1 PARASITES Intestinal Protozoa
advertisement

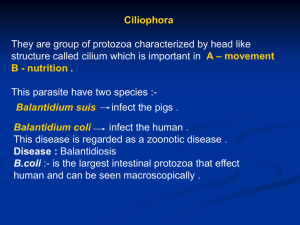
Intestinal Protozoa PARASITES 1 Intestinal Protozoa Intestinal Protozoa Amoeba: Entamoeba histolytica Diseases: Entamoeba histolytica causes amebic dysentery and liver abscess. Important Properties: The life cycle has two stages: the motile (trophozoite) the nonmotile cyst is found within the intestinal and found in nondiarrheal stools. extraintestinal lesions and in diarrheal stools. These cysts are killed by boiling but not by chlorination of water supplies. They are removed by filtration of water. The mature trophozoite has a single The cyst has four nuclei, an important nucleus with lining of peripheral diagnostic criterion chromatin and a central nucleolus (karyosome). 2 Intestinal Protozoa Pathogenesis & Epidemiology: 1. The organism is acquired by ingestion of cysts that are transmitted by the fecal– oral route in contaminated food and water. Anal–oral transmission, e.g., among male homosexuals. 2. The ingested cysts differentiate into trophozoites in the ileum but tend to colonize the cecum and colon. 3.The trophozoites invade the colonic epithelium and secrete enzymes that cause localized necrosis. As the lesion reaches the muscularis layer, a typical "flaskshaped" ulcer forms. 4. Progression into the submucosa leads to invasion of the portal circulation by the trophozoites. By far the most frequent site of systemic disease is the liver, where abscesses containing trophozoites form. Clinical Findings: 1. Acute amebiasis presents as dysentery (i.e., bloody, mucus-containing diarrhea) accompanied by lower abdominal discomfort, flatulence, and tenesmus. 2. Chronic amebiasis: diarrhea, weight loss, and fatigue also occur. Roughly 90% of those infected have asymptomatic infections, but they may be carriers, whose feces contain cysts that can be transmitted to others. In some patients, a granulomatous lesion called an ameboma may form in the cecal or rectosigmoid areas of the colon. These lesions can resemble an adenocarcinoma of the colon. 3. Amebic abscess of the liver is characterized by right-upper-quadrant pain, weight loss, fever, and a tender, enlarged liver. Right-lobe abscesses can penetrate the diaphragm and cause lung disease. 3 Intestinal Protozoa Laboratory Diagnosis: 1. Intestinal amebiasis: finding either trophozoites in diarrheal stools or cysts in formed stools. Diarrheal stools should be examined within 1 hour of collection. Trophozoites contain ingested red blood cells. Because cysts are passed intermittently, at least three specimens should be examined. -E. histolytica can be distinguished by two criteria. (1) The nature of the nucleus of the trophozoite (has a small central nucleolus and fine chromatin granules along the border of the nuclear membrane). (2) The second is cyst size and number of its nuclei. 2. A complete examination for cysts includes a wet mount in saline, an iodine-stained wet mount, and a fixed, trichrome-stained preparation. These preparations are also helpful in distinguishing amebic from bacillary dysentery. 3. Serologic testing ex.indirect hemagglutination test. 4. Detects nucleic acids of the organism in a PCR-based assay. Treatment: 1. The treatment of choice for symptomatic intestinal amebiasis or hepatic abscesses is metronidazole (Flagyl) or tinidazole. 2. Asymptomatic cyst carriers should be treated with iodoquinol or paromomycin. Prevention: 1. avoiding fecal contamination of food and water. 2. good personal hygiene such as hand washing. 3. Purification of water supplies. 4. In areas of endemic infection, vegetables should be cooked. 4 Intestinal Protozoa Flagellates: Giardia lamblia causes giardiasis. Important Properties: The life cycle consists of two stages: the trophozoite the cyst The trophozoite is pear-shaped with two The oval cyst is thick-walled with four nuclei, four pairs of flagella, and a nuclei and several internal fibers. Each suction disk with which it attaches to the cyst gives rise to two trophozoites intestinal wall during excystation in the intestinal tract. 5 Intestinal Protozoa Pathogenesis & Epidemiology: 1.The organism is found worldwide. In addition to being endemic, giardiasis occurs in outbreaks related to contaminated water supplies. Chlorination does not kill the cysts, but filtration removes them. 2.Many species of mammals as well as humans act as the reservoirs. They pass cysts in the stool, which then contaminates water sources. Giardiasis is common in male homosexuals as a result of oral-anal contact. 3.Transmission occurs by ingestion of the cyst in fecally contaminated food and water. 4.Excystation takes place in the duodenum, where the trophozoite attaches to the gut wall but does not invade. The trophozoite causes inflammation leading to malabsorption of protein and fat. Clinical Findings: Watery (nonbloody), foul-smelling diarrhea is accompanied by nausea, anorexia, flatulence, and abdominal cramps persisting for weeks or months. There is no fever. Laboratory Diagnosis: -Finding trophozoites or cysts or both in diarrheal stools. -In formed stools, e.g., in asymptomatic carriers, only cysts are seen. -An ELISA test that detects a Giardia cyst wall antigen in the stool -If microscopic examination of the stool is negative, the string test. Treatment: The treatment of choice is metronidazole (Flagyl) or quinacrine hydrochloride. 6 Intestinal Protozoa Prevention: Prevention involves drinking boiled, filtered, or iodine-treated water in endemic areas. Chilomastix mesnili A non-pathogen - must be differentiated from Giardia. Found in cecum and colon. Transmission occurs by ingestion of mature cysts. Morphology Trophozoite - 4 flagella (3 anterior, 1 associated with the cytostome; one nucleus, always located anteriorly. Cyst - lemon shape; 1 nucleus; cytostome may be seen. 7 Intestinal Protozoa Balantidium coli (ciliates) Balantidium coli, the cause of balantidiasis or balantidial dysentery, is the largest intestinal protozoan of humans. Morphology & Identification: The trophozoite is a ciliated, oval organism. The cell wall is lined with spiral rows of cilia. The cytoplasm surrounds two contractile vacuoles, food particles and vacuoles, and two nuclei—a large, kidney-shaped macronucleus and a much smaller, spherical genetic micronucleus. The macronucleus, contractile vacuoles, and portions of the ciliated cell wall may be visible in the cyst. 8 Intestinal Protozoa Pathogenesis, Pathology, & Clinical Findings: 1.When cysts are ingested by the new host, the cyst walls dissolve and the released trophozoites descend to the colon, and form cysts that pass in the feces. 2.However, rarely, the trophozoites invade the mucosa and submucosa of the large bowel and terminal ileum. As they multiply, abscesses and irregular ulcerations are formed. 3.Chronic recurrent diarrhea, is the most common clinical manifestation, but there may be bloody mucoid stools, tenesmus, and colic. Diagnostic Laboratory Tests: 1.laboratory detection of trophozoites in liquid stools or cysts in formed stools. 2.Sigmoidoscopy may be useful for obtaining material directly from ulcerations for examination. Treatment: A course of oxytetracycline may be followed by iodoquinol or metronidazole if necessary. Epidemiology: -B coli is found in humans throughout the world, particularly in the tropics. - Pig farmers and slaughterhouse workers are particularly at risk, though poor sanitation and crowding in jails, mental institutions are associated with infection. 9

![[Type the document title] Kingdom: Phyla:](http://s2.studylib.net/store/data/012481522_1-94222f0fc30056e395d5b7a2bef31ebc-300x300.png)