Patient Name: ___________________________________ Date: ________________ Revised Prosthesis Evaluation Questionnaire-Mobility Section
advertisement

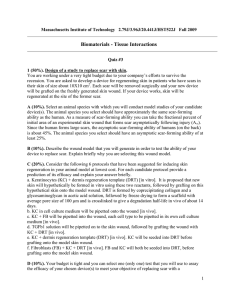
Patient Name: ___________________________________ Date: ________________ Revised Prosthesis Evaluation Questionnaire-Mobility Section Over the past 4 weeks, please rate your ability in the following activities when using your prosthesis (if you don’t have a prosthesis, leave this sheet blank): Unable or hardly able at all (ability <5%) 0 High difficulty (ability 5-34%) (1) Moderate difficulty (ability 35-64%) (2) Little difficulty (ability 65-95%) (3) No problems or almost fully able (ability > 95%) (4) 1. To walk 2. To walk in confined spaces 3. To walk upstairs 4. To walk downstairs 5. To walk up a steep hill 6. To walk down a steep hill 7. To walk on sidewalks and streets 8. To walk on slippery surfaces (i.e. wet tile, snow, rainy street, boat deck) 9. To get in and out of a car 10. To sit down and get up from a chair with a high seat (i.e. dining chair, office chair) 11. To sit down and get up from a low, soft chair (i.e. deep sofa) 12. To sit down and get up from a toilet of regular height (no aids) Total: ______/48 Reference: Franchignoni F, et al. Measuring mobility in people with lower limb amputation: Rasch analysis of the mobility section of the prosthesis evaluation questionnaire. J Rehabil Med. 2007; 39(2):138-44.