fsnn_sbctf_meeting_9_feb_3_2012

Food Security & Nutrition
Network
Social & Behavioral
Change
Task Force
Meeting #9
February 3, 2012
Agenda
1.
Report on TOPS Training / FSN Network Meeting (Jennifer
Peterson, 10 mins)
2.
The FSN Network Website and You (Natalie Neumann, 30 mins)
3.
Review of Underweight Reduction Projects (Sarah Bauler,
20 mins)
4.
Status Reports (15 mins):
• Introductory documents on 5 SBC Tools
• Draft SBC Guidance document (for FFP)
• DBC manual review (and ms-DBC trainings)
5.
SBCTF Work Plan Creation (15 mins)
1. Report on TOPS Training / FSN Network Meeting
• Maputo, September 2011
• Jen Peterson’s report
• June 2011 TOPS Training / FSN Network
Meeting Heads-up
TOPS
T
echnical and
O
perational
P
erformance
S
upport
Program for FFP Grantees
Promoting excellence in food security programming
Food Security and Nutrition Network Training Workshop
Maputo, Mozambique
19 – 23 Septembre 2011
Strengthening the capacity of Title II Implementing Partners
Agenda
• Day 1 & 2 – Technical Discussions: Nutrition, Agriculture, M&E
• Day 3 – Working in consortia, conservation agriculture, food quality issues, agriculture and nutrition integration, WFP household surveys, CARE groups, trigger indicators, Behavior change communications , and PM2A (MCH rations)
• Day 4 – Discussion between donors and NGOs, the influence of grandparents and fathers on the nutrition of young children, value chains and the vulnerable, beneficiary monitoring,
Ag/NRM and Nutrition Behavior Change Communication , food security and gender, CMAM, local purchases for food distribution, Village Savings and Loans (VSL), monitoring the quality of behavior change methods .
• Day 5 – Partner Capacity building, networking and closing.
Working in Consortia
Working in Consortia
Recommendations
• Budgeting resources for technical workshops, field visits and subsequent monitoring, meetings, After
Action Review, tool development, and learning
• Be accountable for information sharing
• Make sure field staff are participating in the « buy-
in »
Best Practices
• Establish common principals
• Use FFP/USAID regulations as a foundation for best practices
• Develop conflict solving mechanisms
• Decentralize with clear and common standards
• Communication protocol and mechanisms
• A good MOU
How to create a Network
1. Establish the rules of the game
2. Define the identity, goal and name for the group
3. Identify leaders for each role and responsibility
4. Identify sources of technical interest and champions
5. Create an action plan
6. Program the next steps and a communication plan.
TOPS Regional
Networks
• Local network (regional) created during this workshop:
– Conservation Agriculture
– Trigger Indicators
– Agriculture – Nutrition/ Health (AGNUTH)
– Capacity building of local partners
• Help us keep them alive!
Dialogue between NGOs and Donors
What NGOs appreciate about FFP:
• Site visits, support
• Flexibility
• Resources and tools, even in the context of financial constraints
• Long term financing (5 years)
• Norms and standards
• Networking opportunities
• Focus on results, accountability and data quality
• Financial standards
• The focus on food security
“Collaboration between donors and NGOs is essential to achieve our objectives” (Rina, LOL participant).
Dialogue between NGOs and Donors
What donors appreciate about NGOs:
• We work in the most difficult areas, with the most vulnerable people
• Expertise, creativity and innovation
• Multidisciplinary
• Advocacy for what counts
• Flexible, responsive to changes
• Involvement of state structures to ensure sustainability
• Local capacity building
• Efficient/cost-effective
• Accountable
• Community mobilization for action
Dialogue between NGOs and Donors
Donor Expectations
• Quality data
• Sharing best practices and
Success Stories
• Participation in Working
Groups
• Consultative, participatory processes
NGO Expectations
• Coordination between donors
• Participation in developing national policies
• Sectoral approaches
« basket funding »
• Respecting Monterey
Principals
• Transparency, communication
Designing for Behavior Change
Using the QIV checklist
• Be positive!
• Provide feedback
• Start with improvements made
• Ask staff to start with an autoevaluation (how do you think you did?)
• Be specific and objective
• Non-verbal Communication
• Opportunity to ask questions at the end
• Links to the training required/the future
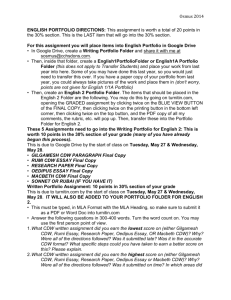
CHECKLIST FOR PRACTICE PROMOTION SESSIONS BY
COMMUNITY DEVELOPMENT WORKERS (CDWs)
Name of CDW:_________________ Evaluator:_______________________
Community: ___________________ Date: __________________________
METHODS YES NO
Setup
1. Did the community development worker (CDW) seat people so that all could see each others' faces? .................................................................................................
2. Did the CDW ask someone if they want to open the session in prayer if appropriate in the local context?..............................................................................
