1 2 3 4
advertisement

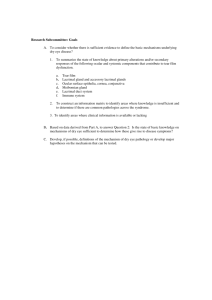
1 2 TITLE: TEAR BREAK-UP TIME FOR TEAR FILM EVALUATION: ARE MOISTENING SOLUTIONS INTERCHANGEABLE? 3 4 5 6 AUTHORS: Carme Serés, MSc* 7 Lluïsa Quevedo, PhD* 8 Genís Cardona, PhD* 9 Estel·la Blanch, BSc Optom* 10 Montserrat Augé, MSc* 11 12 13 14 15 *Research Group of Centre Universitari de la Visió, Optics and Optometry Department, Technical University of Catalonia, Spain 16 17 18 19 Corresponding Author: Genís Cardona 20 Facultat d’Òptica i Optometria de Terrassa 21 Violinista Vellsolà, 37 22 E08222 Terrassa, Catalonia, Spain 23 24 25 E-mail address: gcardona@oo.upc.edu, genis.cardona@gmail.com 26 Phone: +34 93 739 8774 27 28 1 1 ABSTRACT 2 Purpose: It was the main purpose of this study to investigate the influence of the moistening 3 solution on TBUT measurements in an asymptomatic population. 4 Methods: An online survey was employed to determine the compliance of Spanish eye care 5 practitioners with the recommended normalized procedure to administer TBUT. For the 6 purpose of examining the clinical relevance of discrepancies from the recommended 7 procedure, a randomized, double-masked, bilateral study was designed in which a 8 micropipette was used to moisten fluorescein strips with a controlled volume of six different 9 solutions, commonly available in the contact lens office, and TBUT was measured in 58 non-dry 10 eye (OSDI<15) subjects (age from 19 to 32 years). 11 Results: Results from the online survey revealed that 64% of Spanish practitioners frequently 12 use (or have used) different solutions to moisten fluorescein strips during TBUT assessment. 13 Statistically significant differences in TBUT values were found between the various solutions as 14 a whole (χ2=198.384, p<0.001), as well as between all solutions when explored pair-wise (all 15 p<0.001), except for the two saline solutions. 16 Conclusions: The present findings support the relevance of selecting the appropriate solution 17 when conducting TBUT for the evaluation of the tear film. Deviations from the recommended 18 procedure may result in misdiagnosis of dry eye and unnecessary patient referral. 19 20 KEY WORDS 21 22 Dry eye; Moistening solution; Sodium fluorescein; Tear break-up time; Tear film 2 1 INTRODUCTION 2 Tear break-up time (TBUT) remains one of the most commonly employed tests to assess tear 3 film stability and for dry eye diagnosis [1, 2]. First introduced by Norn in 1969, TBUT was 4 defined as the time “interval between the last complete blink and the presentation of the first 5 appearance of a dry spot or disruption in the tear film” [2, 3]. While many variations exist, the 6 usual technique requires the instillation of sodium fluorescein into the tear film, whereupon 7 the ocular surface is observed with a slit-lamp and a combination of excitatory cobalt blue light 8 and a Wratten #12 yellow observation filter [4]. TBUT values may be influenced by the 9 amount, concentration, pH, presence of preservatives and type of fluorescein, among other 10 factors [5, 6]. 11 Several attempts at controlling the volume of instilled fluorescein have been explored. Indeed, 12 pipetting 1 µl of 2% fluorescein solution was found to result in an improved repeatability of 13 TBUT measurements [7], although there remains debate regarding the increased risk of 14 microbial contamination associated with unpreserved fluorescein solutions and the need for 15 contact of the pipette with the ocular surface [8]. Similarly, the Dry Eye Test (DET; Amcon 16 Laboratories, Inc., USA) was developed to deliver the same small volume of fluorescein 17 solution by application of slightly modified impregnated strips to the superior temporal bulbar 18 conjunctiva [1]. More recently, a Modified Fluorescein Strip (MFS) test was described in which 19 the top 1 mm of a standard fluorescein strip is folded to ensure optimal volume of instilled 20 solution and improve repeatability [9]. 21 It may also be noted that the method of instilling fluorescein solution may affect the cutoff 22 values and the predictive value of the test in the diagnosis of dry eye. Thus, while a cutoff of ≤ 23 10 seconds is generally accepted with standard fluorescein impregnated strips [2, 10], a ≤ 5 24 seconds cutoff was proposed when microquantities of fluorescein are instilled [11]. Similarly, 25 whereas sensitivity and specificity values of 72% and 62%, respectively, are associated with a 3 1 10 seconds cutoff point [10], other authors describe a sensitivity of 94%, as compared with 2 OSDI scores, when the MFS test was employed with a cutoff value of 5 seconds [9]. 