell line to myotubes was induced as follows: Upon reaching 100% confluency, cells were allowed to spontaneously differentiate for 6 days. Alternately, the culture medium was replaced with DMEM supplemented with 2% horse serum and antibiotics and allowed to differentiate for 6 days [20]. Differentiation was confirmed by the cellular morphology (differentiated cells were tubular compared to undifferentiated cells; data not shown) and by assaying the creatine kinase (CK) activity of total cell extracts as described earlier [21]. Cells (both differentiated and undifferentiated) were harvested and centrifuged (8509g, 1 min) and the pellet was resuspended in 19 phosphate buffered saline (PBS), pH 7.4, containing protease inhibitors. The cell suspension was sonicated on ice in a sonicator (Sonics and Materials Inc., CT, USA) (5 s each for 4 cycles) and centrifuged (15,0009g, 10 min, 4°C). The supernatant corresponding to the soluble extract were subjected to protein estimation by Bradford method [18]. The extract normalized for total protein was subjected to different biochemical assays including CK and oxidant/antioxidant assays. The CK activity was measured by a commercial kit (Olympus Life Cells were seeded in 96-well plates at a density of 5 9 103 or 5 9 102 for differentiated and undifferentiated cells respectively per well. After 24 h, the cells were exposed to buthionine sulfoximine (BSO) (inhibitor of glutathione (GSH) synthesis) immediately or after differentiation for 84 h. After 24 h of BSO exposure, the cells were treated with cardiotoxin (CTX) for 40 h. After the treatments, viable cells were measured using 3-(4,5-dimethylthiazol-2yl)-2,5-diphenyltetrazolium bromide (MTT) assay [22]. Briefly, 20 ll of 5 mg/ml MTT was added to cells and incubated at 37°C for 2 h. The medium was discarded, the dark blue formazan crystalline product was dissolved in dimethyl sulfoxide, and the absorbance was analyzed in a plate reader (Tecan) at 570 nm. Measurement of Reactive Oxygen Species (ROS) in Cells Total ROS in C2C12 cells was measured by a modified method of Ohashi et al. [23]. Briefly, the medium from treated or untreated C2C12 cells was replaced with 1 ml Locke’s solution (154 mM NaCl, 5.6 mM KCl, 3.6 mM NaHCO3, 5 mM HEPES, 2 mM CaCl2 and 10 mM Glucose, pH 7.4). Dihydrodichlorofluorescein diacetate (DCFDA) (10 lM) was then added and the cells were incubated at 37°C (10 min) in a CO2 incubator. The Locke’s solution was then removed and the cells were harvested. The cell pellet was washed with 19 PBS (pH 7.4) twice and reconstituted in lysis buffer (10 mM Tris– HCl containing 0.5% Tween-20). The lysate was centrifuged at 1,000g (10 min) and the fluorescence of the supernatant was measured (Excitation: 480 nm; Emission: 530 nm) [24]. In Vivo Model of MD All animal experiments were carried out in accordance with the institutional guidelines for the Care and Use of Laboratory Animals as per the internationally accepted principles for laboratory animal use and care. All the experiments involving animals were approved by the institutional animal ethics committee. Adult male C57BL/6 mice (10 week-old) (weight *30g each) (n = 6 for each treatment) were obtained from the Central Animal Research Facility, NIMHANS, Bangalore, India. Mice were housed five per cage with access to standard diet and water ad libitum in a well-ventilated room and all animals were exposed to 12 h light and dark cycle. Mice were injected either with saline 123 888 or CTX (single injection in saline; 300 ll of 10 lM per injection) across the tibialis anterior muscle on either of the hind limbs as described previously [25]. Care was taken to release the CTX uniformly along the muscle tissue by injecting the myotoxin while withdrawing the syringe needle. Twenty four hours and 14 days after the injection, the muscle from the ipisilateral and contralateral limbs were dissected and utilized either for histopathological or biochemical assays as described elsewhere in the methods section. Preparation of muscle extracts was carried out as described previously for the human samples. Neurochem Res (2012) 37:885–898 Assay of Oxidant Markers a nitrocellulose membrane followed by anti-3-NT western blot. Band intensities in westerns were quantified by a densitometric scanner using dedicated software (QuantityOne, BioRad laboratories, Hercules, CA, USA). To determine the specificity of the antibody, soluble protein extract was treated with Peroxynitrite (PN) at different concentrations as described earlier [29]. In brief, PN solution (0–1,000 lM) was placed on the wall of the tube containing the extract and vortex-mixed for a few seconds to ensure proper mixing before degradation of PN. Untreated and PN treated samples were spotted in triplicate onto a nitrocellulose membrane followed by anti-3-NT western blot. Estimation of Lipid Peroxidation SDS PAGE The tissue supernatant (100 ll) was added to 0.75 ml of acetic acid (pH 3.5), 0.1 ml SDS (8%) and 0.75 ml thiobarbituric acid (0.8%). The mixture was heated (45 min) and the adducts formed were extracted into 1.5 ml of 1-butanol followed by measurement of absorbance at 532 nm. The MDA concentration was calculated using the molar extinction coefficient (MEC) (241 mol/cm) and normalized per mg protein [26]. Total muscle protein extracts (*50 lg/lane) from control and MD tissues were run on 10% SDS PAGE stained with coomassie brilliant blue as described previously [30]. Estimation of Protein Carbonyls and Protein Nitration 10 ll of the supernatant (10 lg protein) was mixed with the buffer containing 30 mM Tris HCl buffer (pH 9.1), 0.5 mM EDTA, 50 mM TEMED and 0.05 mM quercetin. The rate of quercetin oxidation was monitored at 406 nm for 10 min [27, 