 Juliet Reyes
Juliet Reyes-
Sources of Trauma to the Larynx:
Behavioral Trauma (phonotrauma)◦ Vocal abuse◦ Vocal misuseMechanical Trauma◦ External sources◦ Automobile accidents◦ Assault from blunt objects◦ Penetrating injuries to larynx◦ Complications of tracheostomy◦ Internal sources◦ Improper endoscopic examination procedures◦ Endotracheal intubation◦ Indwelling nasogastric tubesTrauma due to burns◦ Thermal burns◦ Chemical burns
-
Phonotrauma to the Larynx: Behavioral Trauma: Vocal abuse
Vocal abuse◦ Yelling/screaming/cheering◦ Strained vocalizations (i.e., hyperadduction of the vocal folds because of attempts to make non-speech like sounds-plane/rocket sounds)◦ Excessive talking◦ Use of hard glottal attack◦ Throat clearing/coughing◦ Inhalation of cigarette smoke and environmental pollution◦ Poor singing technique ◦ Talking when the vocal folds are weakened◦ Cold◦ Menstrual cycle (hormone levels)◦ Allergies
-
Phonotrauma to the Larynx: Behavioral Trauma: Voice misuse
Incorrect use of different aspects of voice production;◦Inappropriate loudness/intensity◦Inappropriate pitch/frequencyIncreased loudness/pitch may result from increased stress levels and/or habitual behaviors
**Often results in increased muscle tension in larynx**
-
Puberphonia
The persistence of adolescent voice even after puberty in the absence of organic cause is known as puberphonia. This condition is commonly seen in males. The patient has an unusually high pitched voice persisting beyond puberty. This is uncommon in females because laryngeal growth spurt occurs commonly only in males.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation: laryngitis
◦Laryngitis: an inflammation of the vocal folds and larynx◦ Etiology: phonotrauma overexposure to noxious agents (tobacco, alcohol, drugs); GERD, LPR, environmental agents (allergens, dust).◦ May be acute (resulting from bacterial or viral infection) or chronic (vocal abuse/misuse).
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation: characteristics of laryngitis
◦ Perceptual: hoarseness; potential pitch changes.
Patient may complain about sensations of discomfort and dryness in the throat area
◦ Acoustic: greater than normal frequency and amplitude perturbation
-
Hyperfunction
Hyperfunctional dysphonia is one of the most common conditions associated with the voice. Also referred to as muscle tension dysphonia (MTD) or vocal hyper function, hyperfunctional dysphonia is the constriction and overexertion of the muscles around the larynx (voice box).
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation: Vocal Nodules
-benign growths on the vocal folds, usually in the anterior 1/3.◦Etiology: usually caused by vocal abuse. A reaction of the tissue to constant stress induced by frequent, hard oppositional movement of the vocal folds.◦Early nodules- often soft /pliable, may be unilateral or bilateral◦Chronic nodules- often hard, white, thick, usually bilateral
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation: Vocal Nodules - Occurrence & Characteristics
Occurrence:In adults: occur most frequently in women
• Ages 20-50
In children: occur most frequently in boys
• Ages 3-6Characteristics:
◦Perceptual: hoarseness or breathiness, patient may complain of soreness or pain in the neck, may complain of feeling something in their throat, may throat clear often◦Acoustic: Dependent of the severity of dysphonia; dependent on size of nodule◦Increased frequency and amplitude perturbation, fundamental frequency with the normal range
-
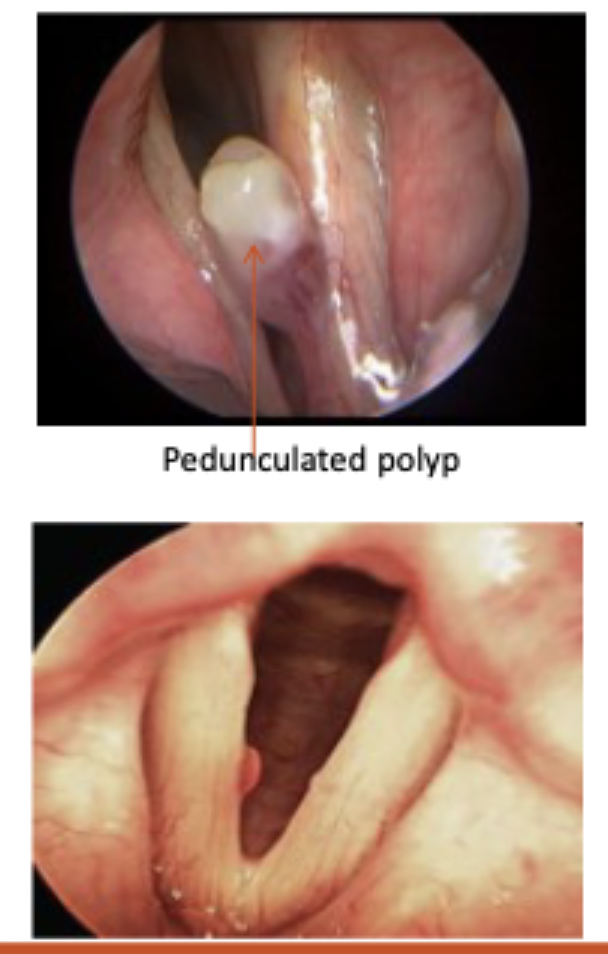
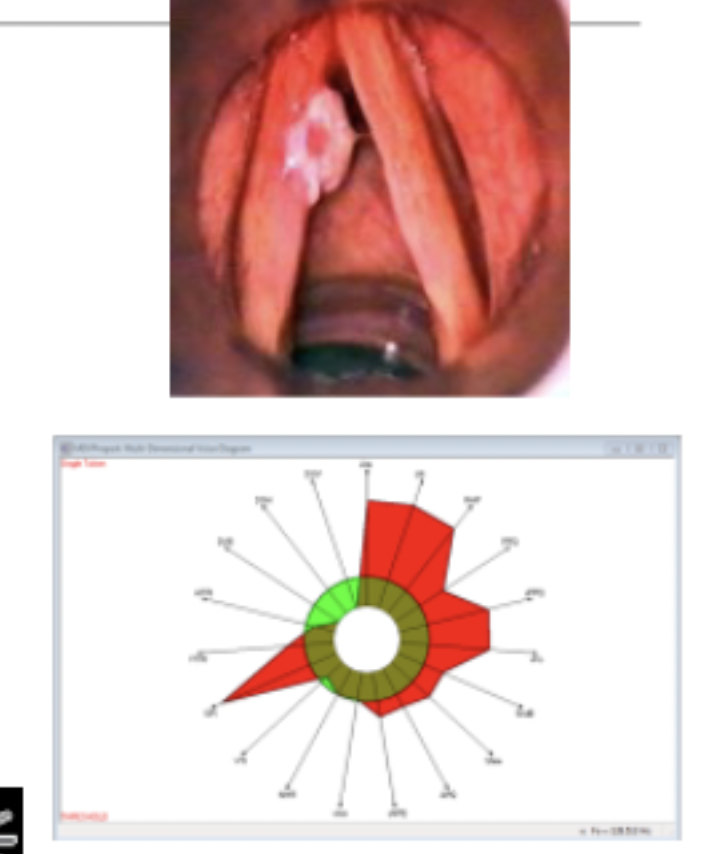
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - vocal polyps
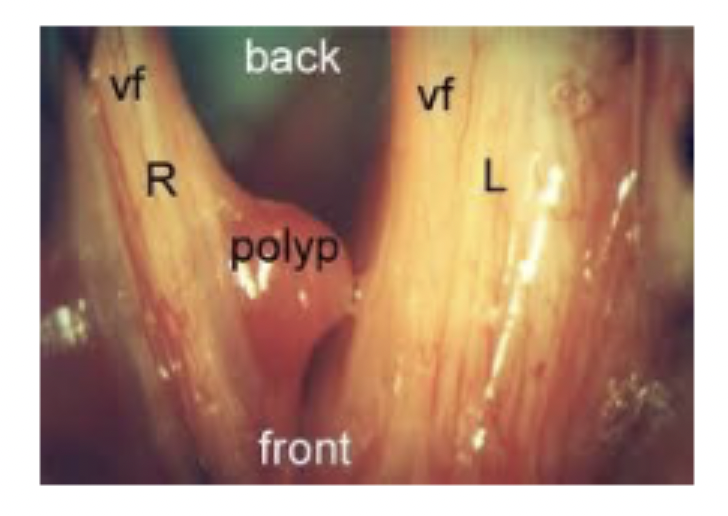
Vocal Polyps: ◦fluid filled area under the mucosal layer believed to result from a period of vocal abuse but may occur from a single traumatic incident (i.e., yelling at a concert).◦Pedunculated polyp- localized and attached to the vocal fold by a slim stalk of tissue◦Sessile polyp- closely adhering to the mucosa◦Hemorrhagic polyp- has the appearance of a blood blister
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - vocal polyps - characteristics
◦Characteristics: ◦Perceptual: ◦Hoarseness, roughness or breathiness. ◦Patient may report sensation of something in the throat.◦ NOTE: Typically, dysphonia is worse for patients with polyps compared to nodules.◦Acoustic:◦Increased jitter and shimmer depending on the site of the lesion◦Reduced phonation range.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - Reinke’s Edema
