Assessing the benefits of unified transfers to multiple
advertisement

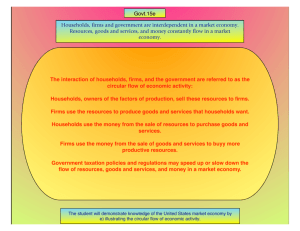
Assessing the benefits of unified transfers to multiple categories of individuals through targeting the household: Zimbabwe’s Harmonized Social Cash Transfers Leon Muwoni, UNICEF Zimbabwe The Zimbabwean Context • Low income country – recently emerged from an economic crises (2000 -2008). • hyperinflation, de-industrialization, high unemployment, large scale emigration and associated loss of skills, deteriorating balance of payments, and a decline in domestic food production • 1.9m households left poor, 500 000 of them below the food poverty line • Weakening of a well established social protection system and erosion of investments in basic services eg Education and Health 200 000 HH require urgent social assistance High levels of Poverty Harmonized Social Cash Transfers • Unconditional transfers harmonizing benefits across various categories of individuals implemented complimentary to a child protection programme • Introduced in 2011 to increase income and consumption for the households below the food poverty line, while at the same time without labour capacity • 20 out of 65 districts now covered with 55 000 households receiving cash benefits prorated to household size, ($10-25) • Targeting through modified proxy means test with a strong community verification component • Beneficiary registration through a central MIS with capabilities of providing data for other non HSCT programmes • Implementation by government with private sector partnerships in delivery and end user monitoring Implementation modalities • Targeting through modified proxy means test with a strong community verification component • Beneficiary registration through a central MIS with capabilities of providing data for other non HSCT programmes • Implementation by government with private sector partnerships in delivery and end user monitoring • Community volunteers key in delivery – get a standard support package • CIT delivery method with a mobile payment solution underway Profile of beneficiary households Table 2: Profile of recipient household members in 20 Districts Total Childre n (0 - 18) Orphans Female Male Elderly Adults Adults (19 (60+) (19 to 59) to 59) Disabled or Chronically ill adult Total 247,645 154,008 49,028 32,247 16,299 45,091 46,166 Perce nt 100% 62% 20% 13% 7% 18% 19% Table 1. Profile of beneficiary households in 20 districts Total Surveyed Total Beneficiary Households Female Headed Elderly headed (60+) Child Headed Households with Children Total 539,057 55,509 34,068 33,647 1,417 45,047 Percen t 100% 10% 61% 61% 3% 81% HSCT Impact Evaluation: American Institute of Research • two year, mixed methods, longitudinal, nonexperimental design study starting with a baseline comparing cash transfer recipient households from Phase 2 districts to eligible households in Phase 4 districts. • Includes targeting evaluation that concluded that the programme targets households below food poverty line (70%), most of them orphaned children, women (widows), people with disabilities and mostly high dependency ratio households • Focus on baseline and targeting results Reaching the most vulnerable: Analysis of targeting sample Parameters Households headed by women Source HSCT households Rural 64% Urban 49% Total 64% DHS 2010-11 44.1% 45.3% 44.6% HSCT households 19% 15% 18% DHS 2010-11 8% 4% 6.5% Percentage of children 0 - 18 HSCT Households 64% 61% 64% Percentage of children 0 - 19 DHS 2010-11 56% 45% 53% Orphans in percent of all children HSCT Households 36% 35% 36% DHS 2010-11 22% 18% 21% Household members Percentage of elderly (60+) Poverty in HSCT HH • % of HSCT beneficiaries living below both the poverty line and the food poverty line significantly higher at 97% and 81% respectively compared to the average for the rural population as a whole at 84.3% and 30% respectively. • HSCT baseline mean consumption 63% below the poverty line, compared with 43% among the rural poor. Demographic Structure of HH High rates of morbidity and chronic illness Indicator Individual Level: Chronically ill Those whose normal activity has stoppped due to chronic illness Chronically ill people receiving Home Based Care Chronically ill people receiving some kind of care (sought any care if chronically ill) People with disability Disabled population receiving care Morbidity (if sick/injured in last 30 days) Sick/injured people who sought curative care Sick/injured people who spent $ for treatment Children 0 - 5 years of age who have had diarrhea/fever/cough in last two weeks Children 0 - 5 years of age who soughtcare care for diarrhea/fever/cough Children 0 - 5 years of age who have healthcard Mean 9.9% 41.2% 3.1% 75.3% 6.0% 39.7% 25.7% 72.4% 28.8% 48.9% 58.4% 85.8% Disability • 36.6% of households had at least one disabled member and that disabled people, made up 6% of the eligible population, split up evenly between men and women. • 2012 census show disability prevalence of 7% • Disability survey 2014 – only 3.5% people with disabilities access pension or grants. • HSCT baseline – 40% of people with disabilities are primary recipients of the cash, 15% are a spouse and 20% are biological children More Orphans Orphan Status of Children Ages 0–17 Status Both parents alive (%) Single orphan: mother dead (%) Single orphan: father dead(%) Both parents dead (%) 1 HSCT ZDHS1 61.4 73.1 7.5 3.1 21.1 16.8 9.4 7.0 ZDHS sample is poorest wealth quintile from rural regions only. There are 8,438 children ages 0–17 in HSCT and 4,938 in the ZDHS sample used in this table. Child Protection and Education • Half children ages 13–20 living in beneficiary households reported having suffered physical violence in the previous 12 months. Identical to 2012 VAC study • High primary school enrolment (90%), lower for secondary (70%) • Lower attendance rate for both primary and secondary Local Economy Cost benefit • Calculations show that it costs 0.5% to GDP – coverage of all 200 000 LC and FP households • Reduces food poverty gap by 78% • At current transfer levels, 40% HH are lifted above the food poverty line and 60% have a reduced gap • Potential to reduce national food poverty rate by 3% points from 16% to 13% (national coverage) Policy Implications • Can be a building block towards building a floor of protection, considering benefits to older persons, children and high dependency households headed working age population • Phased approach to national scale to allow learning and adjustments • On budget support important –fiscal space and investment in SP • Volume of transfers – adjustments to lift HH out of extreme poverty …. But supported by other interventions to allow possible graduation Conclusion • HSCT streamlines, replaces and harmonizes most of the government social assistance programs currently implemented in Zimbabwe • HSCT will reach all children (32 percent being orphans), elderly, disabled and chronically sick persons in Zimbabwe that live in labor constrained food poor households unable to care for their vulnerable members • HSCT provides significant gender benefits as 61 percent of beneficiary households are headed by women, predominantly elderly women and widows • These benefits will be generated at annual costs of USD 60 million representing 0.51 percent of GDP. • HSCT contributes to