3. Did the CDW wear appropriate clothing? ...............................................................
4. Did the CDW sit at the same level as the other participants? .................................
5. If using a lesson plan : Did the CDW follow the lesson plan in the curricula? .........
Overall Communication
6. Did the CDW speak loud enough that everyone could hear? .................................
7. Did the CDW use proper eye contact with everyone? ............................................
8. Did the CDW use changes in voice intonation (not monotone)? ............................
9. Did the CDW speak slowly and clearly? .................................................................
10. Did the CDW move around the room/area without distracting the group? ..............
11. Did the CDW always use examples/terminology that were culturally appropriate? .
12. Did the CDW encourage comments by nodding, smiling, or other actions that show s/he was listening? ........................................................................................
13. Did the CDW ALWAYS reply to participants in a courteous and diplomatic way? ..
14. Did the CDW prevent domination of the discussion by 1 or 2 people? ...................
15. Did the CDW encourage timid participants to speak/participate? ...........................
16. Did the CDW use a participatory method? (game, skit, song, story, other -- SPECIFY:__________________________) ..............................................
17. Did the CDW ask the participants lots of (non-rhetorical) questions? .....................
18. Did the CDW give participants adequate time to answer questions? .....................
19. Did the CDW encourage discussion amongst participants? ...................................
Beginning
20. Did the CDW introduce the topic well (who s/he is, topic, time)? ...........................
21. Did the CDW ask questions to relate topic to the participants’ experiences? .........
22. Did the CDW ask about the current practices of the participants? .........................
Middle
23. Did the CDW use the brainstorming technique at appropriate moments? ..............
24. Did the CDW use any props? .................................................................................
Design for Behavior Change
• How to monitor the effectiveness of our communications?
– Mini KPC (knowledge, practices coverage survey)
– QIV checklist (to encourager staff, monitoring, improve the quality!)
– Comparison to norms, standards
– Exit polls
– Spot checks
– Pre and post test
« The Behavior
Change sessions were particularly interesting! »
(Faly, LOL)
– Quality Assurance (Partnership defined quality)
Testimonials
“The TOPS workshop allowed me to improve my M&E skills , acquire Community Workers
Evaluation Tools and a better vision of the monitoring process, and a better understanding how to read results and identify factors that influence behavior in a person or group.” (Faly, ADRA)
“Exchanges between the participants from different countries helped me to selfevaluate what I was doing back at home, so I can make improvements if necessary.”
(Rina, LOL)
“I appreciated the way that the training was undertaken, with more than 100 people, with maximum participation , and a rich discussion” (Aime, CARE)
Why should your staff attend TOPS workshops?
• They are fun ! Well organized, interactive, and participatory.
• You learn a lot! The sessions on DBC and M&E were particularly appreciated.
• You are exposed to new ideas and state of the art practices, and have an opportunity to discuss practical implementation issues with other MYAP actors.
• They are integrated ! Gender and communication were treated in each technical session, and links between agriculture and nutrition were constantly identified and reinforced.
• You meet new people and develop important contacts to continue technical discussions and seek advice after the workshop (formal and informal networks).
• It really helped Madagascar staff to think outside the box, get off the island, and innovate . They are more open to new ideas now that they see how other programs are passing them by!
• Your MYAP will be a better MYAP as a result of your participation in TOPS.
2. The FSN Network Website and You
Natalie Neumann, CORE Group
3. Review of Underweight Reduction Projects
Sarah Bauler, Samaritan’s Purse
Review of High Performing Underweight
Reduction Projects:
Determine common SBC strategies and other elements used in high performing CSHGPs
Were there common tools, activities and strategies used in the high performing projects that resulted in these particular projects having more success in lowering underweight than other CSHGP projects?
On behalf of the SBC Task force, thank you to the following SBCTF members who participated in writing up the reviews of the final evaluations of the high performing CSHGPs. They are as follows:
IRC/Rwanda: Adugna Kebede
IEF/Malawi: Diane DeBernardo
CARE/Ethiopia: Tom Davis
WRC/Cambodia: Terry Laura
HAI/East Timor: Paul Freeman
MCDI/Benin: Alison Prather
SAWSO/SA: Phil Moses
Selection criteria used to determine high performing CSHGPs in underweight is as follows:
Cut-off for selection was all projects with both baseline and final underweight data that showed a reduction of underweight of 12 points or more.
Average reduction in stunting in food security projects is about
2 points per year. For this data, the average reduction in underweight was 5.5 points, and the third quartile was 11.4 points.
Projects were selected that were in the top quartile in terms of underweight reduction, 12 points or greater.
