Bundling Grassroots Services to Battle Neglected Diseases in
advertisement

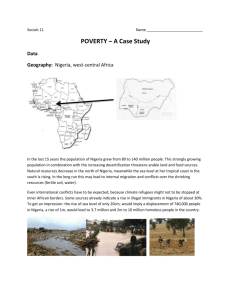
GLOBAL DISEASES: Voices from the Vanguard g Bundling Grassroots Services to Battle Neglected Diseases in Africa A Journey to Nigeria Frank Richards Jr.,, MD The Carter Center March 18, 2008 “Four charismatic scientists invite you to help defeat infectious diseases that thrive in poverty and kill millions of people worldwide.” ld id ” Another (the third) ‘charismatic scientist’ The “P’s” • • • • • • • • • P di t i Pediatrics Parasites (The) Poor Public Health Programs Pills (Tablets) Public Private Partnership Politics President Carter Peace Prize “…I was asked to discuss here in Oslo the greatest challenge that the world faces. Among all the possible choices, I decided that the most serious and universal problem is the growing chasm between the richest and the poorest people on earth….The separation is increasing every year….The results of this disparity are the root causes of most of the problems” world’s unresolved p President Jimmy Carter 2002 Nobel address •‘Diseases of Poverty’ •‘Forgotten ‘F tt Di Diseases off Forgotten F tt People’ P l ’ •‘Neglected Diseases of the Tropics’ An Integrated Community-based MDA Program in Nigeria Structure of my Talk • Introduction p • Public Health Concepts • Three neglected tropical diseases (RB, LF, Schisto) • Nigeria g • Future challenges Structure of my Talk • Introduction • Concepts Control versus Elimination (Eradication) Strategies g Vertical versus Horizontal PH systems • Three tropical diseases (RB, LF, Schisto) • Nigeria • Future challenges Control versus Elimination (Eradication) Strategy Control Elimination li i i TIME Vertical versus Horizontal PH systems Focused Controlled Inputs Outputs Polyvalent P l l t ‘Basket’ Decentralized decisions ‘Sustainable’ Donors Love It! ‘Integration of Programs means Integration g of Problems’ Dr Hans Remme, Dr. Remme WHO/TDR Structure of my Talk • • Introduction Concepts Control versus Elimination (Eradication) Strategy Vertical versus Horizontal PH systems • Three tropical diseases Onchocerciasis River Blindness Lymphatic Filariasis (LF) Schistosomiasis S (‘S (‘Schisto’) ) • • Nigeria Future challenges g Neglected Tropical Diseases Preventive Chemotherapy (Mass Drug Administration-MDA) Pharmaceutical Drug Donation Programs UGA’s Center for Tropical and Emerging Global Diseases (www.ctegd.uga.edu) ( g g ) • • • • • • • Leishmaniasis* Chagas’ Disease* African Trypanosomiasis* S hi t Schistosomiasis* i i * Cryptosporidiosis Lymphatic Filariasis* Malaria *NTDs DALY perspective ((millions)) • • • • • • TB Malaria Treatable NTDs ‘Treatable’ Diarrheal disease HIV--AIDS HIV LRI Hotez et al PLos Medicine 2006 34.7 46.5 56.6 62.0 84.5 84 5 91.3 Control versus Elimination • • • • • Onchocerciasis: Control L Lymphatic h i Fil Filariasis: i i Eli Elimination i i Schistosomiasis: Control Trachoma: Elimination Soil Transmitted Helminths: Control ‘N ‘Nearness to rivers… Can eat the eyes’ African Proverb Geographic Distribution of Onchocerciasis WHO 1999 Microfilaria Intensity (‘load’) of Infection Who suffers from ‘oncho?’ oncho? • • • • • A disease of rural poverty 90 million people at risk 34 million infected 37 countries Some 800,000 people are either blind or visually handicapped • Rarely fatal Clinical Manifestations • Blindness • Visual Vi l Impairment • Skin rashes • Intense itching g WHO/TDR/Ward MIcrofilaria (‘MIcrofilaricide’) MAcrofilaria ( MAcrofilaricide ) (‘MAcrofilaricide’) Treatments approved and shipped by the MectizanR Donation Program 1988 1988-2006 2006 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 70 60 50 40 30 20 10 0 Source: Annual Highlight Mectizan Donation Program www mectizan org Treatments approved and shipped by the MectizanR Donation Program 1988 1988-2006, 2006, with UTG 100 80 60 40 20 06 20 04 20 02 20 00 20 98 19 96 19 94 19 92 19 90 19 19 88 0 Source: Mectizan Donation Progra www.mectizan.org Carter CenterCenter-Assisted Mectizan Distribution Mexico Venezuela Nigeria G t Guatemala l Ethiopia Colombia Ecuador Sudan Cameroon Uganda Brazil Carter Center Center--Assisted Areas Carter CenterCenter-Assisted Programs: Mectizan Treatments 1996 – 2007* 12,200,000 11,054,088 11,109,61110,798,434 12,000,000 9,694,415 8,964,429 10,000,000 8,000,000 6,882,422 8,019,378 7,229,829 6,209,580 6,000,000 5,090,511 3,828,180 4,000,000 2,000,000 0 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 *Provisional November 2007 The Carter Center celebrates Over assisted Ivermectin treatments in 11 Countries in Africa and the Americas since 1996 Thank you to our partners! Cost per Treatment in CarterCarter-assisted African RB Programs Averages $0.50 $ (range $0.10$0.10-1.50) Impact of Eight Years of Mass Ivermectin Treatment in a Cohort of 411 persons in Imo State, Nigeria Nodule Visual Impairment Papular Dermatitis 1995 2002 Leopard Skin 0 Emukah, AJTMH 2004 20 40 60 Cohort Percent Positive Who suffers from ‘LF?’ LF? • A disease of rural and periurban poverty • Over O 1 billion billi people l att risk i k • 120 million infected • 80 countries • Leading cause of disability • Rarely fatal Life Cycle of Lymphatic Filariasis 56 www filariasis org www.filariasis.org Who suffers from ‘Schisto?’ Schisto? • A disease of rural and periurban poverty • Over O 650 million illi people l att risk i k • 200 million infected • 76 countries • Major and subtle morbidity • Rarely fatal Intestinal Schistosomiasis Control versus Elimination • Onchocerciasis: Control • Lymphatic L h i Fil Filariasis: i i Eli Elimination i i • Schistosomiasis: Control Structure of my Talk • Introduction • Concepts Control versus Elimination (Eradication) Strategy Vertical versus Horizontal PH systems • Three tropical diseases (RB, LF, Schisto) • Nigeria • Future challenges Nigeria Carter Nigeria Center assisted GRBP-Assisted GRBP Assisted States States in Nigeria SOKOTO KATSINA YOBE JIGAWA ZAMFARA BORNO KANO KEBBI BAUCHI KADUNA GOMBE NIGER ADAMAWA PLATEAU FCT KWARA NASSARAWA OYO TARABA EKITI KOGI OSUN BENUE Nigeria Integrated Project ONDO OGUN ENUGU LAGOS EDO EBONYI ANAMBRA CROSS RIVER DELTA GRBP alone Km BAYELSA 0 50 IMO GRBP & LCIF Sight i h First i ABIA 100 RIVERS AKWA IBOM State Boundries GLOBAL DISEASES: Voices from the Vanguard g Bundling Grassroots Services to Battle Neglected Diseases in Africa A Journey to Nigeria Frank Richards Jr.,, MD The Carter Center March 18, 2008 Why y ‘Bundling’ g (Integration, ( g , Coimplementation) in Nigeria? • Nigeria has the most River Blindness in the World (27 million in need of treatment) and the best Mectizan treatment program in the World • Most LF (22% of Nigerians infected). 