Reinke’s Edema (also known as polypoid degeneration) :◦the build-up of fluid that occurs primarily in the superficial layer of the vocal folds –the outer most layer includes Reinke’sspace (in the lamina propria)◦Etiology: Edema is the result of trauma and misuse◦Secondary to excessive use of the vocal folds or as a result of infection or inflammation◦Chronic Reinke’sedema is most often associated with smoking and is seen more frequently in females.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - Reinke’s Edema - characteristics
Reinke’s EdemaCharacteristics: ◦Perceptual: low pitch, hoarseness, may have decreased pitch range and increased effort to produce voice◦Acoustic: High cycle-to-cycle Fo perturbations◦May have significant unvoiced components◦Some SPI –slightly soft and breathy ◦May have low fundamental frequency for sex and age of patient
-
Laryngeal lesions or dysphonia caused by trauma - vocal fold cysts

• Vocal Fold Cysts: o Small spheres on the margins of the vocal folds or on superior surface of the fold. Cysts are often unilateral and frequently mistaken for early nodules or polyps.o Etiology: May be caused by the blockage of a glandular duct , causing a retention of mucosa possibly combined with phonotrauma or may be congenital.
-
Laryngeal lesions or dysphonia caused by trauma - vocal fold cysts characteristics

Cysts Characteristics:◦Perceptual: hoarseness, lowered pitch. Patient may report a “tired” voice.◦Acoustic: changes noted for females in reduced phonation range. No other changes reported
-
Laryngeal lesions or dysphonia caused by trauma - Contact Ulcer:
Contact Ulcer:◦ A benign lesion that develops on the vocal process of the arytenoid cartilages. May be unilateral or bilateral.◦ Etiology: results from vocal abuse such are regular hyperadduction of the vocal processes of the arytenoid cartilages. ◦ LPR/GERD may also be a significant factor in the formation of contact ulcers. In adults, more frequently seen in men.
-
Laryngeal lesions or dysphonia caused by trauma - Contact Ulcer characteristics:
Perceptual: low pitch (may be glottal fry), persistent hard glottal attacks. Patient may complain of pain in the larynx, vocal fatigue or referred pain to neck or ear.Acoustic: not enough data
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - Keratosis of the larynx:
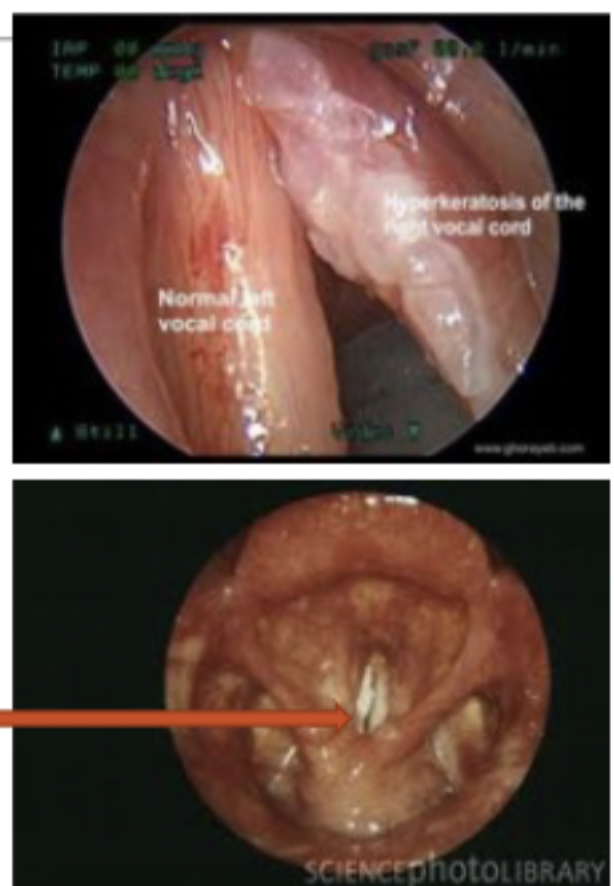
Epthelial lesions in which there is an abnormal tissue growth on the vocal folds. Originates in the epithelium but may extend into the lamina propria. A pathological condition comprised of an accumulation of keratin on the epithelial surface. Two kinds of lesions: ◦ flat, white , plaque-like lesions known as leukoplakia on the laryngeal mucosa◦ Irregular growth of the epithelium resulting in a wart-like lesion known as papillary keratosis.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - Keratosis of the larynx - etiology & characteristics
Etiology: (any combination of the following)◦ Smoking,◦ Alcohol abuse,◦ Environmental pollutants,◦ Vocal hyperfunction, ◦ Prolonged laryngitis.
Keratosis Characteristics:◦ Perceptual –hoarseness, rough vocal quality◦ Acoustic –no known data at this time.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - Laryngeal Carcinoma & etiology
• Lesions that invade the tissue and destroy the normally behaving cells.• Depending on location and size of lesion it may affect vocal fold closure.• If untreated may be life-threatening• Invasion of the tumor into various levels of the lamina propria and muscle results in greater stiffness of the vocal fold tissue.◦ May also restrict or inhibit mucosal wave movement
Etiology:May be caused by smoking (50-70% of oral and laryngeal cancer deaths are associated with smoking), environmental irritants, chemicals, metabolic disturbances, and unknown causes.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - Laryngeal Carcinoma - characteristics
Laryngeal Carcinoma Characteristics:Perceptual:• Hoarseness is the primary symptom. • May also see a lump in the neck, • Broadening of the larynx,• Tenderness in neck, • DysphagiaAcoustic:
• Frequency and amplitude perturbation will be increased.
• Changes dependent on severity of lesion.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - Hemorrhage & etiology

Hemorrhage:• A rupture of the blood vessels results in bleeding into the submucosal layer. • Reddened, edematous vocal fold appearance, usually unilateral may be bilateral.Etiology: • May result from a single episode of traumatic voice use or laryngeal trauma or a combination of heavy voice use and use of anticoagulants, and extended use of inhaled steroids.
