May 2014 training slides
advertisement

Health Impact Assessment
Training
Kristin Raab, MLA, PHA
MN Climate & Health Program Director
Brenda Hoppe, PhD
MN Climate & Health Program Epidemiologist
May 20, 2014
2
Outline
What is HIA?
Definitions, background, steps
How has HIA been used to improve health?
Healthy Corridors for All HIA (St. Paul)
HB 2800: Oregon Farm to School and School Garden
Policy HIA
Above the Falls HIA (Mpls)
How do I determine if I should do an HIA?
First HIA step: screening
What is health?
Health is a state of
complete physical, mental
and social well-being and
not merely the absence of
disease or infirmity.
Source: World Health Organization
This definition has not been amended since
1948
4
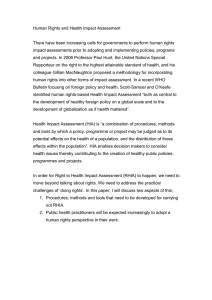
Current Health Conditions in the US
2000 Avg Life Expectancy and Healthcare Spending
US ranked
51st in life
expectancy
for 2012
https://www.cia.gov/l
ibrary/publications/th
e-worldfactbook/rankorder/2
102rank.html
http://ucatlas.ucsc.edu/spend.php
5
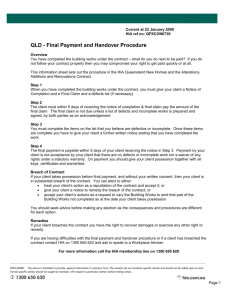
Health Determinants
Health status is determined by: 30% by genetics; only 10% by
health care; but 60% by social & environmental conditions,
and behavior
Source: N Engl J Med 2007;357:1221-8.
6
What do Minnesotans die from?
Leading causes of death in Minnesota: 2010
Cause
Deaths
1. Cancer
9,599
2. Heart Disease
7,144
3. Unintentional Injury
2,087
4. Stroke
2,154
5. Chronic Lower Respiratory Disease 2,012
Rate
166.9
118.7
36.4
35.8
35.1
7
Health Impact Assessment (HIA)
A systematic process that uses an array of
data sources and analytic methods and
considers input from stakeholders to
determine the potential effects of a
proposed policy, plan, program, or project
on the health of a population and the
distribution of those effects within the
population. HIA provides
recommendations on monitoring and
managing those effects.
National Research Council, Improving
Health in the United States: The Role
of Health Impact Assessment, 2011.
8
Values of Health Impact Assessment
HIA aims to advance the
values of
democracy
equity
sustainable development
the ethical use of evidence
a comprehensive approach
Source: http://www.policylink.org/atf/cf/%7B97c6d565-bb43-406da6d5-eca3bbf35af0%7D/PROMOTINGEQUITYHIA_FINAL.PDF
to health
North American HIA Practice Standards Working Group (Bhatia R,
Branscomb J, Farhang L, Lee M, Orenstein M, Richardson M). Minimum
Elements and Practice Standards for Health Impact Assessment, Version 2.
North American HIA Practice Standards Working Group. Oakland, CA:
November 2010.
9
Why Conduct an HIA?
Identify harms and benefits before decisions are made
Identify evidence-based strategies and recommendations to
promote health and prevent disease
Support inclusive and democratic decision-making and
increase transparency in the decision-making process
Support community engagement in the decision-making
process and foster community empowerment
Advance equity and justice
Note: There are many ways to insert health into decision-making. HIA is one way.
10
Types of Decisions Influenced by HIA
•
Policy Decisions (bills by state legislature, city council
decision, local school board on district-wide policy)
•
Policy Implementation (weigh various implementation
options for a policy once it is passed)
•
Project Specific (siting, permitting, construction, design)
•
Comprehensive Plans (neighborhood plan, regional growth
plans, master planning documents)
Provided by Health Impact Project
http://www.healthimpactproject.org/
11
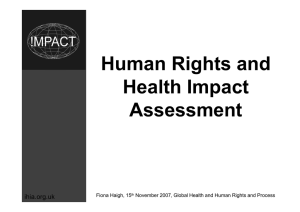
What topics have HIAs addressed?
