The Cost Effectiveness of RSV Prophylaxis: Using Decision
advertisement

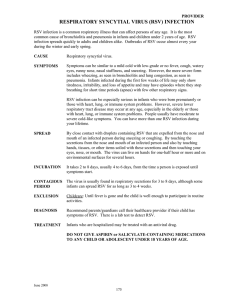
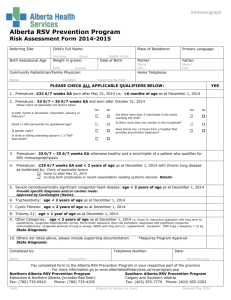
The Cost Effectiveness of RSV Prophylaxis: Using Decision Analysis to Build a Better Guideline Melony E. S. Sorbero, PhD, MS, MPH Purpose • To evaluate the cost effectiveness of current AAP recommendation for use of RSV prophylaxis. • Focus on premature infants without CLD. • Identify more cost-effective alternative recommendations. Sorbero-2 0607 Background • Respiratory syncytial virus (RSV) is the primary cause of lower • • • • • respiratory tract illness in young children. Generally resolves uneventfully in otherwise healthy children. High risk populations may develop severe and sometimes fatal lower respiratory tract infections. RSV infection annually contributes up to 126,300 pediatric hospitalizations in the U.S. Estimated annual hospitalization costs for RSV pneumonia in children <=4 years: $300 - $400 million (1998 $)+. Annual mortality due to RSV in infants and children is estimated to range from 200 ++ to over 2,700 +++. (+Howard et al. J of Peds 2000; ++Shay DK et al. J Infect Dis 2001; +++ Institute of Medicine. In: New Vaccine Development: Establishing Priorities: Vol I. Wash DC Nat Aca Press 1986) Sorbero-3 0607 Background • There may also be long-term health consequences due to severe RSV infections: – Increased risk of asthma and other respiratory conditions – Duration of increased risk up to 10 years • A causal relationship between morbidity and severe RSV infection has not been shown. (Meissner HC at al. Pediatr Infect Dis J. 1999; Sigurs et al. Am J Resp Crit Care Med 2000; Sampalis J Pediatr 2003 ) Sorbero-4 0607 Background • Prematurity increases risk of severe RSV infection. RSV Hospitalization Rate by Gestational Age at Birth 25% 20.60% 20% Percent RSV Hospitalization 14.60% 15% 11.30% 10% 6.40% 5% 0% =< 26 W. 27 - 28 W. > 28 - 30 W. > 30 - 32 W. Gestational Age at Birth (Stevens TP et al. Arch Ped Adoles Med 2000) Sorbero-5 0607 Background • Worldwide RSV epidemics occur yearly – United States: November – April – Peak: January – March (most areas) – Peak: 2 – 3 months earlier (Southeast) • 80% RSV admissions occur within 4 months discharge from NICU. Respiratory Illness Hospitalization Rate by Month of Discharge from NICU in Infants <= 32 Weeks GA 45% 42% 41% 40% 35% 30% 27% Probability of 25% hospitalization 20% 15% 15% 10% 5% 0% Jan. Feb. - Apr. May - Aug. Sept. - Dec. Month of Discharge (Cunningham CK, McMillan JA, Gross SJ Pediatrics 1991) Sorbero-6 0607 Background • No vaccine available for RSV. • 2 products available in U.S. for passive immuno-prophylaxis against RSV. • Respiratory Syncytial virus immunoglobulin intravenous (RSV-IGIV) (RespiGam; MedImmune, Inc, Gaithersburg, MD), containing hightiter RSV antibodies. • Palivizumab, (Synagis; MedImmune, Inc, Gaithersburg, MD), is a humanized monoclonal antibody that binds to the F-protein of RSV. • Require monthly treatments during RSV season. • Synagis less costly and more effective of two. Sorbero-7 0607 American Academy of Pediatrics (AAP) Recommendations for Prophylaxis Use • Released in 1998; updated in 2003. • Infants younger than age 2 years who currently receive or have recently required medical therapy for CLD. • Infant born 28 weeks gestation who are 12 months old at the start of the RSV season. • Infants born at 29 to 32 weeks who are 6 months old at the start of the RSV season. • Infants born between 32 and 35 weeks of gestation with risk factors. (Red Book, 2000) Sorbero-8 0607 Synagis • Efficacy of Synagis in prevention of severe RSV infection in premature infants without CLD: 82%. • Synagis is available in 50 and 100 mg vials. • The cost is $725 per 50 mg and $1370 per 100 mg vial. • Synagis has a shelf life of 6 hours making drug wastage nearly inevitable. Sorbero-9 0607 Study Design • Developed decision analytic model. • Societal perspective. • Two versions: w/ and w/o asthma. • Impact of asthma modeled with semi-Markov processes. • Conducted CEA on models with asthma; CBA on models w/o asthma. • Seven hypothetical cohorts of premature infants without CLD born at 24 – 32 weeks gestational age (GA). • Assumed discharged from NICU at 36 weeks post-conceptual age. Sorbero-10 0607 Model Assumptions • Risk of RSV hospitalization