-
Laryngeal lesions or dysphonias caused by trauma, phonotrauma, chronic irritation - hemorrhage characteristics

Hemorrhage Characteristics:◦Perceptual –hoarseness, loss of upper range, vocal fatigue, dryness. Patients may complain of pain particularly at the time of the vocal injury.◦Acoustic –no known data
-
Dysphonias caused by medical trauma to the Larynx - Laryngeal granuloma:
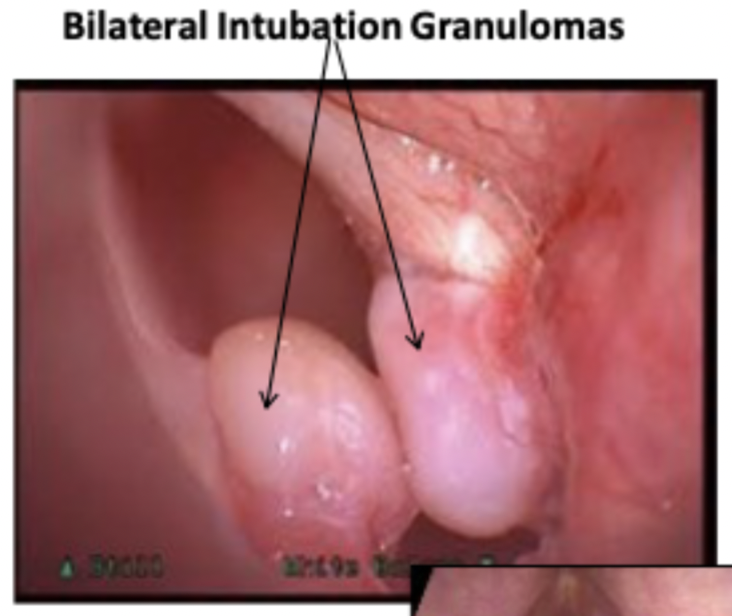
Laryngeal granuloma: Trauma to the vocal fold or vocal process due to contact with the intubation tube causing granulation tissue to form.
Etiology:• Complication of intubation dependent on:o duration of intubation, o method of intubation,o patient’s ageo Patient’s general health condition.• LPR/GERD
-
Dysphonias caused by medical trauma to the Larynx - Laryngeal granuloma: characteristics
Laryngeal Granuloma Characteristics:Perceptual –◦ breathiness and hoarseness (although some may not affect phonation depending on location)Acoustic –May present with the following vocal changes:◦ Hoarse voice with slight noise in upper frequencies◦ Short-term Fo and amplitude slightly elevated◦ Significant long-term amplitude greatly◦ Some unvoiced components◦ Inability to maintain periodic vibrtion
-
Dysphonias caused by medical trauma to the Larynx - Laryngeal Web - etiology & characteristics
Laryngeal Web: A sheet of tissue between the vocal folds usually at the anterior end.Etiology:◦ May be a result of forceful mechanical trauma or chronic infection when laryngeal tissue forms between the vocal folds.◦ NOTE: May also be congenital (we will look at this later) Characteristics:◦ Perceptual –hoarseness, high pitch (potentially secondary to the shortening of the effective vibratory length of the vocal fold due to the attachment of the vocal web◦ Acoustics –no definitive data available...what do you anticipate you will hear?
-
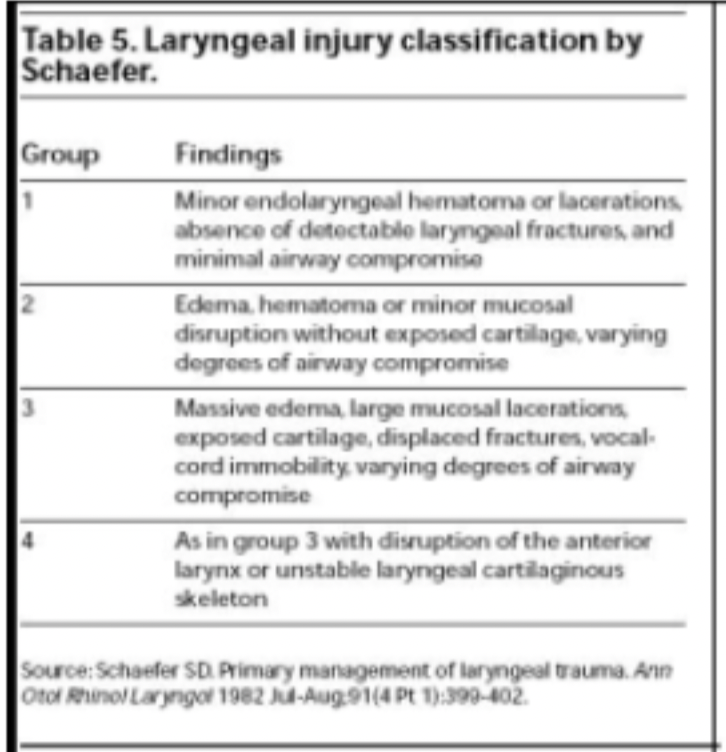
Dysphonias caused by trauma to the larynx - laryngeal fracture
-
Dysphonias caused by laryngeal burns - laryngeal burns etiology & characteristics
Laryngeal Burns: Etiology: ◦ Thermal (caused by inhalation of hot air or gases)◦ Chemical (caused of ingestion of corrosive chemicals)Characteristics:◦ Perceptual –hoarseness, may have pain during phonation◦ Characteristics may vary depending on type of burn◦ Acoustic ◦ no known data
-
Structural Anomalies of the Larynx: 3 major groups of symptoms
Three major groups of symptoms:◦Respiratory difficulty due to airway obstruction◦Vocal changes:◦Hoarseness◦Weak or aphonic cry◦Dysphagia –swallowing problems
-
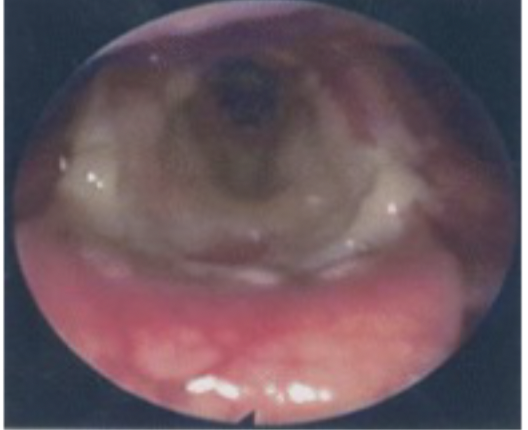
Structural Anomalies of the Larynx : Congenital Subglottic Hemangioma
◦ Large dark reddish colored masses often found in the subglottic region; ◦ Rare;◦ Typically found in children, but may occur in adults;◦ Symptoms may appear 2-3 months after birth; most growth noted between 6-12 months and then spontaneously regress in size. Characteristics:◦ Perceptual –may be asymptomatic, or stridor, hoarseness, excessive coughing.◦ Acoustic - no known data
-
Structural Anomalies of the Larynx: Congenital laryngeal webs/laryngeal atresia
◦ Connective tissue in subglottic, glottic, and supraglottic regions◦ Tissue that completely occludes the larynx at birth is known as laryngeal atresia ; airway must be opened immediately to prevent respiratory distress◦ Etiology: congenital webs are the result of a failure of the vocal fold tissue to separate during the first trimester of pregnancy.