3 The standards published by The Diagnostic Methodology Subcommittee of the International 4 Dry Eye WorkShop recommend TBUT to be performed with fluorescein impregnated strips 5 moistened with a single drop of 0.9% nonpreserved saline [12]. However, it is not exceptional 6 for practitioners to employ alternative solutions to moisten fluorescein strips, such as artificial 7 tears [13], or to instil diagnostic drops containing a mix of fluorescein and oxybuprocaine 8 (Fluotest®, Alcon, Spain) [14]. It may be speculated that other solutions commonly available in 9 the contact lens fitting room, such as multipurpose solutions, may be used by practitioners 10 instead of non-preserved saline for the purpose of moistening fluorescein strips during tear 11 film assessment. 12 It was the first aim of the present study to assess, through an online survey, the compliance of 13 Spanish eye care practitioners with the recommended normalized procedure to administer 14 TBUT. Once the survey responses were analysed and it was determined that practitioners 15 employ a variety of solutions for TBUT measurements, a study was designed to determine the 16 influence of the moistening solution on TBUT measurements. For this purpose, TBUT was 17 measured on a sample of non-symptomatic subjects (OSDI score < 15) by moistening 18 conventional fluorescein strips with a constant, controlled volume of six different solutions, 19 commonly available in any contact lens office. 4 1 SURVEY DESIGN AND RESULTS 2 A simple, user-friendly, anonymous online survey was developed, which could be completed in 3 less than 1 minute (see Figure 1). The survey form consisted of 2 questions in which 4 practitioners were first instructed to report on the type of solution they used to moisten 5 fluorescein strips by selecting one or several of the 5 different main solution categories they 6 were provided with, and then they were asked a simple dichotomous question devised to 7 determine whether they employed any means to control the volume of fluorescein instilled in 8 the tear film of their patients. A link to the survey site was sent by email to one hundred 9 registered optometrists randomly selected from the distribution list of the Faculty of Optics 10 and Optometry of Terrassa (Spain). 11 A total of 47 registered optometrists answered the web-based survey. Of all respondents, 64% 12 admitted using, or having used, one or several different solutions, apart from saline solution, 13 to moisten fluorescein strips during tear film assessment (multi-purpose solution, 26%; 14 artificial tears, 23%; wetting solution, 16%; others, 8%). In addition, 77% of the respondents 15 reported not employing any means to control de volume of fluorescein they instilled to the 16 ocular surface during TBUT. 5 1 METHODS 2 Participants 3 Fifty eight students of optometry (45 female) were enrolled on the second part of study. Mean 4 ± SD age of participants was 21.74 ± 2.64 years (range from 19 to 32 years). All subjects had 5 good ocular health and were free of symptoms of dry eye, as evaluated with the Ocular 6 Surface Disease Index questionnaire (OSDI score < 15 [15]). Exclusion criteria were history of 7 ocular or corneal surgery or injury, current use of any ocular medication, ointment or artificial 8 tear substitutes and current or recent contact lens wear. In addition, pregnancy, diabetes and 9 any other systemic condition or use of medication known to influence tear film stability also 10 resulted in exclusion from the study. 11 All participants provided written informed consent after the nature of the study was explained 12 to them. The study was conducted in accordance with the Declaration of Helsinki tenets of 13 1975 (as revised in Tokyo in 2004) and received the approval of an Institutional Review Board 14 (Universitat Politècnica de Catalunya). 15 16 Moistening solutions 17 Six different solutions were employed for the purpose of moistening conventional 1 mg 18 fluorescein sodium sterile strips (Fluorets®, Chauvin Pharmaceuticals Ltd, Surrey, UK). 19 Solutions were selected from those commonly encountered in any optometric practice and 20 represent a sample of the types of solutions listed in the survey, including several with added 21 viscosity agents. A summary of the characteristics of the solutions employed in the study may 22 be found in Table 1. 