What Is Ease of Use? - Industrial Designers Society of America
advertisement

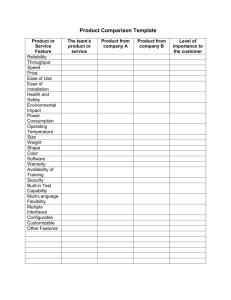
What Is Ease of Use? Mary Beth Privitera, IDSA, University of Cincinnati Introduction Virtually every product development effort, and student project, states “easy to use” as an overarching goal of the design. Answering the question “by whom should it be easy to use?” is usually fairly straightforward. However, determining what ease of use really means to the user and how to assess the “ease of use” for a new device can be a challenge. This assessment with tangible measures for ease of use keeps a multidisciplinary design team focused on the importance of ease of use among other requirements. This paper defines ease of use as the ability of a user to readily and successfully perform a task with a product without the need for an advanced explanation and/or the instruction manual, as determined through selected articles in the design literature and countless interviews with medical personnel, students and medical residents. By assessing the simplicity, obviousness, clarity, and time, better measure of ease of use can be determined. In addition, this paper summarizes the relationship of the learning curve with the product’s perceived “ease of use.” Although this paper focuses on medical device design, principles of ease of use remain the same despite the product focus. The goal of this paper is to explore the defining aspects of “ease” and serve as a helpful guide for designers. “User Friendly” Ease of use, user friendliness, user experience, and usability are intertwined with some overlapping definitions. In general, appropriate device interactions are perceived as more “user friendly” when the design of the device itself is closely matched with the goal of the user and ultimately its usability. While the term “user friendly” has no widely accepted definition within various professional societies, it is associated with usability or the ease in which a user can learn to use the device. Usability can be defined as the user’s perception of the effectiveness (fit and purpose) and efficiency (time required) of the product. Determining the usability of a device considers how easy it is to learn to use the device, the efficiency of use, how easy it is to remember how to use the device in the future, and the number of noncatastrophic errors that result, as well as the user’s subjective satisfaction level. The user experiences of some devices are easier to analyze empirically than others. Conducting usability testing is an industry standard as well as a global requirement, but it does not necessarily mean that the design team “knows” the user nor can it prove that a device is “easy to use” for all users. Usability testing verifies that a device can be used and is helpful in determining the shortfalls of a particular design. Certainly these shortfalls can be mitigated through the application of compensatory strategies but a better approach is to avoid the need for these strategies during the early phases of design. This requires a clear of understanding of what defines ease of use in the context of the user. Simplicity Simplicity is the freedom from complexity, intricacy, or division into parts. Device simplicity can be measured in both the functional characteristic, such as breaking down device interaction into discrete stages, and analyzing the number of steps in all use scenarios for successful device interaction. As clinical procedures increase in complexity, devices and their required interactions by the users also become more challenging. Certainly it is agreed that these use environments are chaotic in nature with multiple types of people interacting each with a unique set of challenges, priorities and goals. Figure 1. Breaking down the elements of the user interaction into specific human device inputs to device outputs such as modeling how the device acts on tissue, affords the design team to develop subtle improvements to each stage or element of the design therefore improving the entire use. For example, the decisions to make a device larger or smaller, one or two handed, or with a control panel consisting of a touch screen or a button impacts the practitioner’s perception of “ease of use.” While these decisions are made with diligence with regard to overall value and cost considerations, it is important to assess how each individual decision impacts the overall use scenario with regards to complexity. In the following sketch, ID student Ming Hsieh breaks down the removal of stem cells from the placenta in both a literal and figurative manner. These sketches assist the design team in understanding the interaction of the device, the user and the clinical goal. (Figure 2 and 3.) Figure 2. Literal representation. Figure 3. Figurative action. Positive user experiences are affected by visual design or graphic user interfaces as well as the physical form of the device. Proper GUI interfaces have the ability to walk users through the steps, making complex functions easy and facilitating comprehensive and effective performance. They can guide users to make better decisions during device use, and react more quickly and naturally. In addition, they allow users to rely on the device for clues with regard to the use sequence and do not tax the user memory. This is especially important if the device is infrequently used. Obviousness All users recognize obviousness as that which is easily seen, recognized, or understood. In effect the use interaction and purpose of a device is immediate and evident. If a user requires an explanation of how to complete something, it is not obvious. User interactions with medical devices are as varied as the spectrum of medical devices themselves. There is a physical interaction where the device itself is a natural extension of the body, which allows the practitioner to complete a clinical task that he/she would otherwise be unable to do. When a device use is obvious, the practitioner is able to achieve their clinical goal without hesitation and/or difficulty, and use of the device becomes as natural as taking a breath. Using form semantics, the physical shape of the device can lead users to logical conclusions as to where they should place their hands, and control and manipulate the device. When the overall shape is ambiguous, users can become confused. Through means of observation