-
Structural Anomalies of the Larynx: Congenital laryngeal webs/laryngeal atresia - characteristics:
◦ Perceptual –◦ Asymptomatic if the web is not located on the level of the glottis◦ Very depending location and extent of lesion- may affect phonation and respiration (same as previous symptoms from medical trauma causing webs.◦ Acoustic –◦ No known data –if vibratory behavior is affected will affect habitual frequency
-
Structural Anomalies of the Larynx - Fetal Laryngoscopy
The general level of obstruction can be readily identified by fetal ultrasound and magnetic resonance imaging (MRI), but determining specific causes and severity of obstruction(e.g. long-segment laryngeal atresia vs a thin membrane) has been a challenge2. • Recent progress has shown the feasibility of using fetal laryngoscopy to evaluate the vocal cords of a fetus.
-
Congenital Structural Anomalies of the Larynx - Laryngeal Cleft:
• A vertical opening between the larynx (cricoid cartilage) and the esophagus. • Cleft may be only in the region of the larynx or may form a complete laryngotracheoesophageal cleft.• Etiology: Results from a failure of the dorsal fusion of the cricoid lamina • Characteristics:• Symptoms usually occur shortly after birth; associate with other congenital anomalies• Respiration obstruction• Weak cry/aphonia• Repeated pneumonia
-
Congenital Structural Anomalies of the Larynx - Laryngocele:
◦ Air or fluid filled dilation or herniation of the saccule (a small pouch located in the anterior portion of the ventricle) extending upward within the false vocal fold.
-
Congenital Structural Anomalies of the Larynx - 3 types of Laryngocele:
◦ Three types of laryngoceles:◦ Internal laryngocele –when the inflated tissue does not penetrate the thyrohyoid membrane, but instead pushes against the false vocal folds
◦ External laryngocele –when the mass pushes up through the thyrohyoid membrane, forming a bulge or swelling on the side of the individual’s neck◦ Combination laryngocele –has features of both the internal and external types/the most common type of laryngocele.
-
Congenital Structural Anomalies of the Larynx - Laryngocele - etiology & characteristics
◦ Etiology:◦ May occur in infants/children◦ May be acquired - excessive pressure within the larynx (i.e., when a person engages in an activity that requires a lot of laryngeal pressure such as playing an instrument, weight lifting, or habitual excessive coughing from asthma or smoking). ◦ Characteristics: ◦ Perceptual –often asymptomatic in infancy. ◦ Hoarse voice or cry◦ Inspiratory stridor◦ External bulge in neck◦ Acoustic –no known data
-
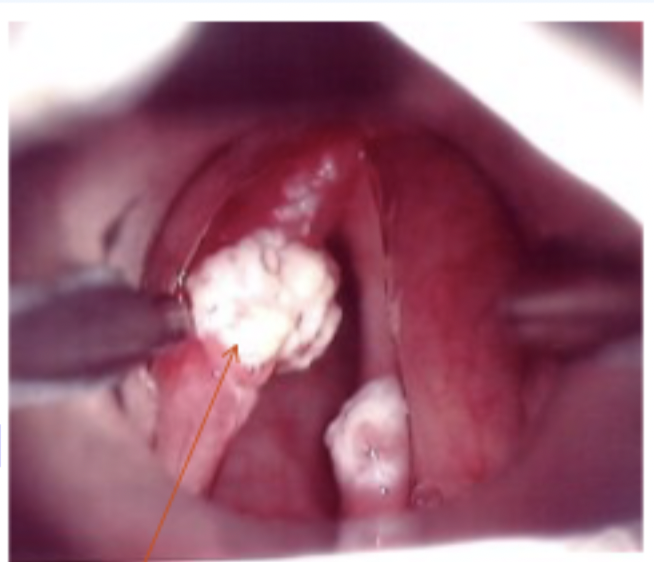
Structural Anomalies of the Larynx - Papilloma:
•A benign tumor that starts in the epithelium; may occur in various parts of the larynx (subglottal, at the level of the vocal folds and supraglottal)Etiology: •Caused by a virus (usually human papilloma virus types 6 and 11)Characteristics: •Perceptual –hoarseness, may also include low pitch, breathiness, and strained vocal quality in the adult patient. Children may present with a weak cry, chronic cough, swallowing difficulties and stridor.•Acoustic –no known data
-
Structural Anomalies of the Larynx: Laryngomalacia:
◦ Excessive flaccidity of the supraglotticlarynx◦ Inspiratory stridor◦ Spontaneous recovery in 12-18 months is often noted◦ Etiology: ◦ Congenital; Delayed or insufficient calcium deposition in infants resulting in inadequate support for the cartilaginous epiglottis; causing the epiglottis to collapse/fold over the glottis during inspiration◦ Characteristics:◦ Perceptual –inspiratory stridor; dyspnea; cyanosis; cry is normal◦ Acoustic –no known data
-
Structural Anomalies of the Larynx - Cri-du-chat syndrome: (Cat’s cry Syndrome)
◦ Identical appearance of laryngomalacia◦ Etiology: partial deletion of chromosome 5◦ Other symptoms include:◦ Mental/physical retardation, beak like profile, microcephaly, hypotonia, hyperterlorism, antimongoloid palpebral fissures, epicanthal folds, strabismus, medial oral clefts, visceral anomalies, speech and language delay. ◦ Characteristics: ◦ Perceptual –presence of a weak, wailing cry◦ Acoustic –no known data
-
Structural Anomalies of the Larynx - Subglottic stenosis:
◦ A narrowing of the airway between the glottis and the first tracheal ring◦Etiology:◦ Congenital: thickening of subglottic tissue and/or vocal folds◦ Cartilaginous narrowing of the cricoid cartilage (anterior to posterior) –small posterior opening◦ Acquired: often the result of prolonged intubation.
-
Structural Anomalies of the Larynx - Subglottic stenosis - characteristics:
• Perceptual –stridor on inhalation and exhalation, less severe cases may be perceived as croup, reduced intensity of airway is limited.• Acoustic –no known data.
-
Neurogenic dysphonias
Any dysphonia which occurs as a result of an impairment in the innervation, function or motor planning aspects of the muscles involved in respiration, phonation, and resonation/articulation resulting in a change in voice production.◦Motor Speech Disorders ◦Disorders of speech resulting from neurologic impairment affecting the motor programming or neuromuscular execution of speech.◦Dysarthria◦Apraxia◦They are NOT language or cognitive-communication problems.