23 6 1 Procedure 2 A randomized, double-masked, bilateral study was implemented to determine TBUT values 3 with each solution. All sessions took place at the same time of the day and consecutive 4 sessions were 1 to 3 days apart, with a minimum wash-out period of 24 hours between 5 sessions. The same experienced examiner conducted all clinical procedures, and solutions 6 were tested in a random order, under controlled and constant room temperature (20 °C ± 2 °C) 7 and humidity (40% ± 10%) conditions. TBUT was captured via video recording and an 8 independent observer, masked to the type of solution under evaluation, later determined the 9 time interval between the last complete blink and the first appearance of a dry spot. 10 For each solution, a micropipette was used to ensure that only 2 µl of solution was applied to 11 the fluorescein strip in order to deliver a controlled, constant volume to the ocular surface. 12 The strip was then lightly applied for 1 second to the superior-temporal bulbar conjunctiva, by 13 raising the upper eyelid while subjects were instructed to look inferior-nasally. Video capture 14 was repeated 3 times, with subjects blinking normally for about 20 seconds between each 15 recording. Both eyes were used for the study and, in each session, the same type of solution 16 was employed in both eyes. Fluorescein was first instilled in one eye, selected at random, and 17 following video capture, the same procedure was repeated in the contralateral eye. 18 TBUT was observed with a Topcon SL-D7 slit-lamp (Topcon España S.A., Barcelona, Spain) with 19 a cobalt blue light filter and a Wratten #12 yellow filter (Kodak, Rochester, NY, US) positioned 20 in front of the observation system. Slit-lamp magnification was set at 10X and a circular beam 21 of 10 mm in diameter was employed to illuminate the ocular surface. A slit-lamp mounted 22 video camera was used to capture TBUT and a frame by frame examination of recordings was 23 later performed by the independent observer. The median of the three measurements was 24 recorded as the TBUT value for that particular subject and solution. In addition, the difference 7 1 in TBUT between the maximum and minimum values for each subject and solution was 2 determined and considered an indicator of TBUT consistency. 3 4 Data analysis 5 Statistical analysis of the data was performed with the SPSS software 19.0 (IBM Corp., NY, US) 6 for Windows. Descriptive statistics were employed to summarize the answers to the online 7 survey. For TBUT and TBUT consistency values, data from right and left eyes was found to 8 present a strong positive correlation (Spearman rho = 0.92; p < 0.001). Besides, when 9 submitted to a Wilcoxon test for matched pairs, no statistically significant differences were 10 encountered between both eyes in either TBUT or consistency values between both eyes for 11 any of the solutions under study (all p > 0.05). Thus, data from only one eye (selected at 12 random) was used for statistical analysis. TBUT values were examined for normality with the 13 Kolmogorov-Smirnov test, revealing a non-Gaussian distribution of the data (in agreement 14 with published literature [4]). Therefore, all results are provided as median values. The 15 Friedman test was employed to analyse the significance of TBUT score differences between 16 solutions, whereupon the Wilcoxon test for related samples was used as a post-hoc test to 17 investigate pair-wise differences between solutions. A p-value of 0.05 or less was considered 18 to denote statistical significance throughout the study. 8 1 RESULTS 2 A summary of TBUT values for each of the moistening solutions is presented in Table 2. 3 Analysis with the Friedman test revealed a statistically significant difference in TBUT scores 4 between the six different solutions (χ2 = 198.384; p < 0.001) which, when submitted to a post- 5 hoc pair-wise analysis with the Wilcoxon test, disclosed statistically significant differences in 6 TBUT values between all pairs of solutions (all p < 0.001), with the exception of between S1 7 and S2 (Z = -0.875; p = 0.381). Solutions S3 and S2 were found to present the smallest (1.22 8 seconds) and largest (1.84 seconds) median differences between the maximum and minimum 9 TBUT measurements (TBUT consistency values), respectively. For comparison purposes, Table 10 2 also shows the number of patients with TBUT values under the cutoff of 5 seconds 11 recommended for small volumes of instilled fluorescein. 