the obviousness can be determined by watching closely during the predetermined stages of use for challenges as communicated by the user both verbally and non-verbally without prompts. To avoid subjectivity, a scale of acceptability or range of user interaction should be developed. For example, noting where a hand interacts with a device at the initial onset and correlating this to the design intent will determine if the physical shape truly communicates proper use as designed. This coupled with noting challenges through facial expression and inadvertent motions will provide indication of the areas of design success and/or failure. In figures 4 and 5, the design team assesses obviousness with nursing staff in the context of use. These images show a model of a device to noninvasively measure bilirubin and hemoglobin for the detection of jaundice. Figure 4. Figure 5. Models such as these were provided to nursing staff for evaluation in the use environment. The multidisciplinary design team evaluated models based upon user recognition without instruction and the overall interaction of the device with the user and the infant. This effort was led by third-year design student Sally Pipkin. Clarity Clarity is defined as the clearness as to the perception or understanding a user has when using a device. As a user completes tasks with a device it is free from ambiguous states and serves as a feedback mechanism in itself. During a medical procedure involving the use of a new device, all users seek the following information: • How do I know if I have done something (beneficial or harmful)? • What can I see? • What do I need to achieve my clinical goal? • What is my next step? The answers to some of the preceding questions can be answered with feedback from the device such as a GUI screen or audible tone. Depending upon the experience level of the user this feedback may or may not be considered. Often expert users will turn off cautionary alarms and guide the procedure through intuition with experience gained through practice. This experience results in the development of procedural shortcuts that are used to complete the task in as few steps as possible while producing the same result. Based upon ideal application of human factors, devices or products will provide multimodal feedback that a user has actually done something. This is an area where if the user is not provided enough feedback they become confused and if there is too much feedback, device use becomes annoying. Time Certainly time is the easiest measure of use ease. However some things aren’t meant to be expedient and do take time for completion. For example, in medical devices I personally do not want my surgeon to necessarily complete tasks in a hurried manner, rather a thoughtful and purposeful one. This requires the design team to set limits of acceptability for time. In Figure 6, an existing device for bilirubin measurement is benchmarked regarding the overall time of use and the time of the diagnostic test to gather data. This sets parameters for the team with measureable and definable criteria. Figure 6. What Does Learning Have to Do with It? It is common to hear that a medical device has a “steep” learning curve, meaning that the device is difficult to use and that a short one means that it is in effect easy to use. While this may be reasonable given a particular complex clinical goal such as placing coils in intracranial aneurysms, the shortest possible learning curve is always best. This is the result of making it easier for the user to do the right thing and difficult to do the wrong thing coupled with the determination as to what the learning curve actually represents. The Learning Environment Affects What and How Users Learn The environment in which physicians learn to use a medical device is different for public, private, military, and civilian institutions. The biggest difference between these learning environments involves the types of injuries treated and access to supplies and experts. The reputation and size of the clinical department can also have an effect. Regardless of training environment, the more hands-on experience a user gets, the better the performance will be when using a device. Learning environment plays an important role. For example, medical residents do not typically learn to intubate in emergency situations, rather they use a staged process beginning with a clinical skills lab and advance into the OR where conditions are controlled and the clinical situation is more stable. Figure 7 depicts students learning to intubate in the clinical skills lab. Here, students first observe an expert then complete a hands-on simulation. Figure 7. The use of simulators, as shown in Figure 7, is widely accepted but far from ideal as the simulator does not replicate the forces and patient tissue interactions a user will experience during an actual procedure with a patient. For example, during an actual intubation procedure, the patient may be injured (preventing neck movement) and the patient’s oral environment will be more lubricious. What Is the User’s Background? Novice vs. Expert While many health care practitioners are excited about new innovations at the interface of technology and biology, they are also concerned about their ability to act appropriately when procedures do not go as planned. This is especially true with novice users. Novice users range from the most inexperienced medical students and modestly trained EMT personnel to seasoned professionals learning to employ an innovative new technology. Even though these users have had significantly different experiences, they all have the same initial lack of familiarity with new devices. Novice users are concerned with the following questions: • What if it breaks? • What if I am using the device inappropriately? • What if I read a measurement/diagnostic test incorrectly? Many devices have more than one method of operation and are designed specifically with this freedom of practice in mind. Thus, experienced users may each follow a slightly different procedure when using the same medical device. These modified approaches have not yet been explored by novice users and therefore are open to interpretation and exploration. Mentors, Role Models, and People We Emulate We all have people we consider to be experts and do our best to learn their techniques, tips and suggestions. When users have