Provided by Health Impact Project
http://www.healthimpactproject.org/
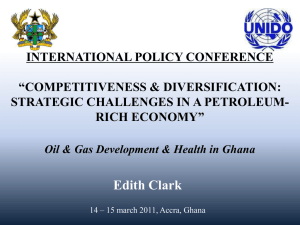
Completed and in progress HIAs
Provided by Health Impact Project & CDC
http://www.healthimpactproject.org/hia/us
13
HIA at the National Level
Two major national funders
Centers for Disease Control & Prevention (CDC) (directly funds
grantees and professional organizations)
Health Impact Project (PEW and RWJF)
SOPHIA (Society of Practitioners of HIA):
http://www.hiasociety.org/
Two conferences:
HIA of the Americas Workshop (Oakland, CA)
National Health Impact Assessment Meeting (WDC)
Local Funder: Blue Cross Blue Shield of MN Foundation
History of HIA in MN
HIAs began with Design for Health
in 2006
MDH began providing technical
assistance, leading or supporting
many HIA-related activities in MN
starting in 2009
Almost all 21 HIAs in MN relate to
the built environment:
comprehensive plans, land use
plans, transportation, except
School Integration Strategies, St.
Paul Emerald Ash Borer, Safe and
Supportive MN Schools Act (not
listed).
New HIAs: Winona Co Active Living
Plan & Lincoln Park SAP
15
MDH’s Role in Promoting HIA
Leading/performing HIAs: (7) Douglas County Comprehensive
Plan; St. Louis Park Comprehensive Plan; Duluth 6th Ave
Redesign Plan; Divine Mercy HIA; Gary/New Duluth Small Area
Plan HIA; Winona County Active Living Plan HIA; Lincoln Park
Small Area Plan HIA
Providing technical assistance: (6) Healthy Corridor for All HIA;
Bottineau Transitway HIA; HIA on the Fort DuPont
Redevelopment Project DE; Second Street Redevelopment Plan
GA; Emerald Ash Borer HIA; MN School Location & Design HIA
Providing HIA training: (10+) (250+ people)
16
MDH’s Role in Promoting HIA (II)
Promoting Health in All
Policies
EAW & Comprehensive
Plans
Tool Development (EAW,
comp planning, brownfields,
climate change)
Sharing information on HIA:
website & listserv (500+)
Promoting HIA through
Collaboration
(http://www.health.state.mn.us/divs/hia/)
17
Collaboration
HIA Interagency Workgroup: (12 agencies)
MN HIA Coalition: (70+ members)
(http://www.health.state.mn.us/divs/hia/coalition.html)
18
HIA Methodology
Six steps
Stakeholder engagement
in all steps
Equity considered
throughout the steps
Scalable
19
Six Steps of HIA
1. Screening - to determine if an HIA is useful for a specific project or
policy
2. Scoping - identify which health effects to consider
3. Assessment - determine which people may be affected and how
they may be affected
4. Recommendations - suggest changes to proposal to promote
positive or mitigate adverse health effects
5. Reporting - present the results to decision-makers
6. Monitoring and evaluating - determine the affect of the HIA on
the decision process
Types of HIAs
Type
Desk Based
Rapid
Intermediate
Comprehensive
Duration
Up to 6 weeks
6-12 weeks
12 weeks – 6 months
6 months – 1 year or
more
Effort
1 full time person
1 full time person
1 full time person,
and supporting help
1 full time person,
and supporting help
Complexity
Provides a broad
overview of potential
health impacts
Provides a more
detailed overview of
potential health
impacts
Provides a thorough
assessment of
potential health
impacts & more
detail on specific
predicted impacts
Provides a
comprehensive
assessment of
potential & predicted
health impacts
Methods
Involves collecting &
analyzing existing
data
Involves collecting &
analyzing existing
data with limited
input from experts &
key stakeholders
Involves collecting &
analyzing existing
data, gathering some
new qualitative data
from stakeholders &
key informants
Involves collecting &
analyzing data from
qualitative &
quantitative sources
LESS COMPLEXITY
MORE COMPLEXITY
Modified from Harris et al. 2007. Health impact assessment: A practical guide, Centre for Health Equity, Training, Research and Evaluation
(CHETRE), Part of the UNSW Research Centre for Primary Health Care and Equity, UNSW:
(http://www.hiaconnect.edu.au/hia_a_practical_guide.htm)
21
Evaluation of HIA
Reviewed 23 HIAs completed in the U.S. between 2005 and 2013
11 HIAs directly contributed to decision outcomes—the way
projects, plans, and policies were developed or implemented
14 HIAs influenced changes beyond the decision under
consideration
16 HIAs showed key stakeholders the health effects of non-health
policies and programs.