9 1 DISCUSSION 2 The results from the survey underline the fact that, even with the existence of published 3 protocols aiming at normalizing such common optometric procedures as TBUT assessment, 4 there is a lack of uniformity when performing this test. Indeed, although previous surveys of 5 the clinical practices of both Spanish and Australian optometrists revealed TBUT to be one of 6 the most commonly employed tests for tear film evaluation and dry eye diagnosis, the same 7 surveys disclosed a lack of agreement between the published recommendations and actual 8 clinical practice [16,17]. These studies, however, did not investigate in detail how optometrists 9 conducted each particular test. 10 Although many authors have acknowledged the influence of volume of instilled fluorescein on 11 TBUT values [1,5,7,9], and also noted the lack of consensus regarding what should be 12 considered a standard procedure to control this volume [1,5,18], to the best of our knowledge 13 no previous research had evaluated the influence of employing alternative solutions to 14 moisten fluorescein strips on TBUT measurements. Therefore, given that the online survey 15 revealed that many practitioners use different solutions for TBUT evaluation, it is important to 16 understand these effects. 17 Overall, TBUT values were comparable to those reported in the literature for non-dry eye 18 subjects and small volumes of instilled fluorescein [11], and were not inconsistent with those 19 documented by other authors when using conventional or modified strips [1]. The small 20 differences between the maximum and minimum TBUT measurements, defined as good TBUT 21 consistency, were also in agreement with previous reports in which small volumes of 22 fluorescein were instilled with modified fluorescein strips [1,9] or by pipetting 1 µl of 2% 23 fluorescein solution [7], but conflicted with other studies in which volume of fluorescein was 24 not found to influence measurement variability [5]. 10 1 Statistically significant differences were uncovered upon comparing TBUT values with different 2 solutions. These findings may potentially be explained by the biophysical properties of each 3 particular solution such as different solution viscosity from the addition of viscosity agents. 4 Thus, for example, S1 and S2 are both saline solutions with similar TBUT values and TBUT 5 consistency, although S2 may be argued to be closer to the ideal recommendation for TBUT 6 evaluation (nonpreserved saline). On the other hand S3, which resulted in the longest TBUT 7 values, contains hyaluronic acid, which has been reported as a high-viscosity agent equivalent 8 to mucus glycoprotein, with the ability to adhere to epithelial cells [19]. Previous research on 9 surface residence time found that solutions containing sodium hyaluronate had a mean half- 10 life on the ocular surface of 321 seconds, significantly longer than others with hydroxypropyl 11 methyl cellulose, which is a viscosity agent for S4, or a buffered saline solution such as S1 and 12 S2 [20,21]. Other reports also disclosed that tear substitutes with sodium hyaluronate provide 13 better tear film stability, as determined by NIBUT values, than those with hydroxypropyl 14 methyl cellulose [22], and also resulted in better patient reported comfort [23]. In addition, in 15 the present study solutions with high or mid-viscosity agents also led to less variation between 16 the maximum and minimum TBUT measurements, that is, in better TBUT consistency, which 17 may also be a reflection of solution properties. 18 These findings, however, may be interpreted with caution. In effect, S6, which contains 19 hyaluronan, was found to result in the shortest TBUT, and the second worst consistency of all 20 solutions. Thus, it may be speculated that different concentrations of HA, as well as different 21 combinations of HA with other solution constituents, may lead to a different overall effect on 22 the tear film, which may be difficult to infer by the inspection of the composition of a 23 particular solution alone. 