obtained from published literature. – Gestational age specific probabilities – Seasonal pattern of hospitalization • Efficacy of palivizumab adapted from IMpact study. • Costs: year 2002 dollars • Costs include: – Hospital costs – Cost of pulmonary clinic visits for Synagis injections – Emergency room visit cost – Drug costs – Cost of hours missed from work by parents for visits and hospitalization Sorbero-11 0607 Models with Asthma • Increased risk of asthma varies with chronologic age. • Duration for increased asthma risk: 10 years • Includes quality of life adjustment for asthma. • Incorporates national estimates of annual asthma cost • Future benefits and costs discounted at 3% Sorbero-12 0607 Effect of Gestational Age on Expected Costs 9,000 8,000 $ 8,000 Expected Costs ($) 7,000 $ 7,298 6,000 5,000 Synagis: AAP Recommendations: Infants: 29 - 32 weeks if = < 6 months old at the start of the RSV season Synagis: AAP Recommendations: Infants: = < 28 weeks if = < 12 months old at the start of the RSV season 4,000 $ 4,092 3,000 Synagis No Synagis $ 2,184 $ 1,548 2,000 $ 678 1,000 0 24 - 26 27 28 29 - 30 Gestational Age at Birth (Weeks) 31 32 Sorbero-13 0607 Incremental Cost-Effectiveness Ratio • Incremental cost-effectiveness ratio (ICER): Cost1 – Cost2 = QALY1 – QALY2 Cost (Synagis) – Cost (No Synagis) QALY (Synagis) – QALY (No Synagis) • Current suggested “standards” for ICER : – Accepted zone : $200,000 – Not generally accepted zone: > $200,000 / QALY Sorbero-14 0607 Incremental Cost / QALY ($ / QALY) Effect of Gestational Age on ICER 2,000,000 1,800,000 $1,500,351 / QALY 1,600,000 $1,855,000 / QALY With Drug Wastage 1,400,000 1,000,000 800,000 600,000 400,000 $1,481,965 / QALY $ 906,310 / QALY 1,200,000 $1,268,679 / QALY $830,152 / QALY $685,720 / QALY $657,780 / QALY Without Drug Wastage 200,000 Acceptable Zone =< $ 200,000 / QALY 0 24 - 26 27 28 29 - 30 Gestational Age at Birth (Weeks) 31 32 Sorbero-15 0607 Why is the ICER so high? • Substantial difference in costs, even without drug wastage • Very small difference in QALYs: – No proven mortality benefit – No proven long-term quality of life improvement – Change in quality of life due to asthma is small: .03 • Treating many infants at low risk for hospitalization Sorbero-16 0607 $3,500,000 $3,000,000 $2,500,000 $2,000,000 $1,500,000 $1,000,000 $500,000 $0 N ov . . Se pt y Ju l ay M ar . 24-26 weeks 27 weeks 28 weeks 29-30 weeks M Ja n. ICER Large variation within GA in ICER Month of Discharge Sorbero-17 0607 Improving the Recommendation’s Cost Effectiveness • Simulations modifying the AAP guidelines • Assume no drug wastage • Restrict to 1st RSV season • Younger age cutoffs (Discharged Sept. through March) • Restrict to infants born 27 weeks GA or less if discharged before RSV season; up to 30 weeks GA if discharged during RSV season Sorbero-18 0607 ICER by GA and Month of Discharge with new Recommendation $600,000 26 weeks 27 weeks 28 weeks 30 weeks $400,000 $300,000 $200,000 $100,000 $0 Ja n. Fe b. M ar . A pr . M ay Ju ne Ju ly A ug Se . pt . O ct N . ov . D ec . ICER $500,000 Month of Discharge Sorbero-19 0607 ICER by GA with New Recommendation $300,000 $280,083 $250,000 ICER $200,000 $216,830 $150,000 ICER $171,224 $100,000 $103,053 $50,000 $0 26 weeks 27 weeks 28 weeks 29-30 weeks Month of Discharge Sorbero-20 0607 Conclusion • In our model for premature infants without CLD, incremental Cost / QALY: – Was high for all gestational ages; Many ICER were over $1 million. – Large amount of variation across months. • Simulations identified more cost-effective options. • Pursue strategies to minimize drug wastage. • AAP guidelines could be revisited to make them more cost effective. Sorbero-21 0607 Limitations • Some costs were based on local estimates. • May have underestimated cost from family members missing work due to infant hospitalized with RSV. • Unclear whether causal relationship between severe RSV infection and asthma and other long-term health consequences; need for additional research. • Decrease in quality of life due to asthma based on adults. Sorbero-22 0607 University of Rochester Collaborators • Department of Pediatrics, Division of Neonatology/Infectious Disease Dr. Nahed El Hassan Dr. Timothy Stevens Dr. Caroline Hall • Department of Community and Preventive Medicine Dr. Andrew Dick Sorbero-23 0607