Female Genital Cutting
advertisement

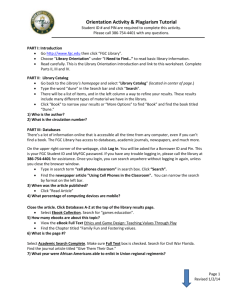
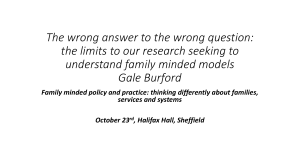
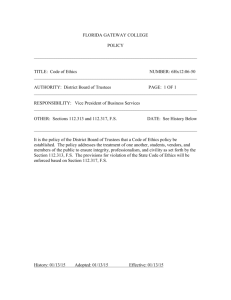
Female Genital Cutting Grand Rounds Presentation April 13, 2012 Erin Black, PGY3 Objectives To understand the historical and cultural significance of female genital cutting (FGC) and its prevalence worldwide To recognize the various types of FGC and their management protocols To develop the skills necessary for delivering appropriate care to circumcised women To understand the legal and ethical issues pertaining to FGC Background Female Genital Cutting (FGC), also known as female circumcision or genital mutilation refers to a number of practices that involve the cutting of a female’s external genitalia. FGC is estimated to have affected over 130 million females worldwide Because of recent immigration patterns, women’s healthcare providers will increasingly encounter patients who have undergone FGC. What is FGC? “All procedures involving partial or total removal of the external female genitalia or other injury to the female genital organs whether for cultural or other non-therapeutic reasons.” World Health Organization. Female Genital Mutilation: a joint WHO/UNICEF/UNFPA statement Geneva: WHO, 1997. What is FGC? FGC is generally performed by a medically untrained person - however, the circumciser will vary from culture to culture. In some cultures, the person performing the act of FGC has limited medical training - midwives, nurses, and some physicians. Many different names have been used to describe FGC - “female circumcision” or “female genital mutilation” It is important to recognize that most women who have undergone FGC, do not recognize themselves to be mutilated Most are offended by the term mutilation. Health care providers should determine how each woman refers to this practice and adopt individual terminology. FGC is performed predominately on girls aged 8-12 In some cultures, it is performed several months after birth In other cultures, it is performed closer to marriage Origins There is no definitive evidence documenting when or why this ritual began Some theories suggest that it was practiced in ancient Egypt, as a sign of distinction Other theories suggest its origin in ancient Greece, Rome, Pre-Islamic Arabia, and Russia It is crucial to recognize that FGC is unrelated to Islam. It is not mentioned in the Qur’an, or the Hadith. FGC is not required by any religion FGC is practiced by members of Jewish, Christian, Muslim, and indigenous religions Although FGC is practiced predominately in Africa, variations have been found in Yemen, UAE, Malaysia, Indonesia, Pakistan, and India. Until the mid-20th century, some US physicians performed clitoridectomies to treat erotomania, lesbianism, hysteria, and clitoromegaly Worldwide Perspective African Perspective Reprinted with permission from: United Nations Children’s Fund. Coordinated strategy to abandon female genital mutilation/cutting in one generation: a human rights-based approach to programming. New York (NY): UNICEF; 2007. Available at: http://www.childinfo.org/areas/fgmc/docs/Coordinated_Strategy_to_Abandon_FGMC%20_in_One_Generation_eng. pdf. Retrieved August 31, 2007. US Perspective Of the at-risk population, close to 63% live in 7 states: California, Minnesota, NY, New Jersey, Maryland, Texas, and Virginia 46% live in 5 metropolitan areas: New York-New Jersey, Washington-Baltimore, Los Angeles-Riverside-Orange County, Minneapolis-St. Paul, and San FranciscoOakland-San Jose areas Minneapolis - St. Paul New York - New Jersey San Francisco Washington Baltimore Los Angeles Data obtained from African Women’s Health Center, Brigham and Women’s Hospital. Why is FGC Performed In some cultures, the practice of FGC is based on love and the desire to protect A cultural norm - a tradition allowing young females their inclusion into society A rite of passage from childhood to womanhood The lack of research pertaining to FGC presents a major difficulty in obtaining accurate statistics. It is estimated (in 2000) that up to 228,000 females in the US had undergone FGC or were at risk for the practice Of the at-risk females, 27% were < 18 years old An increase of 35% when compared to data collected in 1999. Why is FGC performed FGC is seen as protection in some societies In cultures that practice FGC, virginity is prized because it ensures marriagability. It is strongly believed that only