-
Neurogenic dysphonias - Dysarthria/Apraxia
• A group of motor speech disorders resulting from disturbances in muscular control over the speech mechanism• Due to damage of the central or peripheral nervous system• Results from paralysis, paresis, or incoordination of the speech musculature
-
Neurogenic dysphonias - Vocal fold paralysis:
◦ Definition: ◦ When one or both vocal folds are unable to move either towards or away from midline.◦ Etiology:◦ Damage to cranial nerve X (vagus nerve) anywhere along its path from the medulla to the larynx can result in voice difficulties as a result of vocal fold paralysis◦ Approx 90% of all vf paralyses are due to peripheral causes (i.e., lower motor neuron lesions)◦ Characteristics:◦ Vf paralyses result in flaccid dysphonias due to a reduction in muscle tone resulting from a loss in of motor supply to the muscle
-
Neurogenic dysphonias - Bilateral Vocal Fold Paralysis:
◦ Usually the result of lesions high in the trunk of the vagus nerve or at the nuclei of origin in the medulla ◦ Etiology: ◦ tumors, carcinoma, or trauma; most cases are associate with intracranial pathology (hydrocephalus, etc)◦ Type: abductor or adductor; both are life threatening◦ Voice concerns are secondary to respiratory and feeding status ◦ Adductor vf paralysis: neither vocal fold is capable of moving towards the midline; making phonation impossible and placing the individual at risk for aspiration◦ Abductor vf paralysis: vocal folds remain at midline, causing serious respiratory problems; patients will often need a tracheostomy
-
Neurogenic dysphonia - Unilateral Vocal Fold Paralysis:
◦ Most common cause of unilateral vf paralysis is disruption of the recurrent laryngeal nerve (RLN) on one side. ◦ Etiology: disease or trauma to the RLN. ◦ RLN is compromised on one side, ◦ laryngeal adductor muscles (LCA, IA) cannot adduct the vf;◦ paralyzed vf remains fixed in position during both inspiration and exhalation (including during phonation)
-
Neurogenic dysphonia - Unilateral Vocal Fold Paralysis - characteristics:
◦ Perceptual –markedly dysphonic or aphonic; ◦ Vocal quality –breathy, hoarse◦ Phonation time –reduced◦ Loudness –reduced or monoloud◦ Other –diplophonia, pitch breaks
-
Neurogenic dysphonias - Myasthenia Gravis
◦ Myasthenia gravis is a chronic condition that causes muscles to tire and weaken easily.◦ an autoimmune disease in which the neuromuscular junction becomes impaired as the patient uses that particular muscle or muscle group resulting in extreme muscle fatigue◦ Muscles innervated by cranial nerves in the head and neck muscles are very vulnerable to this disease;◦ Possible difficulty swallowing◦ Results in flaccid dysarthria/dysphonia◦ Most often dx in women between ages 20 and 40 or men between ages 50 and 70.
-
Neurogenic dysphonias - Myasthenia Gravis - etiology & characteristics
◦ Etiology –◦ Damage to the receptors at the neuromuscular junction, prevent the normal transfer of impulse from the nerve in the particular muscleCharacteristics: ◦ Perceptual –◦ Typically normal voice changes to weak, breathy, barely audible voice; a few minute of voice rest, voice is restored but cannot be sustained after a brief period of usage.
-
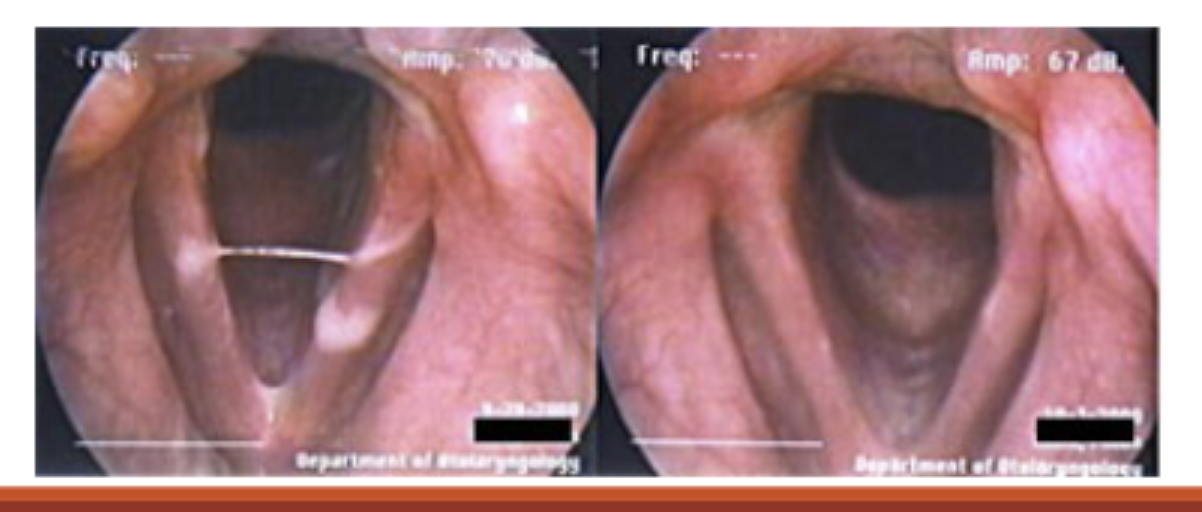
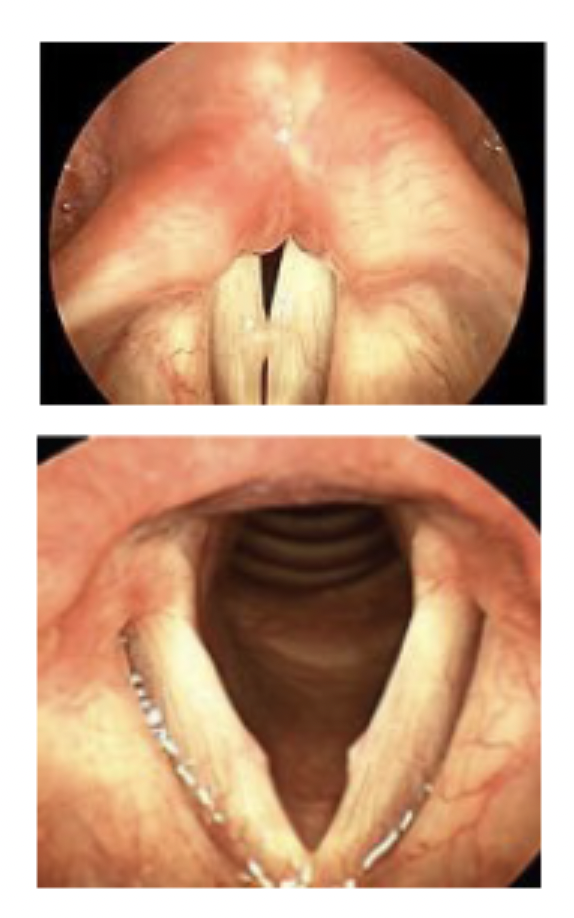
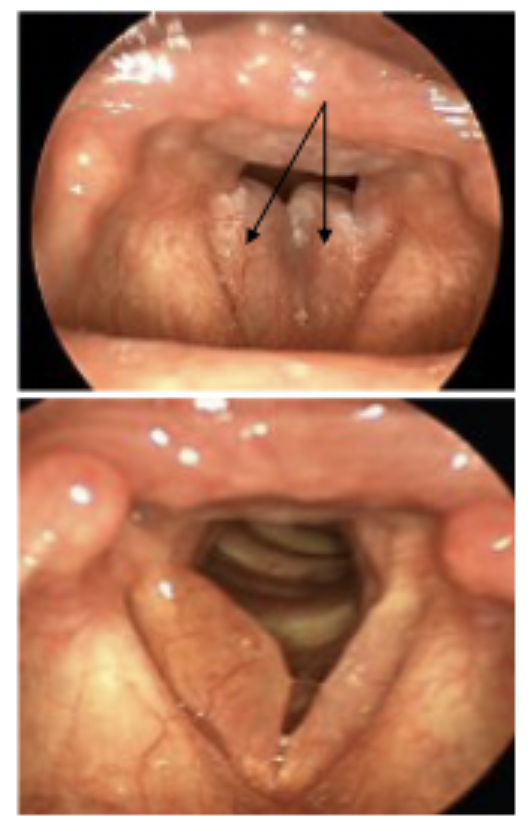
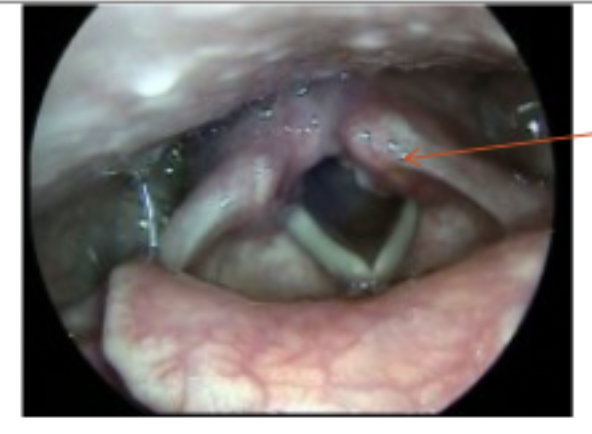
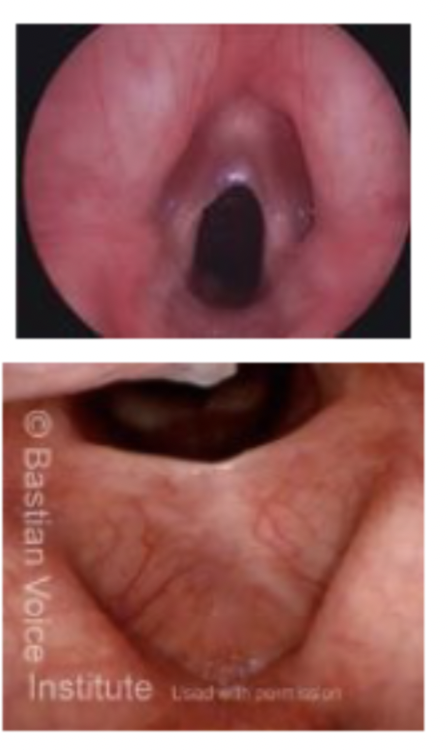
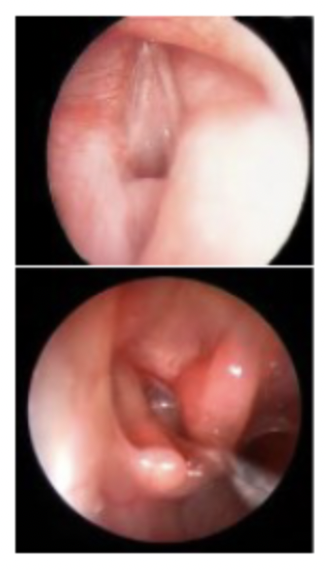
Current Research in neurogenic dysphonias
Before the neostigmine test,• the glottic openness during normal breathing was incomplete due to weakness of the abductor muscle (Picture 1) and;• glottic closure when pronouncing the “e” sound was incomplete due to weakness of the adductor muscle (Picture 2);Right after the neostigmine test, • the glottis openness during normal breathing (Picture 3) and;• closure when “pronouncing the “e” sound (Picture 4) were more complete due to enhanced performance of the abductor and adductor muscles, respectively.
-
Neurogenic dysphonias - Guillain-Barre
◦ Focal demyelination of spinal and cranial nerves◦ Flaccid dysarthria/dysphonia◦ Possible dysphagia◦ Etiology –◦ Unknown cause but frequently preceded by a viral infection◦ Affects extremities as well as facial, oral-pharyngeal and ocular muscles
-
Neurogenic dysphonias - Dysphonias related to upper motor neuron and cerebellar lesions:
◦ Lesions related to the Central Nervous System involving the pyramidal and extrapyramidal tracts◦ Spastic –◦ Muscular hypertonia: significantly increased muscle tone wherein the limb cannot be moved passively or volitionally with ease. ◦ Ataxic –◦ lesion in the cerebellum, loss of regulatory movements
-