3rd globally (after ( India/Indonesia)) • For Schisto, greatest praziquantel tablet requirement of any country (60 million/yr) • A lot l t off other th diseases di (T (Trachoma, h IIntestinal t ti l Worms, W Malaria) Integrated Onchocerciasis, Lymphatic Fil i i and Filariasis d Urinary Ui Schistosomiasis S hi t i i Activities in Nigeria: AC Case St Study d We integrated three MDA programs at the LGA level by • Building on the RB platform • Mapping the distribution of LF and schisto • Tailoring district level training and logistics based on the results of mapping exercises • Implementing community based annual health education and mass treatment (with ivermectin, albendazole and/or praziquantel) where appropriate, per WHO guidelines • Evaluating impact Platform Programs and Integration Models Plateau/Nasarawa ONCHO Program Map in 1998 Bassa Jos North Jos East Jos South B/Ladi Riyom Kanam Kanke Mangu Pankshin Bokkos Wase Karu Keffi Akwanga Kokona Mikang Wamba Nas/ Eggon Quan Pan Langtang South Lafia Obi Nasarawa Toto Shendam Awe Doma Keana No ONCHO ONCHO (12) Impact on Onchocerciasisin Plateau and Nasarawa States of Nigeria Onchocerciasis Nodule Prevalences in 23 Villages Percent Nodule Prevalenc ce 60% 51.2% 50% 40% 30% 20% 10% 2.9% 0% 1992 1999/2000 Distribution of Lymphatic Filariasis (LF) in Plateau / Nasarawa States Results in Villages Sampled for LF Antigen Testing ( Numbers are % positive Antigenemia) Binchi 22 " Bakin Kgi 8 "Fursum 22 "Babale 22 "Laminga 4 "Ou 7 "Maijuju 21 "Chugw 15 Newo " "Hoss/Mkera 17 17 " Gura "Gindiri 20 14 "Jing 30 " Seri 62"Garam 56 Minzam Kadyis y " 38 57 Umaisha 4 Yerwa 12 " Katakpa 26 " Gwamlar 58 " " ! ! Chika/Kwatas Nlet "Nl t 24 ! 40 ! Chip "Gidan Mudu 35 "Daffo Ang Zaria 8 " !! Gantang 27 0 !! Ag Habu "Mangar 9"Kakuruk/kurra 14 14 Garkawa 19 " "Gbunchu 19 "Plapung 50 !! Gudi "Mai Ganga Kutu " 28 44 54 32 "Gauta "Yashi "Kagbu "Sabon Gida Galei 11 "Garaku 39 48 D k T Tofa f 10 "Doka 9 38 "Burum Burum "Arikiya "Bassa 11 Bong "Magama " 46 8 30 15 "Shmankar "Gamakai "Akunza Jarme 15 !! Gangum 90 22 27 "Apurugh "Tunga 50 15 "Dudduguru "Akwete 26 46 " " Dada 30 " "Nasarawa 5 Dogon Kurmi 32 " Idadu 36 "Kadarko Keana 12 16 " Azara 38 " !! Lamba 9 !! Danyam 37 Takalara 17 " Phases 2000 - 2003 2000 Phase 1 Oncho Endemic " LF Prevalence (Sample) " " ! GLOBAL 2000 Villages: % ICT (2000) WHO Villages: % ICT (2000) LF Pilot Villages: % ELISA ( 1998) 2001 Phase 2 Oncho Endemic 2002 Phase 3 Non-Oncho endemic 2003 Phase 4 Non-Oncho endemic Plateau/Nasarawa LF/ONCHO Programme Map Bassa Jos North Jos East Jos South B/Ladi Riyom Kanam Kanke Mangu Pankshin Bokkos Wase Karu Keffi Akwanga Kokona Mikang Wamba Nas/ Eggon Quan Pan Langtang South Lafia Obi Nasarawa Toto Shendam Awe Doma Keana LF ONLY (18) ONCHO/LF (12) Carter Center Center--assisted Onchocerciasis and Lymphatic Filariasis Treatments, Plateau & Nasarawa States, Nigeria 4,000,000 3,162,642 3,500,000 3,000,000 2,500,000 , , 2,000,000 1,500,000 , , LF is now the ‘Platform Program’ 1,000,000 500,000 , 0 1992 1993 1994 1995 1996 1997 LF & Oncho Endemic Area 1998 1999 2000 Oncho Txs 2001 2002 2003 2004 LF Endemic Areas 2005* UTG LF/Oncho Treatments in Plateau and Nasarawa States, Nigeria, by Year Y 4,000,000 3,500,000 3,000,000 2,500,000 2,000,000 1,500,000 1,000,000 500,000 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 Integration of LF with RB was fast and d ‘easy’ ‘ ’ Top indicator of success for the Nigeria LF Effort as a ‘Demonstration Project’ We will attempt to show that annual treatment with th ivermectin the i ti andd albendazole lb d l combination bi ti can demonstrate, on a large scale, the feasibility of eliminating lymphatic filariasis from Africa. Africa Impact on Onchocerciasis, Schistosomiasis and Lymphatic Filariasis in Plateau and Nasarawa States of Nigeria Average Lymphatic Filariasis ICT Results in Seven Sentinel Villages 50% 45.1% 40% 30% 20% 10.0% 10% Average Lymphatic Filariasis Mosquito Infection Rate (W. bancrofti) in 9 Sentinel Villages 0% 2000 10% 2004 Perrcent Mosquito IInfection Percent ICT tes sts