31]. (1U SOD activity = amount of enzyme/mg protein that inhibits quercetin oxidation by 50%). The tissue supernatant (4 mg/ml protein) was derivatized by dinitrophenyl hydrazine (DNPH) in 12% SDS for 20 min at room temperature. The reaction was neutralized by 2 M Tris in 30% glycerol. Sample (5 ll) was spotted in triplicate onto a nitrocellulose membrane and subjected to anti-DNP western blot [27]. DNPH alone (without protein) and non-derivatized protein samples did not give anti-DNP signal indicating the specificity of the antibody. Alternately, the protein carbonyl content was determined by the spectrophotometric method described by Levine et al. [28]. Briefly, homogenate of the muscle tissue (10%) in 20 mM Tris–HCl–0.14 M NaCl (pH 7.4) was prepared and centrifuged at 10,0009g for 10 min at 4°C. To 100 ll of the supernatant, 100 ll of 20% trichloroacetic acid (TCA) was added and centrifuged at 10,0009g for 10 min at 4°C.The supernatant was discarded and the pellet was re-suspended in 1 ml of DNPH (10 mM in 2 N HCl) and kept in dark for 1 h with occasional mixing. To this mixture, 500 ll of 20% TCA was added to precipitate protein and the pellet was washed in 1 ml acetone and dissolved in 1 ml of 2% SDS prepared in 20 mM Tris HCl. The absorbance was read at 360 nm and the results were expressed as g moles carbonyls/mg protein using MEC22.0 mM-1 cm-1. To detect protein nitration (protein 3-nitrotysorine or 3-NT), 75 lg muscle protein was spotted in triplicate onto 123 Assay of Antioxidant Markers and GSH Metabolic Enzymes Superoxide Dismutase (SOD) Assay Catalase Assay The sample (50 ll) was mixed with 900 ll phosphate buffer (0.1 M, pH 7.0) and 50 ll of H2O2 (8.8 mM). The decrease in absorbance at 240 nm was followed for 5 min at room temperature and the enzyme activity was expressed as lmol H2O2 consumed/min/mg protein (MEC = 43.6 mM-1 cm-1) [32]. Estimation of Total Glutathione (GSH ? GSSG) The tissue sonicate or soluble cell extract was mixed with 5% sulfosalycylic acid, centrifuged (18,000g, 20 min) and 10 ll of supernatant was mixed with assay buffer (240 ll) [Phosphate–EDTA buffer containing 0.8 mM DTNB and 0.32U/ml glutathione reductase (GR)]. The reaction was initiated by 0.6 mM NADPH and the kinetics of 5, 50 -dithiobis (dinitrobenzoic acid) (DTNB) recycling was monitored at 412 nm for 5 min [27]. The GSH value was calculated based on the maximum reaction rate compared with GSSG Neurochem Res (2012) 37:885–898 standards. All estimations were conducted in triplicate and the values were normalized per mg protein. Glutathione Peroxidase (GPx) Assay The reaction mixture containing 10 ll supernatant, 0.1 M phosphate buffer, 0.5 mM EDTA, GSH reductase (0.24 U), GSH (2 mM) and NADPH (0.15 mM) was incubated at 37°C for 3 min and the reaction was initiated by the addition of tert-butyl hydroperoxide (0.12 mM) [33]. The change in absorbance at 340 nm was monitored for 5 min and the activity was expressed as nmoles of NADPH oxidized/min/mg protein (MEC = 6.22 mM-1 cm-1). Glutathione Reductase (GR) Assay To the reaction mixture (240 ll) containing Tris–HCl buffer (0.1 M, pH 8.8), 0.1 mM EDTA and NADPH (0.2 mM), 10 ll sample was added and the decrease in absorbance at 340 nm was monitored for 5 min. The enzyme activity was expressed as nmoles of NADPH oxidized/min/mg protein (MEC = 6.220 M-1 cm-1)[34]. Glutathione-S-Transferase (GST) Assay Sample (10 ll) was added to 240 ll of the reaction mixture containing 0.1 M phosphate buffer (pH 6.5), 0.5 mM EDTA, 2,4-dinitro benzene (CDNB) (1.5 mM) and 50 ll GSH (1 mM), and the absorbance at 340 nm was monitored for 5 min. The enzyme activity was expressed as nmoles of S-2,4, DNP-GSH formed/min/mg protein (MEC = 9.6mM-1 cm-1) [35]. Glutamate Cysteine Ligase (GCL) Assay Tissue supernatant (40 lg) was mixed with 100 mM Tris– HCl (pH 8.0), 150 mM KCl, 5 mM Na2ATP, 2 mM phosphoenol pyruvate, 10 mM l-glutamate, 20 mM MgCl2, 2 mM Na2EDTA and Pyruvate kinase/Lactate dehydrogenase mix (17U each) and the reaction kinetics was monitored at 340 nm for 10 min [36]. The reaction was initiated by the addition of 10 mM L-alpha aminobutyrate and the activity was normalized per mg protein. Thioredoxin Reductase (TrxR) Assay The reaction mixture containing 0.2 M phosphate buffer pH 7.4, 1 mM EDTA, 0.4 mM NADPH and sample (10 ll) was initiated by the addition of 10 ll of 2 mM DTNB and 5-thio-2-nitrobenzoic acid formed was measured at 412 nm. The activity of TrxR was expressed as nM of DTNB reduced/min/mg protein [37]. 889 Statistical Analysis Quantitative data were accumulated from at least three independent experiments and expressed as mean ± SD followed by the analysis of variance (ANOVA). In all the experiments, data with P \ 0.05 were considered to be statistically significant. Results Oxidative stress is implicated in muscle injury and MDs [13, 15, 38]. To investigate and compare the oxidative damage and antioxidant function and their contribution in different MDs, we tested the muscle biopsies from immunohistochemically confirmed cases of DMD, Sgpy, Dysfy and normal healthy controls (Table 1, Fig. 1). First we tested whether MD involves oxidative damage to muscle proteins. Analysis of protein nitration (indicated by total protein 3-nitrotyrosine/3-NT) in muscle extracts (75 lg total protein/spot) did not indicate significant change in any of the MDs compared to healthy controls (Fig. 2a, b). Control experiments with lower amounts of soluble protein extracts (15 lg/spot) treated with peroxynitrite (PN, a reactive nitrogen species that causes robust 3-NT modification in proteins) showed dose dependent (50–1,000 lM) increase in 3-NT signal compared to untreated control (Fig. 2c, d) indicating that the antibody was