Neurogenic dysphonias - spastic dysarthria
◦ An upper motor neuron dysphonia primarily characterized by spasticity of the laryngeal muscles.◦ Etiology: ◦ Small bilateral lesions that occur just above the nucleus of the vagus nerve◦ Degenerative disease, vascular causes, TBI, unknownCharacteristics –◦ Perceptual –◦ Vocal parameters –strained, strangled, harsh vocal quality, low pitch, monopitch/pitch breaks, monoloud/reduced/variable loudness, possible hypernasality.◦ Speech: slow, effortful, imprecise artic.
-
Neurogenic dysphonias - Dysphonias related to Disorders of the Cerebellar System - Ataxic dysarthria
◦ Cerebellar dysfunction resulting in a breakdown of the rhythmic, coordinated muscle patterns of speech (incoordination of voluntary muscle movement).◦ Related Dysphonia: changes in vocal parameters as a result of poor regulation of muscle tone and coordination of muscle activityCharacteristics –◦ Perceptual -◦ Vocal parameters: vocal quality may be normal or hoarse/harsh quality, low pitch or monopitch, monoloudness, inappropriate/imprecise prosody, excessive loudness, vocal tremor
-
Neurogenic dysphonias - Dysphonias related to Extrapyramidal System
◦ Disorders associated with a depletion of, or functional reduction in, the effect of the neurotransmitter dopamine on the activities of the basal ganglia. Acetylcholine is another type of neurotransmitter functioning within the basal ganglia.◦ An imbalance within the two neurotransmitters causes movement disorders with related dysarthrias/ dysphonias.
-
Neurogenic lesions - Hypokinetic dysarthria
an extrapyramidal movement disorder due to a depletion of dopamine in the striatum, secondary to a slow degeneration of the substantia nigra of the basal ganglia (Parkinson’s Disease).◦ Characteristics: ◦ Perceptual –◦ Vocal parameters: breathy, harsh vocal quality, reduced loudness, monoloudness, monopitch, reduced stress◦ Imprecise articulation, intermittent rushes of speech
-
Neurogenic dysphonias - Hyperkinetic dysarthria
movement disorders in which the speech muscles are “quick, jerky, and irregular”.◦ 3 Types◦ Quick –Chorea/ Huntington’s disease, Myoclonus, Tourette’s syndrome◦ Slow –Athetosis, drug-induced dyskinesia, dystonia◦ Tremor – organic voice tremor
-
Neurogenic dysphonias - chorea
◦ Chorea –a disease of the basal ganglia◦ Purposeless, irregular, fleeting, involuntary movements of the limbs and facial muscles◦ Etiology: lesions that damage the striate nucleus of the basal ganglion◦ Characteristics: ◦ Perceptual –◦ Vocal parameters (may vary depending on type) :◦ Harsh, strangled/strained , intermittent breathiness vocal quality, ◦ Limited pitch range◦ Limited loudness range, intermittent variability ◦ Inappropriate and imprecise stress patterns –disruption of prosody
-
Neurogenic dysphonias - Myoclonus
◦ a movement disorder that results in a hyperkinetic dysarthria characterized by episodic moments of abnormal speech production due to short rhythmic movements of the laryngeal and supraglottic musculature.◦ Etiology-◦ Lesions in the pathways connecting the red nucleus, the olivary bodies of the medulla and the dentate nucleus of the cerebellum.Characteristics:◦ Perceptual: Vocal parameters: voice arrest during vowel prolongation /singing◦ Myoclonus movements usually go unnoticed during connected speech.◦ Short, rhythmic contractions throughout the speech systems◦ Acoustic: Voiced/voiceless segments may be altered when compared to normal
-
Neurogenic dysphonias - Tourette’s Syndrome
episodic periods of “uncontrolled, abnormal, speech production due to rapid, tic-like movements and involuntary vocalizations◦ Etiology –unknown◦ Characteristics –◦ Perceptual: tics, dysfluency, throat clearing, coprolalia (use of obscene language), and echolalia◦ Typically, limited, if any change to voice parameters◦ Acoustic: N/A
-
Neurogenic dysphonias - Athetosis
a rare movement disorder “ characterized by involuntary, unpatterned, arhythmic wriggling and writhing movements of the head, neck, torso, and extremities.”◦ May interfere with all voluntary body movements.◦ Etiology: congenital (cerebral palsy) or acquired (neuronal degenerative disease, encephalitis, cerebral arteriosclerosis-hardening or blockage of arteries in the brain, hyperthyroidism◦ Characteristics: ◦ Perceptual :◦ Vocal parameters –hoarse, breathy vocal quality, monopitch, monoloudness or dramatic variations in loudness levels, inappropriate and imprecise stress patterns◦ Irregular movements of the face, cheeks, lips, mandible and tongue
-
Neurogenic Dysphonias - Dystonia