positive 60% 9% 8% 7% 6% 5.2% 5% 4% 3% 2% 1 1% 1.1% 1% 0% 2000 2004 Onchocerciasis and Lymphatic Filariasis Treatments:* Plateau and Nasarawa States; Past and Projected Future through 2014 Oncho control LF transmission interruption 3500000 3000000 2500000 2000000 1500000 1000000 500000 0 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014 LF & Oncho Txs Oncho Txs LF Alone What happened to our platform?? Schistosomiasis >1 million PZQ treatments celebrated l b t d in i 2007 Integration of schisto with LF/RB has been problematic and ‘slow’ Ui Urinary S Schistosomiasis hi t i i Photo credit Emily Staub Hematuria 3+ 2+ 1+ Tr (-) Urine Dipstick Hopkins AJTMH 2002 Intestinal Schistosomiasis April 2007: The first big donation DG M Chan and Merck KGaA (E-Merck) Exec Board member Elmar Schnee announce 200 million o tab tablet, et, 10 0 yea year PZQ Q do donation at o ((20 0 million/year) WHO Nigeria Pledge • 1.5 million PZQ tablets/year for Carter Center assisted programs in Nigeria • Targeted for School aged children • Tablets are now in Port of Lagos Costt off PZQ C Costs of extra TX rounds Cost of Mapping Bull WHO Aug 2006 Na-Bangchang K, Kietinun S, Kumar Pawa K, Hanpitakpong W, Na-Bangchang C and Lazdins J. Assessments of Pharmacokinetic Drug Interactions and Tolerability of Albendazole, Praziquantel and Ivermectin C bi ti Combination. T Trans Royal R l Soc S Trop T Med M d Hyg H 2006 TRIPLE DRUG ADMINISTRATION (TDA) Treating 3 diseases at once in Nigeria Treating three diseases (Schisto, LF and river blindness) with PZQ, albendazole and ivermectin administered at the same time. Eigege, Annals Trop Med Parasit 2008 Costt off PZQ C Costs of extra TX rounds Cost of Mapping Bull WHO Aug 2006 WHO PZQ Q MDA Treatment Guidelines (1993) Prevalence* Treat - Hyper yp >50% Entire Population p Meso 20 20-- 49% School aged children Hypo <20% Infected children only *Prevalence in sample of school aged children NIGERIA CARTER CENTERCENTER-ASSISTED SCHISTO VILLAGE PREVALENCE ASSESSMENT 800 747 700 600 48% 500 400 65% 35% 358 300 233 200 125 100 0 Assessed N=22,402 Need PZQ School Age Mass Tx Plateau/Nasarawa Programme Map Bassa Jos North Jos East Jos South B/Ladi Riyom Kanam * Kanke Mangu Pankshin Bokkos * Karu Keffi Akwanga Kokona Wase Mikang Wamba Nas/ Eggon Quan Pan Shendam Langtang South Lafia ! Obi Nasarawa Toto Awe Doma Keana LF ONLY (13) LF/ONCHO (8) LF/SCHISTO (5) LF/ONCHO/SCHISTO (4) Intestinal Schistosomiasis Missed Treatment Opportunities for Schistosomiasis mansoni in Plateau and Nasarawa States Julie R R. Gutman1,Ayodele Ayodele Fagbemi2, Kal Alphonsus2, Abel Eigege2, Emmanuel S. Miri2, Frank O. Richards3 1Emory University, Atlanta, GA, United States 2The Carter Center, Center Jos, Jos Nigeria 3The Carter Center, Atlanta, GA, United States In press AJTMH (2008) NIGERIA CARTER CENTERCENTER-ASSISTED URINARY SCHISTO VILLAGE PREVALENCE ASSESSMENT 800 747 700 600 48% 500 400 65% 35% 358 300 233 200 125 100 0 Assessed N=22,402 Need PZQ School Age Mass Tx ‘Mesoendemic’ ‘Hyperendemic’ Enrolled Subjects 924 Children 25% have intestinal Schisto Missed opportunities • Of the 50% of communities not needing treatment for Urinary Schisto, over half need treatment for Intestinal Schisto • Overall, 80% of villages need treatment for some form f off Schisto S hi t (urinary ( i and/or d/ iintest) t t) Why then, Why, then are we mapping???? Costt off PZQ C Costs of extra TX rounds Cost of Mapping Bull WHO Aug 2006 New Ideas with New Resources Simplify, Simplify, Simplify Ralph Waldo Emerson What should we do? • Use donation to treat all the school aged