 Juliet Reyes
Juliet Reyes-
How does flaccid dysarthria occur?
- produced by a LMN lesion & causes damage to cranial & spinal nerves
-
Etiologies of flaccid dysarthria:
- brainstem stroke
- guillian barre syndrome: demylenization of spinal & cranial nerves
- myasthenia gravis: autoimmune disease that destroys Ach receptors on muscles
- muscular dystrophy: degeneration of m fibers & connective tissue
-
Flaccid Dysarthria
◦Best distinguishing features for flaccid dys.:◦Hypernasality, nasal emission, continuous breathiness, stridor◦May also hear:◦Hoarseness, harshness, diplophonia, monopitch, monoloudness, short phrases, imprecise articulation◦Everything we hear can be traced to weakness
-
Spastic dysarthria
Oral Motor Exam:
- pathological oral reflexes (suck, snout, jaw jerk reflex)
- drooling
- pseudo bulbar affect
- slow, regular AMRs
Articulation:
- imprecise articulation w/ distorted vowels
Resonance:
- hyper nasality
Prosody:
- short phrases
- monopitch & monoloudness
- excess & equal stress
- slow rate
phonation:
- low pitch
- strained strangled voice
- pitch breaks
-
How does spastic dysarthria occur?
- bilateral UMN damage
-
etiologies of spastic dysarthria:
- ALS:
- TBI
- Multiple sclerosis
-
how does ataxic dysarthria occur?
cerebellar damage
-
ataxic dysarthria
oral motor exam:
- hypotonia
- slow voluntary movements
- jerkiness of movement
- wide-based gait
- intention tremor
- dysmetric jaw, face & tongue AMRs
articulation:
- irregular, transient articulatory breakdowns
- vowel distortions
prosody:
- excess, equal stress
phonation:
- excess loudness variations
-
hypokinetic dysarthria occurs by:
damage to basal ganglia
-
hypokinetic dysarthria caused by:
- anti-psychotic medications
- head trauma
- associated with parkinson's
-
hypokinetic dysarthria:
oral motor exam:
- limited ROM
- resting tremor
- masked facies
articulation:
- Bradykinesia: reduced speed of muscles
- hesitations & false starts
- slow speech
- rigidity
- reduced loudness
- imprecise consonant production
- reduced pitch variability
- festinating speech
prosody:
- Monopitch & monoloudness
- palalia
phonation:
- hoarseness
- low volume
-
hyperkinetic dysarthria occurs by:
damage to the basal ganglia
- may be unilateral or bilateral damage
-
hyperkinetic dysarthria
articulation/speech:
- irregular consonant & vowel distortions
- slow, irregular AMRs
resonance:
- intermittent hypernasality
prosody:
- inappropriate silences
- excess loudness variations
- excessive/variable stress patterns
phonation:
- voice stoppages
- strained-harsh voice
- audible inspiration
- tremor like voice
-
unilateral UMN dysarthria
Articulation:
- imprecise artic
- slow rate, slow AMRs
Resonance: WNL
Phonation:
- sometimes hoarseness/harshness
- occasional reduced loudness
-
ALS
- spastic-flaccid dysarthria
atrophy & fasciculations
strained strangled voice
slow rate
-
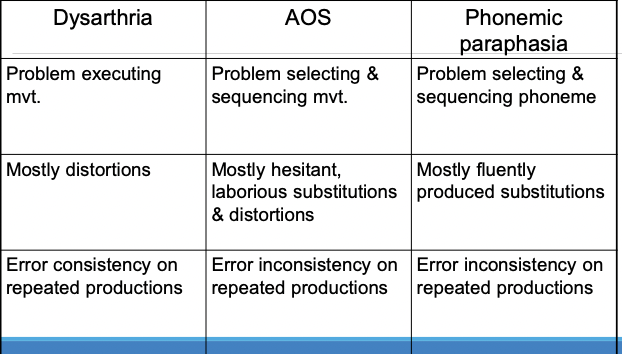
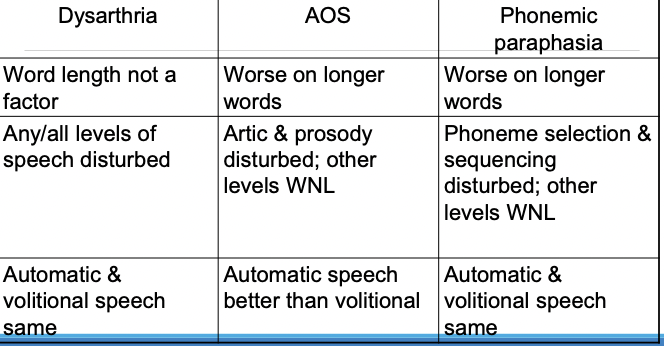
Dysarthria vs AOS vs paraphasias
-
dysarthria vs AOS vs paraphasias
-
AOS
MSD resulting from disturbed planning or programming of volitional speech actions/patterns in the absence of paralysis, paresis, or incoordination
-
AOS speech characteristics
◦Slow rate of speech◦Articulatory groping◦Errors of phoneme distortion and substitution ◦Syllable segmentation◦Disturbed prosody –misassigned/abnormal stress◦Initiation of speech and artic. transitions are particularly difficult◦Prolonged cons., vowels, and inter sound, syllable, and word durations
-
AOS vs paraphasias
AOS◦Errors mostly initial◦Errors more related to phonetic complexity◦Sequencing errors rare◦Additions rare◦Abnormal fluency◦Syllable segmentation
Paraphasia◦Errors can be anywhere◦Errors less related to phonetic complexity◦Sequencing errors common◦Additions common◦Normal fluency◦No syllable segmentation
-
Severe AOS
Speech characteristics depart from less severe form◦Reduced variability of articulatory characteristics:◦Limited speech sound repertoire◦Speech may be limited to a few meaningful or unintelligible utterances◦Imitation of isolated sounds may be in error, and errors may be limited in variety◦Errors may be highly predictable◦Automatic speech may not be better than volitional◦Muteness may be present, but rarely for longer than 1 or 2 weeks if 2°AOS◦Usu. accompanied by severe aphasia and nonverbal oral apraxia
-
Primary Progressive AOS(PPAOS)
AOS of insidious onset, gradual progression & prolonged course in which AOS is the first, only, or most salient feature & in which criteria are not met for diagnosis of another neurodegenerative disease
-
PPAOS speech features
• Slow overall speech rate• Lengthened segments between words• Sound distortions• Increased sound distortions or distorted sound substitutions as utterance length or complexity increases• Syllable segmentation within multisyllabic words
-
types of PPAOS
• Type 1: predominantly articulatory abnormalities• Distortions & distorted substitutions, repeated sounds, attempted self-correction• More evident when aphasia is present & > AOS• Tends to be association with widespread involvement in premotor, prefrontal, temporal-parietal lobes, caudate, & insula• Type 2: predominantly prosodic abnormalities• Segmentation of words & syllables• More evident in PPAOS without aphasia• Tends to be associated with involvement in premotor cortex & midbrain atrophy• Type 3: no clear difference in prominence of articulatory vs. prosodic abnormalities