an opportunity to work alongside and/or be trained by these people, the learning advances rapidly and personal biases are transferred. In the example of physician training, it requires medical residents to observe and mimic those who are proficient. Learning why experienced users do what they do and when they do it is paramount to learning new techniques and follows a cycle of proficiency that includes 1) reading about a procedure, 2) observing the procedure being performed, and 3) teaching others how to perform the procedure. How Do Users Learn? Users learn at different rates, through different means, and in different orders of events. Initially they develop preconceived notions of how a device works. This may be the result of a brief exchange during a medical society meeting, a conversation with a trusted colleague, or through a blog. Once formed, this initial perception is difficult to change as it will most likely include stereotypes or simplifications. Making use of existing knowledge of clinical goals and building upon perceptions can be advantageous to device designers and clinical trainers. The second step in learning is the development of competence. This includes taking the foundation of factual knowledge in the context of a conceptual framework and applying it. Specifically moving a user from initial explorations to planning tasks, noticing patterns, generating explanations, and drawing analogies to other problems that are closely aligned with their personal factual knowledge helps develop competence in users of medical devices. As users develop expertise they develop metacognitive behavior. Here, they have the ability to describe why something will or will not work while completing a task. This is often evident in those physicians who are particularly adept at explaining complex procedures while performing them. They also possess the ability to effectively teach others and are most typically the thought leaders highly sought by industry. Learning Affect The learning affect as described in the literature is that the more a task has been performed the less time will be required to perform the task again. It is closely related to the experience curve effect that expresses the relationship between experience and efficiency. Simply stated, as the user experience increases so does the user’s efficiency (e.g., practice makes perfect). The same is true for device use. It is difficult to practice surgery before one becomes a medical student or surgeon. Each patient is different and although imaging is greatly helpful, practitioners have no idea how a patient’s body will respond to the given therapy until it is tried. To improve performance, the use of surgical simulators has increased. This is a great innovation; however, they typically lack the fidelity of human tissue and it is this tissue response feedback that guides a majority of intraoperative decision making. There are several reasons for this affect, including 1. Personal efficiency: Users are physically more dexterous and mentally more confident, and they spend less time hesitating, learning, experimenting, or making mistakes. They develop shortcuts and improvements that not only reduce procedure time but can also reduce fatigue. 2. Development of standard procedures: Each time a user performs the task with a tool he/she develops a standard protocol of how they personally complete the task. 3. Technology guidance: Here the user is walked through device use either through simulations or throughout the actual procedure. The device serves as a memory aid to the user by providing an “on demand” sense of procedural or device use progression. 4. Knowledge transfer: Users can learn to use similar devices more quickly based upon previous exploration and experimentation. Here, the user transfers knowledge of use from one device to the other. Within various subspecialties of medical devices and consumer products there are some generally accepted modus operandi such as the brake pedal is always on the right, which should be followed. Recognizing these and how to incorporate them into a novel device design can speed the learning process. Conclusion Ease of use should be simple, obvious, clear, and timely for every user and every product. Knowing the user, specifically what similar devices they have previously used, who their mentors are, and their experience level can assist in writing specific measureable criteria for ease of use. This is the foundation of product ease of use. Limit the number of steps for product use to complete what needs to be completed. Make the critical aspects of the device design self-evident as determined through the eyes of the user. In addition, where possible, conform to known standards within the context of the device design, seeking information regarding users’ quirks, beliefs, and experiences as early as possible in the design process without discarding learned behaviors. Provide clear feedback to the users as to the product use state throughout its use. Finally, all of our lives are busy; consider the time for learning, how users learn and what affects the rapid advancement from novice to expert for product use. From the above, determine measures, such as notable frustration as indicated by facial expressions and/or time to maintain the importance of ease of use among the other design criteria. While some designers may argue that ease of use is inherently subjective and should be left alone, our counterparts in business and engineering require tangible measures as a confirmation of a positive verbal expression. Acknowledgments Sally Pipkin, fourth-year industrial design student in the Medical Device Innovation Program; Ming Hsieh, fifth-year industrial design student in the Medical Device Innovation Program; and Jay Goldberg, Marquette University, Biomedical Engineering References Bransford, J., & Brown, A. L., (2000). How people learn: brain, mind, experience, and school: expanded edition. National Research Council (U.S.) Committee on Learning Research and Educational Practice, National Research Council. Donovan, M. S., Bransford, J., & Pellegrino, J. W. (2000, June). How people learn: Bridging research and practice. National Research Council. The Learning Curve, http://library.thinkquest.org/C005704/index.php3 Zull, J. (2002). The art of changing the brain: enriching the practice of teaching by exploring the biology of learning.