specific to protein 3-NT. On the other hand, protein oxidation levels (indicated by total protein carbonyls) were significantly elevated in all MDs with DMD showing maximum protein oxidation (*65% increase; P \ 0.001) followed by Sgpy (*50% increase; P \ 0.001) and Dysfy (*25% increase; P \ 0.05) (Fig. 2e, f). Control experiments carried out with DNPH alone (without protein) and protein alone (without DNPH treatment) did not give any western signal indicating that the antibody was specific to DNP-derivatized proteins (Fig. 2h). Analysis of protein carbonyls by an alternate approach (spectrophotometric method-see methods section) recapitulated the same trend in the data (Fig. 2i) as obtained in the slot blot method (Fig. 2e, f) thereby confirming the status of protein oxidation in the muscle samples. Quantitative analysis of lipid peroxidation indicated *3 fold increase in DMD (P \ 0.001) while it was increased by *2.5 and *2-fold in Sgpy (P \ 0.01) and Dysfy (P \ 0.05) respectively (Fig. 2j). Based on these data, oxidative stress was evident in different MDs with DMD, the most severe dystrophic condition showing maximum oxidative damage and Dysfy exhibiting the least damage. To analyze whether increased oxidative stress in MDs is linked with the antioxidant function, we assayed the 123 890 Neurochem Res (2012) 37:885–898 Fig. 1 Histopathological analyses of the muscle biopsies used for the study. Muscle biopsies from suspected cases of DMD (n = 15), Sgpy (n = 15), Dysfy (n = 15) and healthy controls (n = 10) were confirmed by histopathology. The figure shows the Haematoxylineosin (HE) staining and immunostaining for Dystrophin (DYS2), Sarcoglycan (Gamma-sarc) and Dysferlin in representative muscle biopsies of DMD, Gamma-Sgpy and Dysfy compared to control (magnification in all images = X400). All the MDs showed dystrophic pathology (indicated by HE staining) and loss of respective structural proteins (indicated by immunostaining) activities of the constitutive antioxidant enzymes in the muscle extracts. While the SOD activity was unaltered in DMD and Dysfy, it was decreased by *20% in Sgpy (P \ 0.01) (Fig. 3a). On the other hand, catalase activity was increased by *100% in DMD (P \ 0.01) and by *50% in Dysfy (P \ 0.001) while it was unchanged in Sgpy (Fig. 3b). However, Thioredoxin reductase activity was unaltered in all the three MDs compared to control (Fig. 3c). Since the variation in the antioxidant enzymes was not drastic enough to explain the oxidative damage in MDs, we tested whether the total GSH was altered. Total GSH was depleted by 50% in DMD (P \ 0.01) and by 40% in Sgpy (P \ 0.05), while it was unchanged in Dysfy compared to control (Fig. 4a, supplementary Fig. 1). We observed that the GSH depletion in DMD was due to *50% loss in the GCL activity (P \ 0.01) leading to decreased GSH synthesis (Fig. 4b). The GCL activity was increased by *30% in Dysfy (P \ 0.01) while it was unaltered in Sgpy. Next, we tested whether the antioxidant enzymes and metabolic enzymes associated with GSH were altered. The GPx and GST activities were drastically decreased in all the MDs (*50% decrease in Dysfy; *60% in DMD and by *70% in Sgpy compared to control; P \ 0.001 in all the three MDs) (Fig. 4c, d). However, GR activity was significantly increased in DMD (*40% increase compared to control; P \ 0.01) and Dysfy (*55% increase compared to control; P \ 0.05) while it was unaltered in Sgpy (Fig. 4e). Our data clearly correlated oxidative damage, GSH depletion and altered activities of GSH-metabolic enzymes with MD pathology in human samples. To confirm the contribution of GSH to muscle pathology under defined conditions, we generated CTX (from the venom of snake Naja mossambica mossambica) mouse model of MD (n = 6) as described earlier [25] and analyzed the status of oxidative stress and total GSH. In vivo injection with CTX (one injection with 300 ll solution of 10 lM CTX) into the tibialis anterior muscle caused transient but significant muscle cell damage and infiltration of inflammatory cells after 24 h (day 1; d1) compared to saline control (Fig. 5a), consistent with previous reports [25]. After 14 days of CTX injection (d14), there was significant recovery in muscle architecture (Fig. 5a), although most of the cells displayed centrally located nuclei. Interestingly, CTX-induced 123 Neurochem Res (2012) 37:885–898 A 891 B n1 n2 n4 n5 n7 n8 n10 f1 f3 f4 f6 f7 f9 f10 n1 n3 n4 n6 n7 n9 n10 f2 f3 f5 f6 f8 f9 n2 n3 n5 n6 n8 n9 f1 f2 f4 f5 f7 OD (AU) Protein 3-NT b f8 f10 b Control C 0 50 100 200 D Dysfy DMD Sgpy 2.5 2.0 OD (AU) Triplicate 250 500 750 1000 1.5 1.0 0.5 Triplicate 0 50 100 200 250 500 750 1000 PN (µM) E Oxyblot F n1 n3 n4 n6 n7 n9 n10 s2 s3 s5 s6 s8 s9 OD (AU) n1 n2 n4 n5 n7 n8 n10 s1 s3 s4 s6 s7 s9 s10 b n2 n3 n5 n6 n8 n9 s1 s2 s4 s5 s7 s8 s10 b Control H 1 2 3 4 5 6 7 8 MW (kDa) 96 66 42 Triplicate 30 DMD Control Dysfy DMD Sgpy Sgpy Lipid peroxidation µg MDA/mg protein J Dysfy I DMD Dysfy Sgpy Control nM protein carbonyls/mg protein G Control Dysfy DMD Sgpy Fig. 2 Quantitative analysis of oxidative markers in the muscle samples of MDs. Soluble extracts from DMD (n = 15), Sgpy (n = 15), Dysfy (n = 15) and healthy controls (n = 10) were used to compare the levels of different oxidant markers. a and b respectively show representative protein 3-NT blot (75 lg total protein per spot shown in duplicate per sample) and quantitation of nitrated proteins compared to controls; n = normal control; f = Dysfy; b = blank (no protein). c shows a control 3-NT dot blot of soluble protein extracts (15 lg/spot) treated with increasing PN (0–1,000 lM as indicated above each lane). d indicates the quantitation data of the slot blot from c. e A representative