24 It must be noted, however, that albeit statistically significant differences were found, absolute 25 TBUT values differences were probably devoid of clinical significance (if defined as a change of 11 1 30% or more [5]). Besides, further research, with a sample of both dry eye and non-dry eye 2 patients, is required to investigate the influence of solution on the sensitivity and specificity of 3 TBUT measurements with the various solutions. In addition, it needs to be noted that although 4 all subjects were considered as normal based on an OSDI score < 15, some patients presented 5 TBUT values with S2 (the recommended solution) lower than the cutoff value of 5 seconds. 6 This finding, which is not unexpected, given the documented discrepancy between signs and 7 symptoms [24], raises the question of whether different results would have been obtained 8 with a study sample resulting from a different set of inclusion criteria (e.g. based on clinical 9 signs instead of symptoms). It was believed, however, that although absolute TBUT scores 10 would probably differ, the main goal of the study, which was to explore the effect of solution 11 selection TBUT values, should still be valid. 12 Finally, it is worth observing that in the present study a constant volume of solution was 13 employed. However, the findings from the online survey revealed that many practitioners do 14 not adhere to any protocol to control the amount of instilled fluorescein. In addition, it is 15 known that the size of a drop will depend on such properties of the solution as viscosity and 16 surface tension, that is, solution composition and drop size are interrelated variables. In 17 consequence, it may be relevant to explore the joint contribution of volume and solution 18 composition on TBUT values. 19 In conclusion, the present findings support the relevance of selecting the appropriate solution 20 when conducting TBUT for the evaluation of the tear film. Deviations from the recommended 21 procedure may result in misdiagnosis of dry eye and unnecessary referral of patients, with the 22 associate economic implications. In addition, communication and continuous education and 23 training efforts are required to encourage practitioners to revise and adhere to the published 24 recommendations for tear film evaluation. 12 1 REFERENCES 2 1. Korb DR, Greiner JV, Herman J. Comparison of fluorescein break-up time measurement 3 reproducibility using standard fluorescein strips versus the dry eye test (DET) method. 4 Cornea 2001; 20: 811-5. 5 6 7 8 9 10 11 12 13 14 2. Lemp MA. Report of the National Eye Institute/Industry Workshop on Clinical Trials in Dry Eye. CLAO J 1995; 21: 221-32. 3. Lemp MA, Dohlman CH, Holly FJ. Corneal desiccation despite normal tear volume. Ann Ophthalmol 1970; 2: 258-61. 4. Cho P, Douthwaite W. The relation between invasive and noninvasive tear break-up time. Optom Vis Sci 1995; 72: 17-22. 5. Johnson ME, Murphy PJ. The effect of instilled fluorescein solution volume on the values and repeatability of TBUT measurements. Cornea 2005; 24: 811-7. 6. Mengher LS, Bron AJ, Tonge SR, Gilbert DJ. Effect of fluorescein instillation on the precorneal tear film stability. Curr Eye Res 1985; 4: 9-12. 15 7. Marquardt R, Stodmeister R, Christ T. Modification of tear film break-up time test for 16 increased repeatability. In: Holly FJ, ed. The Precorneal Tear Film in Health, Disease, 17 and Contact Lens Wear. Lubbock, TX: Dry Eye Institute, 1986, pp: 57-63. 18 19 20 21 8. Rautenbach P, Wilson A, Gouws P. The reuse of ophthalmic Minims: an unacceptable cross-infection risk? Eye (Lond) 2010; 24: 50-2. 9. Pult H, Riede-Pult BH. A new modified fluorescein strip: Its repeatability and usefulness in tear film break-up time analysis. Cont Lens Anterior Eye 2012; 35: 35-8. 22 10. Vitali C, Moutsopoulos HM, Bombardieri S. The European Community Study Group on 23 diagnostic criteria for Sjögren’s syndrome. Sensitivity and specificity of tests for ocular 24 and oral involvement in Sjögren’s syndrome. Ann Rheum Dis 1994; 53: 637-47. 25 26 11. Abelson M, Ousler G, Nally L. Alternate reference values for tear film break-up time in normal and dry eye populations. Adv Exp Med Biol 2002; 506 (Part B): 1121-5. 27 12. The Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop. 28 Methodologies to diagnose and monitor dry eye disease. Ocul Surf 2007; 5: 108-52. 29 13. Duran P, León A, Márquez M, Veloza C. Evaluación de la película lagrimal con métodos 30 diagnósticos invasivos vs método de diagnóstico no invasivo. Investigaciones Andina 31 2006; 8: 36-49. 32 14. Vico E, Quereda A, Benítez-del-Castillo JM, Fernández C, García-Sánchez J. A 33 comparative study of 0.15% sodium hyaluronate versus polyvinyl alcohol in the 34 treatment of dry eyes. Arch Soc Esp Oftalmol 2005; 80: 387-94. 