a circumcised woman is desirable for marriage Uncircumcised woman are usually outcast Cultural Beliefs In some societies, the practice of FGC is driven by cultural beliefs The clitoris is considered unattractive The clitoris is believed to contribute to infertility The clitoris may be considered lethal If the clitoris comes into contact with a baby’s head during birth, the newborn may die. Lastly, in some societies, a narrow vaginal opening is believed to heighten men’s sexual pleasure In reality, many men are unable to penetrate the narrow vaginal opening and experience sexual dissatisfaction. Types of FGC The WHO has classified FGC into 4 types, based on the extent of genital excision Type Type Type Type I II - Excision III - Infibulation IV - Other FGC: Type I Excision of the prepuce and/or partial or total clitoridectomy The mildest form Because healing results in a smooth scar Type I FGC may be missed by the untrained examiner Courtesy of Nawal M. Nour, MD, MPH FGC: Type II - Excision Removal of the clitoris, accompanied by partial or total excision of the labia minora The most common form of FGC Approximately 80% of FGC cases Although no stitching is performed during Type II FGC, deep cutting of the labia minora may result in raw surfaces that fuse together during healing Creating a false infibulation or pseudo-infibulation Courtesy of Nawal M. Nour, MD, MPH Type II FGC Courtesy of National Committee Against Excision, Burkina Faso, © RAINBO FGC: Type III - Infibulation Partial or total removal of the external female genitalia, and Infibulation Reapproximation of the remnant labia majora Creation of a neo-introitus - Approximately 15% of FGC cases - Extensive damage may be done to the external genitalia, resulting in immediate and long-term health consequences. - Although Type III is mainly described as involving cutting of the clitoris, some women may have infibulation over an intact clitoris. Courtesy of Nawal M. Nour, MD, MPH Type III FGC Courtesy of Nawal M. Nour, MD, MPH FGC: Type IV - Other Describes any other form of genital manipulation Pricking, piercing or incising Stretching Cauterization Corrosive substances Manipulation Health Complications of FGC Anesthesia may or may not be administered Instruments may include knives, razors, or heated stones Instruments may be old, rusty, or dull Instruments may not be cleaned between each procedure Hemostasis via catgut suture, egg, warm oil, tar, dough, or animal excrement Girls’ legs may be bound at the ankles, above the knees, or at the thighs The girls may lie in this immobilized position for approximately one week, during the healing process. Immediate Complications of FGC Although numerous, they are rarely seen in the US Complications depend on the severity of the procedure Hemorrhage (4-19%) Laceration of the dorsal artery of the clitoris, or the labial branches of the pudendal artery Fever (22%) Acute cellulitis (15%) Tetanus (2%) Sepsis (2%) Type III FGC is especially prone to complications Binding the legs during the healing process interferes with wound drainage and may promote upward spread of infection Oliguria secondary to dehydration, urinary retention, and injury to the bladder and/or urethra may also occur Long Term Complications of FGC Common Dysmenorrhea, dyspareunia, urinary issues, infection(s), infertility Rare Hematocolpos, keloids, fistula *psychosocial issues *most long-term complications are seen in women with Type II and III FGC Keloid Formation Courtesy of CNLPE, Burkina Faso, © RAINBO Inclusion Cyst Formation Courtesy of Douglas W. Laube, MD Documentation of short- and long-term complications are unreliable, as families rarely seek medical attention for fear of prosecution It is important to note that not all women undergoing FGC experience complications For these women, acknowledging their circumcision may be the most culturallysensitive and appropriate health care practice Is HIV transmission increased? 