oxyblot for analysis of protein oxidation (10 lg derivatized protein per spot shown in duplicate per sample); n = normal control; s = Sgpy; b = blank (no protein). f shows the quantitation data of the slot blot from e. g shows the SDS PAGE profile of total muscle extracts from normal and MD samples indicating comparable protein used for slot blot experiments. h shows control oxyblot (dot blot) carried out with DNPH alone (without protein), protein alone (without DNPH treatment) and protein ? DNPH indicating that the antibody was specific to DNPderivatized proteins. i shows the quantitation of oxidized proteins by spectrophotometirc determination of DN-derivatized proteins. j represents estimation of lipid peroxidation (quantitated by TBARS) in different muscle samples compared with health controls. *P \ 0.05, **P \ 0.01 and ***P \ 0.001 compared to healthy controls in all the experiments 123 892 A C Dysfy DMD Sgpy Control Dysfy DMD Sgpy Thioredoxin reductase A Dysfy DMD Sgpy B Total GSH µg/mg protein) (µ Control C Dysfy DMD D DMD Sgpy nM of 2,4-DNP-GSH /min/ mg protein GST Control Dysfy DMD Sgpy Dysfy DMD Sgpy DMD Sgpy GR nM of NADPH oxidised /min/ mg protein nM of NADPH oxidised /min/ mg protein E Control Sgpy GPx Dysfy GCL nM of NADPH oxidised /min/ mg protein GSH Control 123 Catalase % Catalase activity % SOD activity Control Control Fig. 4 Analysis of GSH and related antioxidant and metabolic activities in muscle samples of MDs. Soluble extracts from DMD (n = 15), Sgpy (n = 15), Dysfy (n = 15) and healthy controls (n = 10) were used to compare the levels total GSH (a), GCL activity (b), GPx activity (c), GR activity (d), and GST activity (e). *P \ 0.05, **P \ 0.01 and ***P \ 0.001 compared to healthy controls B SOD nM DTNB reduced /min/mg Fig. 3 Assay of antioxidant enzymes in the muscle samples of MDs. Soluble extracts from DMD (n = 15), Sgpy (n = 15), Dysfy (n = 15) and healthy controls (n = 10) were used to compare the levels of different antioxidant enzymes. a Percentage differences in SOD activity among different MDs (100% SOD activity = 143.49 units/min/mg protein). b Percentage differences in catalase activity among different MDs (100% catalase activity = 2.86 nM of H2O2 converted/min/g protein). c corresponds to the thioredoxin activity assayed in different MDs. *P \ 0.05, **P \ 0.01 and ***P \ 0.001 compared to healthy controls Neurochem Res (2012) 37:885–898 Control Dysfy Neurochem Res (2012) 37:885–898 dystrophic muscle pathology at d1 correlated with *35% depletion in total GSH (P \ 0.001) and 12-fold increase in lipid peroxidation (P \ 0.001) in the muscle samples compared to controls (Fig. 5b, c). Following recovery of the muscle architecture at d14, the GSH and MDA content were restored to the level comparable with the saline control (Fig. 5b, c), thus linking GSH depletion, oxidative damage and muscle pathology. We recapitulated the same conditions in undifferentiated or differentiated C2C12 murine myoblast cell line [Differentiation in C2C12 cells into myotubes was confirmed by *3 fold increase in CK activity (P \ 0.01) (Fig. 6a) consistent with previous reports [21]. Dosedependent exposure to CTX (0–2 lM for 40 h) caused significant cell death with differentiated cells displaying increased vulnerability to the myotoxin compared to undifferentiated cells [LD50 = 2 lM (P \ 0.001) and 1 lM (P \ 0.001) for undifferentiated and differentiated cells respectively] (Fig. 6b). Next, we tested whether selective depletion of GSH prior to CTX exposure influenced myotoxicity. Accordingly, pretreatment with BSO (specific inhibitor of GCL that depletes GSH in a dose dependent manner) for 24 h (10 lM) followed by CTX treatment exacerbated cell death and this effect was more pronounced in differentiated cells (P \ 0.001) compared to undifferentiated cells (P \ 0.001) (Fig. 6c, d). However, exposure to BSO alone did not impinge on cell viability either in undifferentiated or differentiated cells indicating that GSH depletion combined with other toxic insults are required for cell death in muscle cells (Fig. 6e). Next we tested the status of total GSH and oxidative damage in the CTX cell model. Exposure to BSO alone (0–10 lM) caused dose dependent depletion of GSH both in differentiated and undifferentiated cells (Fig. 7a, b). Interestingly, treatment with CTX alone caused significant GSH depletion both in undifferentiated (*50% depletion at 2 lM; P \ 0.001) and differentiated cells (*75% depletion at 1 lM; P \ 0.001) compared to untreated cells and this was further depleted when the cells were pre-treated with BSO (Fig. 7c, d). In these cells, GSH depletion was associated with increased ROS (30% increase in undifferentiated cells, P \ 0.05; *5-fold increase in differentiated cells; P \ 0.001) compared to the respective controls (Fig. 7e, f). CTX-mediated GSH depletion and ROS accumulation was exacerbated by pretreatment with BSO (10 lM) and this was more pronounced in differentiated cells compared to undifferentiated cells. These data correlates GSH depletion, oxidative stress and muscle pathology with implications for MD. Discussion DMD, Sgpy and Dysfy are recessive NMDs characterized by a leaky sarcolemma resulting in muscle cell death [1]. 