17 HIAs built consensus
HIAs amplified community member voices in the decision-making
process
Bourcier, E., Charbonneau, D., Cahill, C., & Dannenberg, A. (2014). Do health impact assessments make a difference? A national
evaluation of HIAs in the United States. Seattle: Center for Community Health and Evaluation.
22
Case Studies
Healthy Corridor For All (MN)
http://sapcc.org/node/600
23
Healthy Corridor for All
1st Comprehensive HIA in MN:
funded by Health Impact Project
Rezoning ordinance
Lead by three organizations:
ISAIAH, Take Action MN,
PolicyLink
Community driven:
The HIA Steering Committee
(20+) was made up of
community leaders and
residents
http://www.policylink.org/atf/cf/{97c6d565-bb43-406d-a6d5eca3bbf35af0}/HEALTHYCORRIDOR_SUMMARY_FINAL_20120111.PDF
24
Community Concerns
Transit-oriented development can be very
beneficial for communities by providing
opportunities for people to live, work, and
play without having to get into a car,
potentially reducing congestion, air
pollution, and increasing access to
opportunity for transit-dependent
households. Yet, as TOD has been
constructed in many cities, it has often
been associated with displacement of lowincome people and communities of color.
This HIA helped support equitable development— ensuring that low-income
households and communities of color benefit from TOD without being
displaced.
25
Scoping
First meetings:
Discussed vision for the
community
Discuss range of possible issues
Voted
3 Areas of Assessment:
1. Healthy Economy
2. Healthy, Affordable Housing
3. Safe and Sustainable
Transportation
26
Key research questions: how will the
proposed zoning…
Healthy Economy
Obj 1: change the amount and quality of jobs that will be available to
residents in the corridor neighborhoods?
Obj 2: affect, small, locally and minority-owned businesses by the corridor?
Affordable, Healthy Housing
Obj 3: affect the likelihood of neighborhood gentrification and the involuntary
displacement of current residents?
Obj 4: impact the cost of housing in the neighborhood and the availability of
affordable housing?
Safe and Sustainable Transportation
Obj 5: coordinate with and affect affordable and accessible public trans?
Obj 6: coordinate with and affect access to safe and connected routs to from
and around rail and bus stops?
27
Housing Pathway
28
Assessment:
Availability of Affordable Housing
Existing Conditions:
14% of total housing units in CC are subsidized affordable units
(80% of Area Median Income or less). 65% of corridor residents
make less than 80% of the AMI
59% of resident spend more than 30% of their income on
housing, compared with 40% St. Paul & 37% Ramsey
68% of renters pay more than 30% of their income in rent
29
Assessment:
Availability of Affordable Housing (II)
Key Impact Assessment Findings:
Market projections suggest nearly 7000 new residential units may
be built in station areas by 2030 of which several hundred may be
affordable if projects use public funding
% of existing subsidized affordable hosing units is likely to
decrease, increasing housing burdens and potentially leading to
involuntary displacement
Rising rents and home values will likely decrease the amount of
affordable housing
If property values near transit stations continue to rise,
acquisition of land for affordable housing near transit will be
more difficult due to higher land costs
30
Recommendations: 5 Policies
Community Equity Program: Pilot program requiring residential
and mixed use projects within ¼ mi of transit stations to make a
% of units affordable or facilitate the production of affordable
housing
Codify Commitment to Affordable Housing: make explicit
statements in the ordinance of the intent to promote diversity
and provide a range of affordable housing
Density Bonus Program: expand incentives in the ordinance to
offer increased density in the form of floor area and height
bonuses and/or modification of parking requirements for
affordable housing
31
Recommendations (II): 5 Policies
Relieving Lack of Commercial Parking: adopt regulations that
would allow use of undeveloped parcels for temporary parking
lots to relieve parking problems during construction
First Source Hiring: all construction contractors notify the St.
