AB - Risk Assessment Form 2014-2015
advertisement

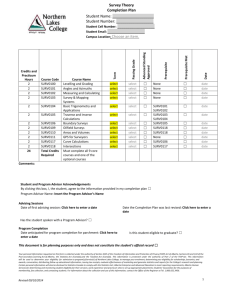
Addressograph Alberta RSV Prevention Program Risk Assessment Form 2014-2015 Referring Site: Child’s Full Name: Surname Birth Gestational Age: Given Date of Birth: Current Community Pediatrician/Family Physician: Name Location Primary Language: Mother: Father: Name: Cell: Name: Cell: Middle Initial Weight in grams: Birth Place of Residence: Home Telephone: Telephone Number PLEASE CHECK ALL APPLICABLE QUALIFIERS BELOW: YES 1. Premature: ≤32 6/7 weeks GA born after May 31, 2014 i.e. <6 months of age as at December 1, 2014 2. Premature: 33 0/7 – 35 6/7 weeks GA and born after October 31, 2014 Please check all applicable risk factors below Yes Is birth month in November, December, January or February? No Yes No Are there more than 5 individuals in the home counting the child? Is there more than one smoker in the household? Small (<10th percentile) for gestational age? Does family live >2 hours from a hospital that provides bronchiolitis treatment? Is gender male? Is child or sibling attending daycare ≥ 3 “half” days/week? 3. Premature: 33 0/7 – 35 6/7 weeks GA otherwise healthy and a twin/triplet of a patient who qualifies for RSV immunoprophylaxis 4. Premature: ≤35 6/7 weeks GA and < 2 years of age as at December 1, 2014 with chronic lung disease as evidenced by: Check all applicable factors home O2 after May 31, 2014 on long term prophylaxis or recent exacerbation needing systemic steroids Details: 5. Severe hemodynamically significant congenital heart disease: age < 2 years of age as at December 1, 2014 Provide specific diagnosis and/or cardiac meds: Approved by Cardiologist (Name): 6. Tracheostomy: age < 2 years of age as at December 1, 2014 7. Cystic Fibrosis: age < 2 years of age as at December 1, 2014 8. Trisomy 21: age < 1 year of age as at December 1, 2014 9. Other Categories: age < 2 years of age as at December 1, 2014 i.e. home O2, meconium aspiration with long term O2 supplements, congenital diaphragmatic hernia, Pierre Robin sequence, stem cell transplant, diagnosed with significant congenital immunodeficiency, congenital anomaly of lung or airway, GERD with long term O 2 supplements, Exception: SMA Type 1 weighing < 15 kg State Diagnosis: 10. Others not listed above, please include supporting documentation State Diagnosis: Completed by: Name *Requires Program Approval Telephone Number: Designation Date: dd-mmm-yyyy Fax completed form to the Alberta RSV Prevention Program in your respective part of the province For more information go to www.albertahealthservices.ca/rsvprogram.asp Northern Alberta RSV Prevention Program Southern Alberta RSV Prevention Program Edmonton & Northern Alberta (includes Red Deer) Calgary and Southern Alberta Fax: (780) 735-6919 Phone: (780) 735-4205 Fax: (403) 955-7779 Phone: (403) 955-2283 Draft Original to remain on chart Revised May 2014