population ((approximately pp y 1 million)) in two state area • Use Triple Drug Administration (TDA) • Get it done in a single round • Less focus on mapping results • Forgo community community--wide PZQ treatment for now and evaluate impact in higher prevalence areas Community based treatment SCHISTO TREATMENTS, 1999 – SEPTEMBER 2007 IN PLATEAU, NASARAWA AND DELTA STATES 196,568 200,000 185,644 160,000 , 136,3 316 151,863 180,000 84,165 93,88 5 120 000 120,000 100,000 101 ,908 140,000 TRX 44,830 80 000 80,000 60,000 20,000 8,414 40,000 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 SCHISTO TREATMENTS, 1999 – SEPTEMBER 2007 IN PLATEAU, NASARAWA AND DELTA STATES 1,000,000 900,000 800,000 700,000 600,000 500,000 400,000 300,000 200,000 , 100,000 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 Conclusions • Integrating LF and RB programs at district level was easy • LF took over from RB as the ‘platform program’ due to size • Control vs Elimination strategies. Stopping LF MDA after 55-6 years ( (2008)? )? Do we loose our platform f program? Conclusions • Schistosomiasis integration was difficult, not only because PZQ is not donated, but: Slow and costly LGA level mapping and village illage stratification Delivery of praziquantel separately from ivermectin and albendazole • Going for 1,000,000 PZQ treatments in 2008 Structure of my Talk • • Introduction Concepts Control versus Elimination (Eradication) Strategy Vertical versus Horizontal PH systems • • Three tropical diseases (RB, LF, Schisto) Nigeria • Future challenges GLOBAL DISEASES: Voices from the Vanguard g Bundling Grassroots Services to Battle Neglected Diseases in Africa A Journey to Nigeria Frank Richards Jr.,, MD The Carter Center March 18, 2008 Fostering Partnership MOBILE DISTRIBUTION COMMUNITY DIRECTED TREATMENT (ComDT, CDTI) Community-based Communityvs. vs Facility--based Facility “That’s the difference between government and individuals. i i i Governments don’t care, individuals do.” Mark Twain Key Hypothesis of new BMGF Grants on Integration I Integration i off community i b based d disease di control programs will increase effectiveness and reduce cost cost,, easing the strain on public health systems in African countries. Integration will therefore improve the health off as many people l as possible ibl att a costt that th t can be sustained for as long as necessary. A Nigerian woman and her baby show their insecticideinsecticide-treated bed net. GLOBAL DISEASES: Voices from the Vanguard g Bundling Grassroots Services to Battle Neglected Diseases in Africa A Journey to Nigeria THANKS G Governments t off Plateau/Nasarawa Pl t /N States St t Federal Government of Nigeria (FMOH) University of Jos CDC Emory University The Gates Foundation Merck & Mectizan Donation Programme GlaxoSmithKline (GSK) Izumi Foundation Lions International APOC/WHO/World Bank Reflections for Students “Never Go Back the Way You Came” From: A P F Profile fil off D Dr. B Ben K Kean,”” CUMC Alumni News, 1985 ‘When When a student asks me today about going into tropical medicine, I tell him or her this: Decide what field yyou want to ggo into;; master the specialty; then, when you go into the tropics, you can bring that special knowledge with you…. The basis for eventual success in tropical medicine is temporary restraint of enthusiasm...’ W. Foege: In Search of a National Agenda for International Health Problems AJTMH 1990; 42:293-97 Don’tt be afraid to be a ‘Globalist’ Don Globalist •Be Be an Activist •Be a Practical Scientist Seek Simple Solutions •Seek •Be Confident Be Focused •Be Thanks!