movement disorder characterized by “slow involuntary movements and severe postural deformities resulting from fixed muscle contractions”◦ May be focal or generalized throughout the bodyEtiology: damage to the extrapyramidal system due to encephalitis, degenerative basal ganglia disease, trauma, intoxication, unknown causes.◦ Characteristics: ◦ Perceptual : vocal parameters intermittent, harsh, strained-strangled, breathy vocal quality, limited pitch and loudness ranges, inappropriate variations in loudness, inappropriate and imprecise stress, forced inspirations and exhalation◦ Irregular movements of the lips, mandible, tongue◦ Other associated symptoms include neuromuscular and dysarthric symptoms
-
Neurogenic Dysphonias - Essential tremor
a “finely oscillating tremor” that can be found in individuals without any other conditions.◦ Etiology –idiopathic or an involuntary, benign hereditary laryngeal tremor◦ Characteristics: ◦ Perceptual: ◦ quivering intonation, voice arrests◦ Lip, mandibular, soft palate, or tongue tremor may be present◦ Acoustic:◦ Increased variation in intensity and frequency
-
Neurogenic Dysphonias - Dysphonias related to Dysarthrias of Multiple Motor Systems
dysphonias comprised of characteristics from flaccid, spastics, ataxic, hypokinetic, hyperkinetic dysarthria◦ Amyotrophic Lateral Sclerosis –a “progressive degenerative debilitating disease of the anterior horns, cranial nerve motor nuclei, and the corticobulbar and corticospinal tracts results in mixed flaccid-spastic dysarthria”◦ Onset of disease –usually middle –late age ◦ Etiology –no known etiology
-
Neurogenic dysphonias - ALS characteristics
ALS Perceptual Characteristics◦ Harsh, breathy vocal quality, monopitch, monoloudness◦ Hypernasality◦ Strained, strangled voice◦ See Table for additional speech/voice changes• ALS Acoustic Characteristics◦ Increase noted in stop gaps in stop consonants and vowel durations ◦ Changes in fundamental frequency, jitter, shimmer, intensity and HNR seem to be most affected
-
Neurogenic Dysphonias - Multiple Sclerosis
a demyelinating disease characterized by deposits of plaque anywhere in the central nervous system. ◦ Symptoms may be mild initially with long period of remission or latency in between episodes. Severity of symptoms increase as disease progresses. ◦ Results in a mixed dysarthria (impacts multiple motor systems)◦ Occurs around age 30◦ Etiology: unknown, assumed to be an autoimmune disorder
-
Neurogenic Dysphonias - Multiple Sclerosis - characteristics
◦ Perceptual:◦ vocal parameters include harsh vocal quality, reduced pitch and impaired loudness control, hypernasality◦ Poor respiration, poor sustained phonation◦ Associated symptoms: ◦ Articulation errors◦ Decreased neuromuscular coordination for respiration; decreased vital capacity◦ Nystagmus (A rapid, involuntary, oscillatory motion of the eyeball)
-
Neurogenic Dysphonias - Wilson’s Disease
progressive lenticular degeneration which results in a mixed ataxic-hypokinetic-spastic dysarthria◦ Etiology –inadequate processing of dietary copper due to a rare, inherited autosomal recessive disorder◦ Characteristics –◦ Perceptual : ◦ Vocal parameters –harsh vocal quality, low pitch, reduced range of pitch and loudness◦ Acoustic: ◦ No definitive parameters ◦ Motor speech symptoms: difficulty noted in the face, lips, mandible, velopharyngeal movement◦ Neuromuscular symptoms
-
Neurogenic Dysphonias - Spasmodic Dysphonia
◦ Cause: increasing evidence that most cases of spasmodic dysphonia are neurogenic or having to do with the nervous system (brain and nerves-probably supranuclear although once thought psychogenic). „ • AD type• VF's spasm shut◦ Vocal strain, voice blocks • AB type ◦ VF's spasm open ◦ Breathy voice, aphonic moments ◦ Worse during unvoiced consonants „ • Mixed type• TASK SPECIFIC! Symptoms only occur during connected speech
-
Neurogenic Dysphonias - Dysphonias associated with Apraxia of phonation◦ Apraxia of Speech
◦ Etiology –a lesion that separates Broca’s area from the motor association area that deals with motor planning; most often secondary to a CVA.◦ Characteristics: ◦ Perceptual: ◦ Vocal parameters –may have intermittent aphonia, voicing errors◦ Acoustic:◦ No definitive parameters ◦ May have an absence of voluntary or imitative respirationAssociated symptoms –◦ changes in motor programming for articulation◦ pauses or hesitations in conversation speech
-
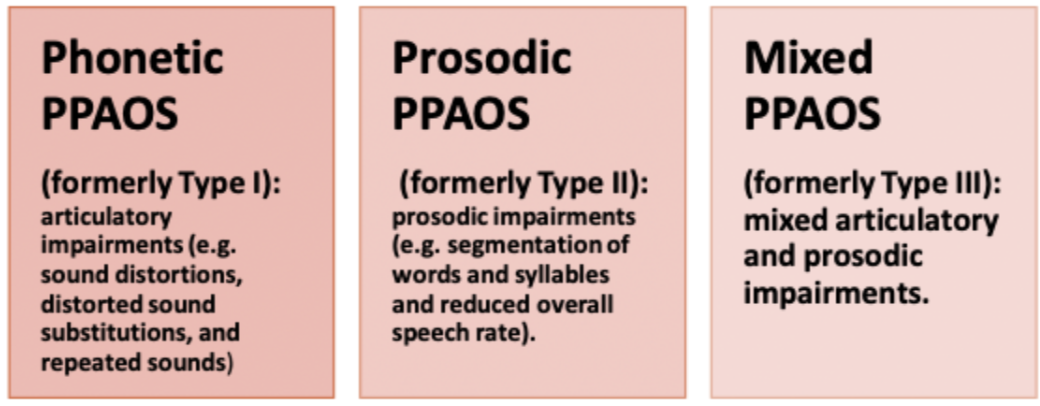
Neurogenic Dysphonias - Primary Progressive Apraxia of Speech (PPAOS)
• A recently described neurodegenerative disorder in which patients present with an isolated apraxia of speech.• Focal degeneration of superior premotor and supplementary areas implicated.• Due to the novel nature of PPAOS, there is limited understanding of the progression of this disease.