2 theories At the time of circumcision - the same instrument may be used to circumcise many girls At the time of intercourse - the small neo-introitus (Type III) may become more traumatized during intercourse. Open lacerations could provide and easy site for HIV transmission Currently, studies have not shown an increase in HIV in FGC populations* *statistics may not be as accurate, due to under-reporting of FGC FGC: Obstetric Challenges Those with Type I or II FGC are less likely to experience obstetric difficulties. Those patients having undergone Type III FGC may pose the greatest risk Narrow neo-introitus Difficult Difficult Difficult Difficult to to to to perform accurate cervical exams place internal monitors (FSE, IUPC) place Foley catheter deliver fetal head What if a patient presents in labor with an infibulation scar? An anterior incision (defibulation) may be considered Consider blood loss, patient discomfort, psychosocial concerns If a defibulation incision is not performed The fetal head may lacerate the perineum causing hemorrhage Due to the high resistance at the introitus, the 2nd stage of labor may be prolonged It is important to discuss with your patient the possible obstetric challenges FGC patients should be given an adequate trial of labor Cesarean Deliveries should be offered only for specific fetal and maternal indications FGC: Obstetric Challenges Studies have documented an increased risk of: Cesarean Deliveries Postpartum hemorrhage Perineal lacerations Wound infections Prolonged 2nd stage of labor Separation of episiotomy scars Extended maternal hospital stay Sepsis FGC: Fetal Complications Studies (in developing nations) have also documented an increased risk of: Lower APGAR scores Infant resuscitation Low birth weight Neural damage IUFD Majority of complications occurred among women with FGC Type III Complications are unlikely to occur as frequently in the US because of extensive fetal monitoring and access to operating facilities. Defibulation AKA De-infibulation Anterior incision that opens up the infibulation scar Recreating the labia majora Removing the obstruction More difficult in patients with Infibulation inclusion cysts, abscesses, or extensive keloid formation Benefits of Defibulation Even in a patient who has not suffered FGC complications, Defibulation may prevent potential future complications. Defibulation may decrease the incidence of Chronic urinary tract infections Vaginitis Dysmenorrhea Labor complications Dyspareunia Issues surrounding Defibulation Optimum timing of Defibulation procedure May be performed at any time during a woman’s life May be preferential to perform prior to the first coital experience Decreased perineal lacerations, pain, infection, bleeding The medically optimal time for performing Defibulation may not be the best time socially or psychologically for the patient. In pregnant women, Defibulation can be safely performed during the 2nd trimester, or at least 4-6 weeks prior to delivery. Timing allows for healing of the incision prior to labor Regional anesthesia recommended due to decreased fetal and maternal risks General and Local anesthesia are also options Defibulation Counseling Counseling regarding the benefits of Defibulation may take time and may require multiple visits. Patients may not feel the procedure is necessary Risks of a surgical procedure Bleeding, infection, etc. Psychosocial issues Cultural beliefs Defibulation Procedure In Brief, Local, regional, or general anesthesia Anterior Incision Subcuticular, absorbable sutures placed on the newly formed labia Long-acting local anesthesia Assurance of hemostasis, and placement of urinary straight catheterization FGC and Physician Competency To appropriately care for a woman with FGC, the physician should display cultural competence There are many similarities and differences among women who have undergone FGC A routine gyn exam may require more explanation and time Counseling needs and psychosocial issues should be considered Be SENSITIVE ! Acknowledge the patient’s individual and cultural beliefs FGC Questions and Considerations Circumcised women may have language barriers - they may communicate primarily through their husband or other family members Some FGC patients may request postpartum Reinfibulation What if a minor requests confidential Defibulation? In 1997, it became a US federal crime to perform FGC on a girl < 18 years of age Applies to the person performing the procedure and the person consenting for the procedure Questions? References Female Genital Cutting: Clinical Management of Circumcised Women, 2nd edition. ACOG 2007 World Health Organization. Female genital mutilation - a joint WHO/UNICEF/UNFPA statement. Geneva: WHO; 1997 http://www.who.int/reproductivehealth/publications/fgm/fgm_statement.html. http://www.state.gov/g/drl/rls/hrrpt/2006. http://www.brighamandwomens.org/africanwomenscenter/FGC metro.aspx. http://www.who.int/mediacentre/factsheets/fs241/en/.