893 While DMD and Sgpy are early onset, rapidly progressive diseases, Dysfy is a late onset slowly progressive disorder [4]. There might be specific mechanisms underlying the clinical and pathological differences among these NMDs. Our study revealed varied dynamics of oxidative and antioxidant processes in different MDs which might contribute to the differences in these pathologies. We observed widespread oxidative damage that correlated with the severity of the pathology with DMD displaying maximum protein oxidation and lipid peroxidation followed by Sgpy and Dysfy (Fig. 2). The correlation between alterations in antioxidant function and the severity of MD has been previously suggested [39]. The mechanisms contributing to increased oxidative damage are quite dissimilar among the three MDs. Total GSH was considerably depleted in the rapidly progressive diseases DMD and Sgpy, compared to Dysfy, which represents chronic dystrophy. A recent study [40] not only suggested that low GSH hastens the onset of cardiomyopathy in mdx mice but also substantiated the role of GSH deficiency in DMD pathogenesis. Spassov et al. [41] demonstrated decreased GSH and GSSG content in the masticatory muscles of the mdx mice. Redox regulation of specific proteins contributes to the muscle function while dysregulation of redox-sensitive processes is linked to the loss of muscle mass and function during aging and MDs [42]. Dorchies et al. [43] demonstrated that natural antioxidants prevented oxidative damage, restored GSH content and protected against dystrophic pathology in the experimental models of DMD. In DMD and Sgpy, drastic depletion of GSH and significant reduction in GPx and GST activities contributed to oxidative damage. In addition, lowered SOD activity contributed to the pathogenesis in Sgpy. On the other hand, oxidative damage in Dysfy was contributed by lowered activities of GPx and GST (Figs. 3, 4). These events are either directly responsible for the pathological and clinical differences among the MDs or can occur in response to muscular degeneration. In DMD, GSH depletion was due to a significant decrease in the activity of the GSH synthesizing enzyme GCL (Fig. 4b). This is a novel observation with therapeutic implications in MDs. However, GSH depletion in Sgpy could not be explained by the GCL mechanism (Fig. 4b). The oxidative damage in Sgpy could be contributed partly via slight decrease in SOD activity and significant decrease in GPx and GST activities. Even though the GSH levels were unaltered in the Dysfy samples, decreased GST and GPx activities could contribute to the oxidative damage and muscle pathology. Further, lipid peroxidation in Dysfy could be attributed to the loss of GST activity (Fig. 2c) since soluble lipid peroxides are detoxified by conjugation with GSH via GST. The oxidant effects were relatively milder in Sgpy since the GSH levels 123 894 Neurochem Res (2012) 37:885–898 A Saline CTX d1 Saline CTX d14 1.4 GSH d14 GSH d1 1.2 1.2 1 *** 0.8 0.6 0.4 Total GSH (µg/mg protein) Total GSH (µg/mg protein) B 0.8 0.4 0.2 0 0 Saline 0.2 Lipid peroxidation d1 *** 0.15 0.1 0.05 0 0.10 MDA (ng/mg protein) MDA (ng/mg protein) C Saline CTX CTX Lipid peroxidation d14 0.08 0.06 0.04 0.02 0 Saline CTX Saline CTX Fig. 5 Analysis of histopathology, antioxidant and oxidant markers in CTX mouse model of MD. Muscle biopsies from saline injected and CTX injected animals (n = 6 each) were isolated after 24 h (day1; d1) or after 14 days (d14) and subjected to histopathology. a shows the Haematoxylin-eosin (HE) staining (Magnification = 400X) which indicates dystrophic pathology in CTX injected muscle at d1 (comparable to the human samples in Fig. 1) which was significantly restored at d14 compared to saline control. Dystrophic pathology in CTX muscle at d1 also correlated with depletion of total muscle GSH (b) and increased lipid peroxidation (c) which were restored to control levels by d14; ***P \ 0.001 compared to saline control were higher compared to DMD (Fig. 4a). However, GCL activity was unaltered indicating that the GSH loss might be contributed by other mechanisms such as formation of protein disulphides, and/or other GSH conjugates but these possibilities have to be supported by additional experiments. 123 Neurochem Res (2012) 37:885–898 D Differentiated Cell viability (% control) CPK activity (% control) A Undiff 2 % HS Control 10 % FBS CTX (1 µM) BSO BSO+CTX (10 µM) B Differentiated E Undifferentiated Differentiated Cell viability (% control) Cell viability (% control) Undifferentiated 0 1 2 0 1 2 CTX (µ µM) C 0 5 10 0 5 10 BSO (µM) Undifferentiated Cell viability (% control) Fig. 6 Effects of GSH depletion and CTX exposure in C2C12 muscle cell line. C2C12 cells were differentiated into myotubes and exposed either to CTX alone for 40 h or pretreated with BSO for 24 h followed by CTX treatment. Following different treatments, undifferentiated and differentiated cells were analyzed for cell viability. a differentiation of the C2C12 myoblasts into myotubes was confirmed by *3 fold increase in CK activity. b shows CTX (0–2 lM) dependent loss of cell viability in undifferentiated and differentiated C2C12 cells. c and d correspond to exacerbation of CTX myotoxicity by BSO (10 lM). e corresponds to the effect of BSO alone (5 and 10 lM) on cytotoxicity in undifferentiated and differentiated C2C12 cells. In all experiments, *P \ 0.05, **P \ 0.01 and ***P \ 0.001 compared to controls 895 Control CTX (2 µM) Most of the studies related to antioxidant enzymes in MDs have concentrated on DMD using human samples and mdx mice. But the data obtained from DMD studies are varied and are contradictory in some cases [5, 6, 9, 14]. DMD pathology was associated with chronic oxidative stress, impairment of the redox-sensitive metabolic enzymes [13], decreased activity of both MnSOD and Cu/ Zn SOD and increased activity of GPx and GST [5, 16]. On the contrary, several studies have reported unaltered or elevated activities of antioxidant enzymes and GSH in DMD compared to controls [9, 14, 16, 44]. The decreased activity of the antioxidant enzymes, GPx and GST shown in our study is in accordance with a recent report [45] which demonstrated the inhibition of