Paul Human Rights and Equal Economic Opportunity
Department of available job openings—a referral system shall
identify targeted applications who meet contractor’s
qualifications. Contractor would be required to keep a log of
referrals and applicants hired to monitor the program for
compliance.
32
Monitoring/Evaluation
Increased relationships among SC members who never worked
together in the past
Increased community capacity to understand land use policy and
its impacts on health and equity
Research and data SC leaders can continue to use
City Council: resolution to create affordable housing workgroup
Commissioned a feasibility analyses on a number of affordable
housing recommendations
Shifted policy debate to include more community voices and
introduced health into the discussion
33
Farm to School and School Garden Policy
Bill 2800 (HB 2800), the Farm to
School and School Garden
legislation, as introduced in
January of 2011:
(1) allocate $19.6 million in state funds,
equivalent to 15 cents per lunch and 7
cents per breakfast, to reimburse schools
for purchasing Oregon food products,
and
(2) provide $3 million in competitive
education grants to support food, garden
and agriculture activities, up to 150
school teaching gardens each fiscal year.
Source: Henderson, T., Rader, M., Sorte, B., Ratcliffe, M. M., Lawrence, A., Lucky, J., and Harris, C. (2011) Health Impact Assessment: Farm to
School and School Garden Policy, HB 2800, Upstream Public Health and the Health Impact Project.
http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
34
Screening/Scoping: Health Determinants
1.
Employment
2.
Diet & Nutrition
3.
Farm to School & School
Garden Education
4.
Environmental Health
5.
Social Capital
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
35
Key Research Questions
HB 2800 Farm to School
http://www.healthimpactproject.org/resources/document/Upstream-HIA-Oregon-Farm-to-School-policy.pdf
36
Assessment
Literature review
Secondary data analysis
(food insecurity, school meal
eligibility, school nutrition
services, unemployment)
Economic analysis
Interviews, committee
feedback, community
forums
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
37
Assessment: Employment
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
38
Current Conditions/Assessment
Oregon’s unemployment rate was 10.5% in
December 2010, higher than the national average
of 9% .
The recession hurt Oregon’s farms: almost 2/3 of
farms reported net losses. Small & mid-sized farms
especially are struggling to compete.
Unemployed are up to twice as likely to die earlier
than others of the same age and sex.
The meal reimbursement program would create
jobs and stimulate economic growth.
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
39
Conclusions
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
40
Assessment: Farm to School & School Garden
Education
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
41
Current Conditions/Assessment (II)
Current Oregon learning standards do not require children to learn where
food comes from or how it is made.
Cafeterias are not connected to classroom curriculum.
1 in 4 Oregon adolescents are overweight or obese.
58% of 11th graders eat three or less servings of fruits and vegetables a
day.
Research on F2S & SG programs report that children choose more fruits
and vegetables - leading to potential increases in consumption.
Studies show that children who spend time in the garden learn better, get
physical activity and behave better in the classroom.
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
42
Conclusions (II)
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
43
Recommendations
Amend HB 2800 to specify that schools can only get reimbursed
for foods produced/processed in OR
Food, Agriculture and Garden education grants will be
preferentially given to school districts serving:
a low-income student population
schools with a racially diverse student population
schools in rural or urban areas with limited food access
Support schools developing multiple-component programs,
having at least one element in each of the following categories:
Education, Promotion, Procurement and Community
Involvement
All pictures and text from: http://www.upstreampublichealth.org/sites/default/files/F2SHIA_FINAL.pdf
44
Above the Falls Master Plan
(2000) City of MSP & MPRB adopted
redevelopment plan for Upper Mississippi
Riverfront
Phase out heavy industry, address land use conflicts
Some projects completed, but not to scale
Stakeholders raised concerns over practicalities, costs
(2012) Above the Falls Policy Review and
Implementation Study
45
ATF: Screening
Feasible
Resources (staff, money, info)
Interest
Timely
Fit into timeline for incorporation of Review & Implementation Study
Stakeholders already mobilized
Value
Opportunity to increase awareness of health impacts & disparities
Research unknowns
Highlight common ground & accelerate implementation
46
ATF: Scoping
Identify Alternatives
Many land use alternatives to consider so developed criteria for
selection
4 measurable land use decision alternatives that HIA would
investigate
47
ATF: Scoping (II)
Determine Study Area
Determine Goals
Elevate health considerations
Maximize benefits & mitigate risks
Collect input from diverse stakeholders, esp.