-
Neurogenic DysphoniasTypes of PPAOS
-
Resonance disorders - Hypernasality:
•excessive nasal resonance during non nasal sounds (i.e., vowels and vocalic consonants)•Etiology: velopharyngeal incompetence or failure of the velopharyngeal port to attain and/or maintain sufficient closure; • Organic and nonorganic etiologies where velopharyngeal closure is negatively affected.◦ Structural deficits: (i.e., cleft palate)◦ Neurologic deficits:(i.e., spastic dysarthria)• Vocal parameters –increased nasal resonance◦ Non organic: no associate symptoms◦ Hypernasal non-organic voice sample◦ Organic: faulty articulation, nasal emissions, facial grimacing, laryngeal abnormalities, reduced intensity/loudness
-
Resonance disorders - Hyponasality:
◦ Speech productions that are deficient or lacking in nasal resonance.Etiology:◦ Organic origin: more typical- resulting from an obstruction in the nasopharyngeal area◦ Enlarged adenoids, nasal polyps, allergies resulting in edema of the nasal membranes, nasal papilloma, trauma in the nasal area, tumors, mucosal congestion, high palatal arch, overcorrection for hypernasality◦ Non organic origin: uncommon◦ May be residual after organic origin is resolved; desired resonance• Vocal parameters - Voice has a “muted” sound, sounds like patient has a “head cold”.
-
Resonance disorders - Mixed resonance:
Evidence for both hypernasality due to velopharyngeal dysfunction and hyponasality• May be due to nasal obstruction• Often reduced nasal air emission from one naris on mirror exam
-
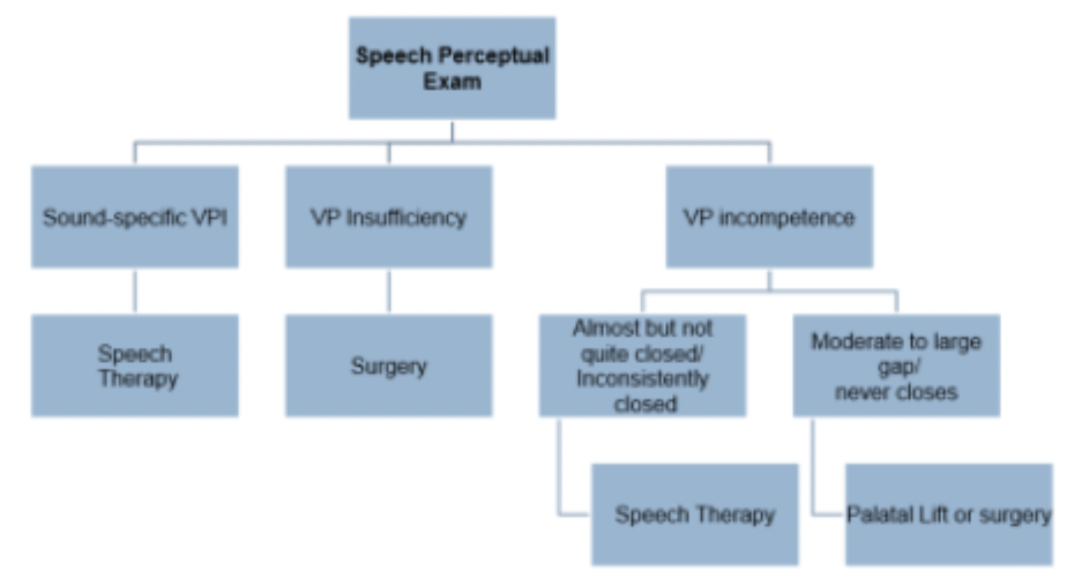
Resonance disorders: assessment/recommendations
-
Resonance disorders - Cul-de-sac resonance:
◦ a “muffled and hollow” vocal quality, lacking full resonance.Etiology: tongue deeply retracted and posteriorly placed in the pharynx◦ Usually a nonorganic basis◦ May occur due to organic origin such as deafness, flaccid and spastic dysarthria, athetoid cerebral palsy, and oral apraxia.
-
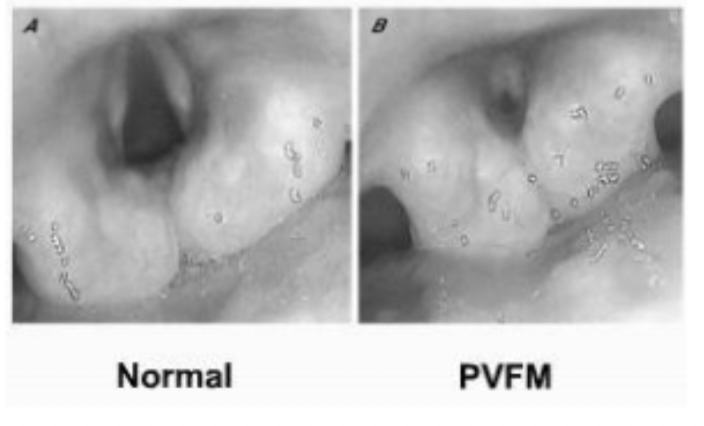
Functional voice disorder - Paradoxical vocal fold motion (PVFM):
• Airway obstruction due to vocal fold closure• Occurs during speech and inhalation• Etiology: no definitive etiology, frequently mistaken for asthma◦ Possible causes:1. psychological causes2. airway hyperactivity3. potential neurogenic causes4. pharmacological5. unspecified
-
Functional voice disorder - Paradoxical vocal fold motion (PVFM) - vocal/non-vocal
• PVFM Symptoms: may be consistent or variable• Vocal-
◦ Breathy, weak phonation,◦ Hoarseness◦ Inspiratory stridor• Nonvocal-
◦ Throat tightness,◦ Wheezing◦ Chest tightness◦ Shortness of breath◦ Cough
-
Functional voice disorder - What is Muscle Tension Dysphonia? (MTD)
Excess or dysregulated/imbalanced activity of the intrinsicand extrinsic laryngeal muscles is the primary cause of thevoice disturbance.• A voice disorder in the absence of visible structural orneurological laryngeal pathology (or where the vocal foldpathology is insufficient to explain the degree of thedysphonia).
-
Functional voice disorder -MTD: Sources of excessive/dysregulated laryngeal muscle activity...
• Psychological &/or personality factors induce laryngeal tension. • Technical misuses of the vocal mechanism. • Learned adaptations following upper respiratory infection. • Extreme compensation for underlying vocal fold pathology. Increased laryngeal tone secondary to LPR.
-
Functional Voice disorder -MTD: Broad Conceptualization
• Key feature is laryngeal and paralaryngeal hypertonicity • No particular voice quality or glottic configuration is uniquely identified with MTD. • Extrinsic and intrinsic laryngeal muscle dysregulation contributes to the abnormal voice. • Muscle tension pulls larynx out of “natural” position. • Larynx is suspended high in the neck & the entire hyoid-laryngeal sling is stiff
-
Functional voice disorder -Symptoms of Excess Laryngeal Muscle Tension:
• Laryngeal tenderness, soreness, pain, tightness which intensifies with extended voice use (especially with palpation) • Unilateral symptoms are more common• Pain radiates to one or both ears/fullness of the ears • Vocal fatigue, increased effort, “swellings” in the tongue base/neck regions • Dynamic range restricted (decreased loudness/pitch) • May be seen/witnessed in voice and or dysphagic patients
-
Age-related voice changes - Presbyphonia
• Etiology: Aging of the vocal mechanism• Perceptual characteristics: ◦ Altered pitch (male –rising;female –lowering)◦ Hoarseness; roughness, breathiness, strain, slowed rate of speech• Visual characteristics: ◦ Bowing of the vocal fold edge, vocal fold atrophy, a spindle shaped gap during phonation.
-
Age-related voice changes - Presbyphonia - Acoustic characteristics:
◦ Increased F0 in males◦ Decreased F0 in females ◦ Decreased intensity ◦ Increased noise-to-harmonics ratioNOTE: ◦ Presbyphonic changes are not atypical in otherwise healthy elderly individuals.◦ Presbyphonia can significantly impact quality of life.