these enzymes by reactive oxygen and carbonyl species in vitro. Although chronic oxidative stress was evident in DMD, Ragusa et al. [14] have suggested that it may not be the chief pathogenic mechanism. However, our data clearly showed increased oxidative damage, GSH depletion and decreased antioxidant function in DMD and Sgpy. This study is unique in that it has tried to correlate the oxidative damage and BSO BSO+CTX (10 µM) antioxidant function with the severity of the dystrophic pathology. Compared to DMD, there are limited reports linking oxidant and antioxidant markers with LGMD. Calpain-3 deficiency in the muscle might cause mitochondrial abnormalities leading to oxidative stress and energy deficit ultimately leading to pathology in calpainopathy [46]. Dioszeghy et al. [47] demonstrated that lipid peroxidation and SOD activity were not significantly altered in erythrocytes and muscle samples from patients with LGMD compared to controls. However, lipid peroxidation in the muscle from patients increased with the age of the patients and the duration of the disease. Treatment of the mouse model of Dysfy with antioxidants decreased the dystrophic markers and enhanced tissue integrity [48]. GSH depletion and oxidative stress have been associated with brain aging and different diseases including neurodegenerative diseases etc. [49]. In many cases, it is not clear whether upstream processes contribute to GSH depletion and oxidative damage or these events by themselves trigger cell damage. On the other hand, any 123 896 A B 0 1 2 5 7.5 0 10 1 BSO (µ µM) C 5 7.5 10 D GSH-differentiated Cells Total GSH (% control) Total GSH (% control) Control BSO CTX Control BSO+CTX BSO CTX BSO+CTX (10 µM) (1 µM) (10 µM) (2 µM) E 2 BSO (µM) GSH-Undifferentiated Cells F ROS-differentiated Cells AFU/cell) ROS-Undifferentiated Cells Control BSO (10 µM) contribution from oxidative damage to the dystrophic pathology cannot be ruled out. In MDs, interaction between the primary genetic mutation and free radical production has been proposed to contribute to the pathology (reviewed by Tidball and Wehling-Henricks [50]). Accordingly, free radical dynamics in the muscle could be altered by dystrophin deficiency in DMD via the proposed three mechanisms ultimately contributing to pathology: Firstly, altered production of free radicals can disrupt signaling pathways thus promoting muscle pathology. Next, in response to dystrophic pathology, muscle cells could alter the oxidant production which can further promote muscle damage. Thirdly, differences in individual responses and behavior could alter the generation and dynamics of free radicals in the muscle. However, the specific processes linking genetic mutations with oxidative damage are not completely delineated. In this study, we observed that the dystrophic pathology in DMD might decrease the total GSH via lowered GCL activity by undefined mechanisms (Fig. 4a, 123 GSH-differentiated Cells Total GSH (% control) Total GSH (% control) GSH-Undifferentiated Cells AFU/cell) Fig. 7 Effects of CTX and BSO exposure on total GSH and ROS in C2C12 muscle cell line. C2C12 cells (undifferentiated and differentiated) were exposed to BSO (24 h) and CTX (40 h) either alone or in combination followed by assessment of GSH content and ROS concentration. a and b dose dependent GSH depletion in undifferentiated and differentiated C2C12 cells by BSO (0–10 lM; 24 h); 100% GSH = 1.5 lg/mg protein both in undifferentiated and differentiated cells. c and d Total GSH level in C2C12 cells exposed to BSO alone or CTX alone or BSO for 24 h followed by CTX (40 h). e and f correspond to total intracellular ROS corresponding to DCF fluorescence (AFU = arbitrary fluorescence units). In all experiments, *P \ 0.05, **P \ 0.01 and ***P \ 0.001 compared to controls Neurochem Res (2012) 37:885–898 CTX (2 µM) BSO+CTX Control BSO (10 µM) CTX (1 µM) BSO+CTX b). To substantiate our claim on the role of GSH depletion and oxidative damage in muscle pathology, we generated cell and animal models of CTX. The muscle pathology observed following exposure to CTX was comparable to human MDs which included loss of muscle cell integrity and infiltration of neutrophils (Fig. 5a). CTX mediated muscle pathology in vivo is an accepted model for muscle damage/injury and dystrophy [51, 52]. CTX mediated dystrophy correlated with GSH depletion and oxidative stress (Fig. 5b, c). Following recovery of muscle structure (at 14 days after CTX exposure), the total GSH and MDA content in the CTX-injected muscles were restored to control levels directly correlating dystrophic pathology with GSH depletion and oxidative stress (Fig. 5). GSH depletion might be one of the events contributing to muscle pathology. This led us to test whether GSH depletion prior to the introduction of the myotoxin would exacerbate its toxicity. GSH depletion by BSO increased CTX toxicity and this was more pronounced in the differentiated cells Neurochem Res (2012) 37:885–898 since the GSH depletion was higher in these cells compared to undifferentiated cells (Figs. 6, 7). These data suggest that GSH depletion could underlie the dystrophic pathology in the human samples and drugs that boost GSH levels could have therapeutic implications for MD. But, as suggested earlier [50], in DMD, the interaction between dystrophin deficiency and oxidative stress in the dystrophic muscle is complex and may not be rescued by antioxidant therapy alone but probably in combination with other compounds including anti-inflammatory agents etc. We conclude that oxidative stress is an important mechanism among phenotypically and genotypically comparable pathologies, and the extent of damage significantly correlates with the severity of