untapped groups
Serve as catalyst for redevelopment efforts
48
ATF: Scoping (III)
Identify pathways
Obesity
Environmental quality (air, noise, water quality)
Mental health
Safety & security
Neighborhood cohesion
Neighborhood livability
Employment
49
ATF: Scoping (IV)
Scoping Results
Research questions
What draws/inhibits residents to RF? Links to health?
Which land uses draw the most residents to RF locally &
regionally? Links to health?
Which land uses could improve/harm health of
residents?
Measurable health indicators
Proposed research methods
50
ATF: Assessment
Literature review
Baseline Health Profile
Analysis of Impacts
51
ATF: Assessment (II)
ATF Research Activities:
Review of literature and previous HIAs
Secondary data analysis of health indicators
Community Input Survey
Resident input from community events and forums
52
ATF: Assessment (III)
53
ATF: Assessment (IV)
Baseline Health Profile
Demographics
Existing land use
Pollution in the area
Evidence & existing conditions related to 4 land use
alternatives:
Park Access + Obesity + Mental Health
Parkland + Environmental Quality
Trails & River Connection + Health
Employment + Health
54
ATF: Recommendations
55
ATF: Recommendations (II)
56
ATF: Monitoring & Evaluation
57
ATF: Monitoring & Evaluation (II)
Internal Evaluation Report
Collected feedback from key stakeholders
Evaluated overall HIA process and various steps
Focus on if goals were achieved
Included Impact Evaluation
58
Screening helps determine if HIA…
… is feasible
sufficient information about the decision?
resources available to conduct the HIA?
… can be done in time
fit within the decision-making time frame?
… would add value to the decision making process
health already being considered?
will decision benefit from an HIA, promote health, influence
positive change?
59
When not to do an HIA
No added value
Chula Vista Plan to Improve Walkability
Plan was already considering health
Health advocates involved in design
Resources better focused elsewhere
No influence on decision
Milwaukee Zoo Interchange Project
Insufficient time to complete HIA for drafts
Stakeholders (DOT) not open to considering health
Source: Wisconsin Department of Health Services, Health Impact Assessment: A Tool to
Increase Health Equity in Decision-Making, Great Lakes Intertribal Council, April 23, 2012
60
Concerns about HIA
Concern
Response
HIA is costly
Not as costly as treatment of health impacts in
the long run
HIA is time-consuming and
will slow decision-making
process
Conducting the HIA early will bring issues to the
front of the decision-making process, potentially
speeding approval processes, and preventing
costly litigation that delays projects
HIA will stop economic
development
The role of HIA is to identify mitigations and
recommendations, not to say “don’t do that”
HIA is not scientific
Role of HIA is to pull together disparate pieces of
the best available evidence to make a broad
statement about impacts
Source: Wisconsin Department of Health Services, Health Impact Assessment: A Tool to
Increase Health Equity in Decision-Making, Great Lakes Intertribal Council, April 23, 2012
61
Getting Started
How to start the screening process:
1. Define the decision
What is being proposed?
What is the timeline for the decision?
Project
Launch
Final
Decision
Draft
Plan
Available
Can the HIA be
ready here?
62
Engaging Stakeholders
2. Decide who will be involved in the
screening process
Identify the stakeholders (i.e.,
residents, business owners, regional
agencies, local organizations, elected
officials)
3. Determine if potential partners are ready to
work on the HIA
Do they have resources available to
conduct an HIA?