Common themes in the reviewers’ overall impression of high performing CSHGPs:
Establishment of volunteer networks and support groups to improve health behaviors
Utilized the Care Group Model to mobilize communities and achieve remarkable behavior change (WR/Cambodia)
Utilized Mother to Mother Support Groups (MTMSG) to target mothers, especially pregnant and lactating mothers, to adopt new behaviors (CARE/Ethiopia)
Utilized an impressive array of volunteer networks (i.e. community members, local leaders, committee members, government officials) to expand coverage and improve health-related behaviors. Also used breastfeeding support groups. (IEF/Malawi)
Health education by community volunteers (IRC/Rwanda)
Volunteer CHWs, also called “front-line health agents”, were trained in adult education and BCC techniques (MCDI/Benin)
Supported/strengthened East Timor’s newly developed community health volunteer program (HAI/East Timor)
Common themes in the reviewers’ overall impression of high performing CSHGPs-cont.
Focused on Key Influencers to promote behavior change
Utilized Ethiopian Church leaders and confessors that transmitted health messages after each church services and performed routine home visits targeted P/L women (CARE/Ethiopia)
Utilized Church Leaders to participate in community assessments, drama performances, developing of the FP film (HAI/East Timor)
MBCC (Male Behavior Change Communication Specialists) were used to reinforce health messages promoted by the WHEs. Also used Health Center staff and Village Leaders to also strengthen the role, respect and value of the WHEs (WR/Cambodia)
Traditional Leaders and DEC Leaders trained on HIV/AIDS were utilized to educate community members (IEF/Malawi)
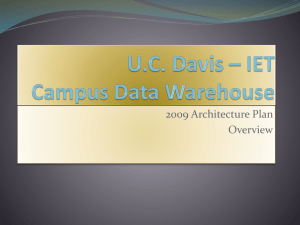
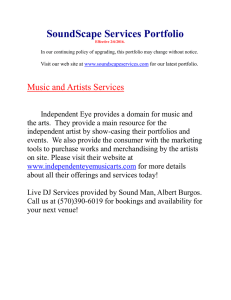
Side note: Review of BA studies that identified
Key Influencers of selected behaviors
Key influencers were organized into following groups: husbands, grandmothers/grandfathers, cousins, mother-in-laws, family members, most people, medical staff, and neighbors/friends
Overall, husbands were more likely to be an important influencer of a maternal behavior (as compared with other groups like grandmothers).
Approval / Disapproval by Different Groups on Selected Behaviors:
Barrier Analysis Studies, Various Organizations
(and Degree of Association)
Common themes in the reviewers’ overall impression of high performing CSHGPs
Strong linkages between project activities and the
MOH to improve health service delivery
Strengthened and supported the health system linkages between the MOH and the community (WR/Cambodia)
Increased available health services by strengthening the links between community and health facilities (IRC/Rwanda)
Strengthened the health system through capacity building, management and logistical support (CARE/Ethiopia)
Partnered with the MOH to build the capacity of their newly developed community mobilization program called SISCa
(HAI/East Timor)
Utilized Health Zone Directors to train Regional Health Center staff to improve quality of care at health facilities (MCDI/Benin)
Common themes in the reviewers’ overall impression of high performing CSHGPs
Utilized Positive Deviants to Promote Behavior change
Use of Model Mothers by the “identification and publicizing” of mothers who exemplified desired CS behaviors (CARE/Ethiopia)
Used the VISA (Visit Identify Sensitize Accompany)
Mother Approach which utilized mothers currently practicing desired behaviors as peer educators for other mothers (MCDI/Benin)
Common themes in the reviewers’ overall impression of high performing CSHGPs
Use of Health Committees/Health Councils
Feedback Committees composed of the CG Leaders and Village Leaders met with MOH staff to provide health updates (WR/Cambodia)
Health Associations consisting of volunteer CHWs and MOH health center staff met monthly
(IRC/Rwanda)
Common SBC Products and tools used in high performing
CSHGPs—not much consensus.
Doer/non-doer analysis (barrier analysis) (MCDI/Benin)
BEHAVE Model (MCDI/Benin, IEF/Malawi)
Positive Deviant studies/PD/Hearth (IEF/Malawi,
CARE/Ethiopia)
Child health cassette recorded messages/radio messages/films (CARE/Ethiopia, IRC/Rawanda, HAI/East
Timor)
Leaflets/posters/counseling cards (CARE/Ethiopia,
IEF/Malawi, HAI/East Timor, WR/Cambodia)
Street drama/puppetry/stories/games (HAI/East Timor,
WR/Cambodia, IEF/Malawi)
4. Status Reports a.
Introductory documents on five key methods
• PDQ: Done … comments?
• Barrier Analysis: Done … comments?
•
Care Groups: Done
… comments?
•
QIVC ( pending )
• To put to a vote soon.
b.
Draft SBC Guidance document (for FFP): Comments? Additional review?
c.
DBC manual review (and Ms-DBC trainings) -- ongoing
Jose Thekkiniath
Sarah Bauler
Elizabeth Arlotti-Parish
- Lauren Erickson (partial)
- Nancy Keith (pending)
- Mary DeCoster (pending, traveling)
* Ms-DBC Training: Niger,
Burundi,
Eth, DC (3/12-17), Uganda
5. SBC TF Workplan Creation
Time permitting, go through format.
Finish filling out in next meeting.
Thanks for your participation !!