the disease. We presume that the structural and signaling alterations due to genetic mutations and loss of sarcolemmal proteins might trigger the interplay of pro-oxidant and anti-oxidant mechanisms to a variable extent. Studies on CTX cell and animal model demonstrated that GSH depletion and oxidative damage are closely associated with dystrophic muscle pathology. Further, GSH depletion prior to dystrophic insult might exacerbate myotoxicity with implications for MDs. On a therapeutic note, this phenomenon could help in evolving novel therapies to offer myoprotection against oxidative damage in MD. Acknowledgments This work was financially supported by the Department of Science and Technology, India. RR is a senior research fellow of the Council for Scientific and Industrial Research, India. The authors thank all the patients and their families for the muscle biopsies. RR and MMSB conceived the experiments. RR and NG carried out the experiments. AN carried out the clinical analysis. MMSB, RR and NG analyzed the data. RR and MMSB wrote the paper. References 1. Dubowitz V, Sewry CA (2007) Muscle biopsy—a practical approach, 3rd edn. Saunders Elsevier, London 2. Munoz P, Rosemblatt M, Testar X, Palacin M, Zorzano A (1995) Isolation and characterization of distinct domains of sarcolemma and T-tubules from rat skeletal muscle. Biochem J 307(Pt 1): 273–280 3. Rando TA (2001) The dystrophin-glycoprotein complex, cellular signaling, and the regulation of cell survival in the muscular dystrophies. Muscle Nerve 24(12):1575–1594 4. Emery AEH (1999) Neuromuscular disorders: clinical and molecular genetics. Wiley, England 5. Burr IM, Asayama K, Fenichel GM (1987) Superoxide dismutases, glutathione peroxidase, and catalase in neuromuscular disease. Muscle Nerve 10(2):150–154. doi:10.1002/mus.880100208 6. Kar NC, Pearson CM (1979) Catalase, superoxide dismutase, glutathione reductase and thiobarbituric acid-reactive products in normal and dystrophic human muscle. Clin Chim Acta 94(3): 277–280 7. Jongpiputvanich S, Sueblinvong T, Norapucsunton T (2005) Mitochondrial respiratory chain dysfunction in various neuromuscular 897 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. diseases. J Clin Neurosci 12(4):426–428. doi:10.1016/j.jocn. 2004.06.014 Haslbeck KM, Friess U, Schleicher ED, Bierhaus A, Nawroth PP, Kirchner A, Pauli E, Neundorfer B, Heuss D (2005) The RAGE pathway in inflammatory myopathies and limb girdle muscular dystrophy. Acta Neuropathol 110(3):247–254. doi:10.1007/ s00401-005-1043-3 Burri BJ, Chan SG, Berry AJ, Yarnell SK (1980) Blood levels of superoxide dismutase and glutathione peroxidase in Duchenne muscular dystrophy. Clin Chim Acta 105(2):249–255 Grosso S, Perrone S, Longini M, Bruno C, Minetti C, Gazzolo D, Balestri P, Buonocore G (2008) Isoprostanes in dystrophinopathy: evidence of increased oxidative stress. Brain Dev 30(6): 391–395. doi:10.1016/j.braindev.2007.11.005 Haycock JW, Mac Neil S, Mantle D (1998) Differential protein oxidation in Duchenne and Becker muscular dystrophy. Neuro Report 9(10):2201–2207 Nakae Y, Stoward PJ, Kashiyama T, Shono M, Akagi A, Matsuzaki T, Nonaka I (2004) Early onset of lipofuscin accumulation in dystrophin-deficient skeletal muscles of DMD patients and mdx mice. J Mol Histol 35(5):489–499 Dudley RW, Khairallah M, Mohammed S, Lands L, Des Rosiers C, Petrof BJ (2006) Dynamic responses of the glutathione system to acute oxidative stress in dystrophic mouse (mdx) muscles. Am J Physiol Regul Integr Comp Physiol 291(3):704–710. doi: 10.1152/ajpregu.00031.2006 Ragusa RJ, Chow CK, Porter JD (1997) Oxidative stress as a potential pathogenic mechanism in an animal model of Duchenne muscular dystrophy. Neuromuscul Disord 7(6–7):379–386 Dudley RW, Danialou G, Govindaraju K, Lands L, Eidelman DE, Petrof BJ (2006) Sarcolemmal damage in dystrophin deficiency is modulated by synergistic interactions between mechanical and oxidative/nitrosative stresses. Am J Pathol 168(4): 1276–1287; quiz 1404-1275. doi:10.2353/ajpath.2006.050683 Murphy ME, Kehrer JP (1986) Activities of antioxidant enzymes in muscle, liver and lung of chickens with inherited muscular dystrophy. Biochem Biophys Res Commun 134(2):550–556 Salminen A, Kihlstrom M (1989) Increased susceptibility to lipid peroxidation in skeletal muscles of dystrophic hamsters. Experientia 45(8):747–749 Bradford MM (1976) A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal Biochem 72:248–254 Renjini R, Gayathri N, Nalini A, Srinivas Bharath MM (2011) Analysis of Calpain 3 protein in muscle biopsies of different muscular dystrophies from India. Indian J Med Res (in press) Hsu DK, Guo Y, Alberts GF, Copeland NG, Gilbert DJ, Jenkins NA, Peifley KA, Winkles JA (1996) Identification of a murine TEF-1-related gene expressed after mitogenic stimulation of quiescent fibroblasts and during myogenic differentiation. J Biol Chem 271(23):13786–13795 Ardite E, Barbera JA, Roca J, Fernandez-Checa JC (2004) Glutathione depletion impairs myogenic differentiation of murine skeletal muscle C2C12 cells through sustained NF-kappaB activation. Am J Pathol 165(3):719–728 Vali S, Mythri RB, Jagatha B, Padiadpu J, Ramanujan KS, Andersen JK, Gorin F, Bharath MM (2007) Integrating glutathione metabolism and mitochondrial dysfunction with implications for Parkinson’s disease: a dynamic model. Neuroscience 149(4):917–930. doi:10.1016/j.neuroscience.2007.08.028 Ohashi T, Kakimoto K, Sokawa Y, Taketani S (2002) Semiquantitative estimation of heme/hemoprotein with dichlorodihydrofluorescin diacetate. Anal Biochem 308(2):392–395 Harish G, Venkateshappa C, Mythri RB, Dubey SK, Mishra K, Singh N, Vali S, Bharath MM (2010) Bioconjugates of curcumin display improved protection against glutathione