63
HIA Screening
4. Evaluate the program, plan, or policy
based on screening criteria (including will the
program have a significant impact on health)
Utilize a Screening Worksheet or a Checklist
There are a number to choose from
Use the one that best meets your needs
64
Screening Criteria
Has a project, plan or policy been proposed?
Is there time to conduct HIA before decision is made?
Will decision affect health?
Would health inequities be impacted? How?
Are impacts likely to be significant in terms of number
of people impacted, severity, immediacy or
permanence?
Is there expertise, evidence and/or research methods
available to analyze health impacts?
65
Screening Criteria (cont.)
Is health already being considered?
Are there clear links between the proposal and
health?
Are decision-makers open to considering HIA
findings?
Do stakeholders have interest, capacity/resources to
participate in the HIA?
66
HIA Screening: Final Task
The Final & Essential Screening Task
1.
Define the decision and its alternatives
2.
Decide who will be involved in the screening process
3.
Determine if potential partners are ready to work on the HIA
4.
Evaluate the project plan, or policy based on screening criteria
5.
Notify stakeholders of your decision
67
Example: Above the Falls Master Plan
Focus area includes or adjacent to diverse
neighborhoods with large health disparities
Land use barriers to accessing the river
Proposal to transition predominantly industrial ->
parks and residential land uses
Health concerns: water, noise and air pollution
Master Plan update – incorporate findings from:
ATF Policy Review & Implementation study
Park Board’s RiverFirst visionary design
HIA recommendations
68
Ex Screening
Example screening
69
ATF Screening
ATF Screening Criteria
the strength of the connection between the land use
alternative and health;
the extent of potential impact (i.e. reach) among the
resident populations;
timing of implementation of the land use alternative
such that it could be informed by the HIA;
stakeholder support for the alternative;
potential health effects on current health status of
priority populations; and
effect on the local economy.
70
More Examples from HIP
Paid Sick Days HIA (national, state, local)
Treatment Instead of Prison HIA (WI)
School Integration Strategies HIA (MN)
Federal Farm Bill HIA (national)
HIA for proposed coal mine at Wishbone Hill (AK)
Lower Duwamish Waterway Superfund Site (WA)
HIA for open burning enforcement in La Crosse county (WI)
71
HIA Reports
Improving Health in the United States: The Role of
Health Impact Assessment
(http://www.nap.edu/catalog.php?record_id=13229)
Minimum Elements and Practice Standards for Health
Impact Assessment
(http://www.humanimpact.org/doc-lib/finish/11/9)
Guidance and Best Practices for Stakeholder
Participation in Health Impact Assessments
(http://www.hiasociety.org/documents/guide-forstakeholder-participation.pdf)
Promoting Equity through the Practice of Health Impact
Assessment:
(http://www.policylink.org/atf/cf/%7B97c6d565-bb43406d-a6d5eca3bbf35af0%7D/PROMOTINGEQUITYHIA_FINAL.PDF)
72
Resources: HIA Websites
MDH HIA webpage
(http://www.health.state.mn.us/divs/hia/)
CDC Healthy Places webpage
(http://www.cdc.gov/healthyplaces/hia.htm)
World Health Organization HIA webpage
(http://www.who.int/hia/en/)
HIA Gateway – Public Health England
(http://www.apho.org.uk/default.aspx?QN=P_HIA)
UCLA – HIA Guide web
(http://www.hiaguide.org/)
Health Impact Project website
(http://www.healthimpactproject.org/)
Design for Health website
(http://www.designforhealth.net/resources/healthi
mpact.html)
Healthy Development Measurement Tool website
(http://www.thehdmt.org/)
Source: http://www.policylink.org/atf/cf/%7B97c6d565bb43-406d-a6d5eca3bbf35af0%7D/PROMOTINGEQUITYHIA_FINAL.P
DF
73
Contact Information
Kristin Raab, MPH, MLA
Director
MN Climate & Health Program
Minnesota Department of Health
651.201.4893
kristin.raab@state.mn.us
Brenda Hoppe, PhD
Senior Epidemiologist
MN Climate & Health Program
Minnesota Department of Health
651.201.4908
Brenda.hoppe@state.mn.us