13 1 2 3 4 5 6 15. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol 2000; 118: 615-21. 16. Cardona G, Serés C, Quevedo L, Augé M. Knowledge and use of tear film evaluation tests by Spanish practitioners. Optom Vis Sci 2011; 88: 1106-11. 17. Downie LE, Keller PR, Vingrys AJ. An evidence-based analysis of Australian optometrists’ dry eye practices. Optom Vis Sci 2013; 90: 1385-95. 7 18. Tomlinson A, Bron AJ, Korb DR, Amano S, Paugh JR, Pearce EI, Yee R, Yokoi N, Arita R, 8 Dogru M. The International Workshop on Meibomian gland dysfunction: report of the 9 diagnosis subcommittee. Invest Ophthalmol Vis Sci 2011; 52: 2006-49. 10 19. Mengher LS, Pandher KS, Bron AJ, Davey CC. Effect of sodium hyaluronate (0.1%) on 11 break-up time (NIBUT) in patients with dry eyes. Br J Ophthalmol 1986; 70: 442-7. 12 20. Snibson GR, Greaves JL, Soper ND, Tiffany JM, Wilson CG, Bron AJ. Ocular surface 13 residence times of artificial tear solutions. Cornea 1992; 11: 288-93. 14 21. Snibson GR, Greaves JL, Soper ND, Prydal JI, Wilson CG, Bron AJ. Precorneal residence 15 times of sodium hyaluronate solutions studied by quantitative gamma scintigraphy. 16 Eye (Lond) 1990; 4: 594-602. 17 22. Prabhasawat P, Tesavibul N, Kasetsuwan N. Performance profile of sodium 18 hyaluronate in patients with lipid tear deficiency: randomised, double-blind, 19 controlled, exploratory study. Br J Ophthalmol 2007; 91: 47-50. 20 21 22 23 23. White CJ, Thomas CR, Byrne ME. Bringing comfort to the masses: a novel evaluation of comfort agent solution properties. Cont Lens Anterior Eye 2014; 37: 81-91. 24. Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea 2004; 23: 762-770. 14 1 TABLES 2 3 Table 1: Summary of the characteristics of the moistening solutions employed in the study 4 Commercial Name Manufacturer Main Type Preserved Composition Sensitive Eyes® Plus Saline Bausch & Lomb, Rochester, NY, US Isotonic, buffered saline solution Boric acid, sodium borate, potassium chloride and sodium chloride Solución Fisiológica Cinfa 5 ml uni-dose drops Acuaiss 0.35 ml uni-dose eye drops Laboratorios Cinfa, S.A., Huarte, Spain DISOP SA, Alcobendas, Spain Sterile, buffered saline solution Wetting drops Polyaminopropyl biguanide (0.00003%) and disodium edetate (0.025%) Non-preserved Multi-dose 15 ml Sensitive EyesTM Lens Lubricant Bausch & Lomb, Rochester, NY, US Opti-Free® Express® multipurpose solution Alcon Laboratories, Inc., Fort Worth, TX, US Isotonic and buffered solution Aqueous, sterile, isotonic and buffered solution BiotrueTM multi-purpose solution Bausch & Lomb, Rochester, NY, US Aqueous, sterile, buffered and isotonic solution Non-preserved Non-preserved Polyquaternium-1 (0.001%) and myristamidopropyl dimethylamine (0.0005%) Polyaminopropyl biguanide (0.00013%) and polyquaternium (0.0001%) Sodium chloride (0.9%), boric acid, borax and purified water Hyaluronic acid, hidroxyethyl cellulose, sodium chloride, sodium tetraborate, boric acid and 0.02% disodium edetate Boric acid, sodium borate, sodium chloride, poloxamine, hidroxypropyl methyl cellulose, sorbic acid (0.25%) and disodium edetate (0.1%) Citrate, sodium chloride, boric acid, sorbitol, aminomethylpropanol, poloxamine and edetate disodium Hyaluronan, sulfobetaine, poloxamine, boric acid, sodium borate, edetate disodium and sodium chloride 5 15 1 Table 2: TBUT values (in median and interquartile range) for the six different employed 2 moistening solutions. Median TBUT consistency was determined as the difference between the 3 maximum and minimum measurement for each particular subject and solution. 4 SOLUTION CODE Median (seconds) Interquartile range (seconds) S1 S2 S3 S4 S5 S6 6.0 6.0 6.8 6.2 5.7 5.5 1.5 1.6 1.5 1.6 1.3 1.2 Friedman test χ2 = 198.384 p < 0.001 Wilcoxon test All pair-wise differences p < 0.001 except for the difference between S1 and S2 (p = 0.381) Median TBUT consistency (seconds) 1.6 1.8 1.2 1.3 1.7 1.7 Number of patients with TBUT Values under 5 s 6 6 0 2 8 8 5 6 7 8 S1: Sensitive Eyes® Plus Saline; S2: Solución Fisiológica Cinfa 5 ml uni-dose drops; S3: Acuaiss 0.35 ml uni-dose eye drops; S4: Multi-dose 15 ml Sensitive EyesTM Lens Lubricant; S5: Opti-Free® Express® multi-purpose solution; S6: BiotrueTM multi-purpose solution. 16 1 FIGURES 2 3 Figure 1: Web-based survey sent to 100 Spanish registered optometrists to assess habits while 4 conducting TBUT 5 6 17