depletion 123 898 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. Neurochem Res (2012) 37:885–898 mediated oxidative stress in a dopaminergic neuronal cell line: implications for Parkinson’s disease. Bioorg Med Chem 18(7):2631–2638. doi:10.1016/j.bmc.2010.02.029 Kherif S, Lafuma C, Dehaupas M, Lachkar S, Fournier JG, Verdiere-Sahuque M, Fardeau M, Alameddine HS (1999) Expression of matrix metalloproteinases 2 and 9 in regenerating skeletal muscle: a study in experimentally injured and mdx muscles. Dev Biol 205(1):158–170. doi:10.1006/dbio.1998.9107 Ohkawa H, Ohishi N, Yagi K (1979) Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal Biochem 95(2):351–358 Mythri RB, Venkateshappa C, Harish G, Mahadevan A, Muthane UB, Yasha TC, Srinivas Bharath MM, Shankar SK (2011) Evaluation of markers of oxidative stress, antioxidant function and astrocytic proliferation in the striatum and frontal cortex of Parkinson’s disease brains. Neurochem Res 36(8):1452–1463. doi:10.1007/s11064-011-0471-9 Levine RL, Garland D, Oliver CN, Amici A, Climent I, Lenz AG, Ahn BW, Shaltiel S, Stadtman ER (1990) Determination of carbonyl content in oxidatively modified proteins. Methods Enzymol 186:464–478 Mythri RB, Jagatha B, Pradhan N, Andersen J, Bharath MM (2007) Mitochondrial complex I inhibition in Parkinson’s disease: how can curcumin protect mitochondria? Antioxid Redox Signal 9(3):399–408. doi:10.1089/ars.2007.9.ft-25 Sambrook J, Russell DW (2001) Molecular cloning, a laboratory manual, 3rd ed edn. Cold spring Harbor Laboratory Press, New York Bagnyukova TV, Storey KB, Lushchak VI (2003) Induction of oxidative stress in Rana ridibunda during recovery from winter hibernation. J Therm Biol 28(1):21–28. doi:10.1016/s03064565(02)00031-1 Aebi H (1984) Catalase in vitro. Methods Enzymol 105:121–126 Flohe L, Gunzler WA (1984) Assays of glutathione peroxidase. Methods Enzymol 105:114–121 Carlberg I, Mannervik B (1985) Glutathione reductase. Methods Enzymol 113:484–490 Guthenberg C, Alin P, Mannervik B (1985) Glutathione transferase from rat testis. Methods Enzymol 113:507–510 Seelig GF, Meister A (1985) Glutathione biosynthesis; gammaglutamylcysteine synthetase from rat kidney. Methods Enzymol 113:379–390 Hill KE, McCollum GW, Burk RF (1997) Determination of thioredoxin reductase activity in rat liver supernatant. Anal Biochem 253(1):123–125. doi:10.1006/abio.1997.2373 Brancaccio P, Lippi G, Maffulli N (2010) Biochemical markers of muscular damage. Clin Chem Lab Med 48(6):757–767. doi: 10.1515/cclm.2010.179 Degl’Innocenti D, Rosati F, Iantomasi T, Vincenzini MT, Ramponi G (1999) GSH system in relation to redox state in dystrophic skin fibroblasts. Biochimie 81(11):1025–1029 Khouzami L, Bourin MC, Christov C, Damy T, Escoubet B, Caramelle P, Perier M, Wahbi K, Meune C, Pavoine C, Pecker F (2010) Delayed cardiomyopathy in dystrophin deficient mdx 123 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. mice relies on intrinsic glutathione resource. Am J Pathol 177(3):1356–1364. doi:10.2353/ajpath.2010.090479 Spassov A, Gredes T, Gedrange T, Pavlovic D, Lupp A, KunertKeil C (2010) Increased oxidative stress in dystrophin deficient (mdx) mice masticatory muscles. Exp Toxicol Pathol. doi: 10.1016/j.etp.2010.04.006 Jackson MJ (2008) Redox regulation of skeletal muscle. IUBMB Life 60(8):497–501. doi:10.1002/iub.72 Dorchies OM, Wagner S, Buetler TM, Ruegg UT (2009) Protection of dystrophic muscle cells with polyphenols from green tea correlates with improved glutathione balance and increased expression of 67LR, a receptor for (-)-epigallocatechin gallate. Biofactors 35(3):279–294. doi:10.1002/biof.34 Jackson MJ, Brooke MH, Kaiser K, Edwards RH (1991) Glutathione depletion during experimental damage to rat skeletal muscle and its relevance to Duchenne muscular dystrophy. Clin Sci (Lond) 80(6):559–564 Lesgards JF, Gauthier C, Iovanna J, Vidal N, Dolla A, Stocker P (2011) Effect of reactive oxygen and carbonyl species on crucial cellular antioxidant enzymes. Chem Biol Interact 190(1):28–34. doi:10.1016/j.cbi.2010.12.028 Kramerova I, Kudryashova E, Wu B, Germain S, Vandenborne K, Romain N, Haller RG, Verity MA, Spencer MJ (2009) Mitochondrial abnormalities, energy deficit and oxidative stress are features of calpain 3 deficiency in skeletal muscle. Hum Mol Genet 18(17):3194–3205. doi:10.1093/hmg/ddp257 Dioszeghy P, Imre S, Mechler F (1989) Lipid peroxidation and superoxide dismutase activity in muscle and erythrocytes in adult muscular dystrophies and neurogenic atrophies. Eur Arch Psychiatry Neurol Sci 238(3):175–177 Potgieter M, Pretorius E, Van der Merwe CF, Beukes M, Vieira WA, Auer RE, Auer M, Meyer S (2011) Histological assessment of SJL/J mice treated with the antioxidants coenzyme Q10 and resveratrol. Micron 42(3):275–282. doi:10.1016/j.micron.2010. 10.001 Bharath S, Hsu M, Kaur D, Rajagopalan S, Andersen JK (2002) Glutathione, iron and Parkinson’s disease. Biochem Pharmacol 64(5–6):1037–1048 Tidball JG, Wehling-Henricks M (2007) The role of free radicals in the pathophysiology of muscular dystrophy. J Appl Physiol 102(4):1677–1686 Vidal B, Serrano AL, Tjwa M, Suelves M, Ardite E, De Mori R, Baeza-Raja B, Martinez de Lagran M, Lafuste P, Ruiz-Bonilla V, Jardi M, Gherardi R, Christov C, Dierssen M, Carmeliet P, Degen JL, Dewerchin M, Munoz-Canoves P (2008) Fibrinogen drives dystrophic muscle fibrosis via a TGFbeta/alternative macrophage activation pathway. Genes Dev 22(13):1747–1752. doi:10.1101/ gad.465908 Yuasa K, Hagiwara Y, Ando M, Nakamura A, Takeda S, Hijikata T (2008) MicroRNA-206 is highly expressed in newly formed muscle fibers: implications regarding potential for muscle regeneration and maturation in muscular dystrophy. Cell Struct Funct 33(2):163–169