 Youssef Draz
Youssef Draz
A.F. 2024 0 Physiology for 2nd year medical students Motor Final
-
Monosynaptic spinal reflex= Stretch reflex = (myotatic reflex).
• only monosynaptic reflex
• Def: Stretch of an innervated muscle is followed by its contraction.
• Components:
▪ Stimulus: Stretch of muscle.
▪ Receptor: Muscle spindle (intrafusal fibers).
▪ Afferent: Primary and secondary endings.
▪ Center: Anterior horn cells ( AHCs)
▪ Efferent: Motor nerve (A alfa motor fibers).
▪ Effector organ: Skeletal muscle (extrafusal fibers)
▪ Response:
1) Contraction of the same muscle
2) informs CNS about length of the muscle. (part of position sensation
-
Structure of muscle spindle:
• Intrafusal fibers:
▪ 8-10 muscle fibers, enclosed in a spindle shaped connective tissue capsule.
▪ smaller than extrafusal fibers and parallel to them
▪ Each fibre consists of:
1. Central non- contractile area: the receptor area
2. Peripheral contractile part
Types:
1. Nuclear bag fibres: central area dilated with aggregation of nuclei
2. Nuclear chain fibres (smaller): one line of nuclei spread in a chain in receptor area
N.B.: ends of capsule are attached to muscle tendon or sides of extrafusal fibers.
-
Innervation of muscle spindle
Afferent fibres:
Primary (annulo spiral) endings
fibres: group la: thick rapid (up to 120 m/s)
encircle: both nuclear bag and chain
secondary (flower-spray) endings
fibres: group II smaller myelinated fibers
encircle: nuclear chain fibres only
• Afferents enter spinal cord and either:
a. End directly on motor neurons supplying extrafusal fibers of same muscle.
b. Ascend to: Cerebellum & Cerebral cortex:
CNS informed about muscle length and rate of length change
II. Efferent (motor) fibres: gamma motor neurons in anterior horn of spinal cord
▪ supply peripheral contractile parts of intrafusal fibres
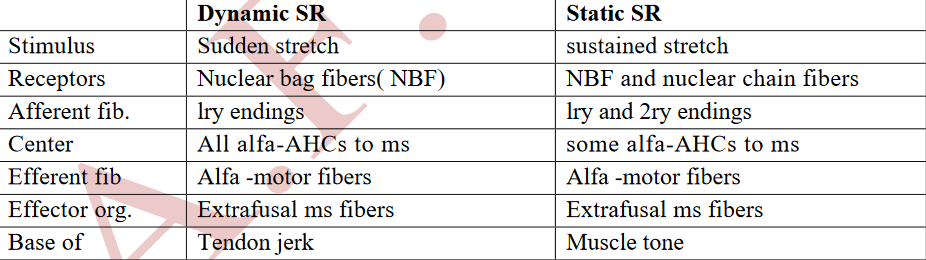
1. Dynamic: to nuclear bag fibres (as plate endings).
2. Static: to nuclear chain fibres (as trail endings)z
-
conditions of Excitation of muscle spindles:(Stretch of whole muscle)
• spindle is parallel with extrafusal f i b e r s .
•when muscle is passively stretched stretched.
• initiates reflex contraction of extrafusal fibers
• feedback device operates to maintain muscle length
-
conditions of Excitation of muscle spindles:(Contraction of intrafusal fibres by gamma efferents (without stretch of extrafusal fibers):)
• gamma neurons cause contraction in peripheral contractile part of intrafusal fibers
• receptors in center will be stretched.
• causes stimulation of primary endings encircling receptor area.
• Afferents enter spinal cord and stimulate alpha neurons → extrafusal fibres
contract
-
conditions of Excitation of muscle spindles:(Maximum stimulation of muscle spindles)
Both stretch of whole muscle and increased discharge of gamma efferents in same time.
-
conditions of Excitation of muscle spindles:(Minimal or no stimulation)
• when muscle actively contracts because spindles lie in parallel with extrafusal fibres.
• Unloading: reduction of firing from spindles during muscle contraction
▪ if there is shortening of extrafusal fibres without shorting of intrafusal fibers
▪ Disadvantages : CNS no longer receive information about extent and rate of
change of muscle length.
-
conditions of Excitation of muscle spindles:(Activity of gamma motor neurons prevent unloading: cortex sends impulses to both)
a. Alfa motor neurons: shorten extrafusal fibres
b. Gamma motor neurons: shorten peripheral contractile parts of intrafusal fibres.
• Functions:
a. maintains firing to CNS (informed about changes in muscle length).
b. helps cerebral cortex to re-adjust motor commands to spinal motor neurons.
-
Physiological significance of stretch reflex
1. Helps to maintain muscle length
2. Control of voluntary movements.
3. Muscle tone
-
Q. Role of muscle spindle in control of voluntary movements
Servo-Assistant function: during muscle contraction
• impulses from higher centers to do voluntary movement stimulate alpha and gamma neurons simultaneously.
a. alfa activates extrafusal fibers.
b. gamma leads to contraction of peripheral parts of intrafusal fibers with subsequent stretch of central (receptor) part → reflex activation of extrafusal muscle fibers.
• Because of "alfa- gamma linkage", contractile part of spindle shortens with muscle:spindle discharge continue throughout contraction.
• Main advantage: efficient load compensation: If extrafusal fibers are stretched by sudden load, intrafusal fibers will be stretched also which will lead to reflex contraction of the extrafusal fibers
-
Q. Role of muscle spindle in control of voluntary movements
Damping function: (Smoothen muscle contraction).
• signals from cortex to AHCS are unsmooth → oscillatory (jerky) movements.
• stretch reflex prevents oscillation and smoothen contraction.
• Proof: Cutting sensory nerves from muscle (de-affrentiation) = loss of stretch reflex →un-smooth jerky muscle contraction
-
Role of muscle spindle in muscle tone
• Muscle tone: continuous, alternating, reflex, subtetanic contraction of muscle fibers or
resistance of the muscle to stretch.
• Base of muscle tone: Static stretch reflex
• During rest: muscle spindle is continuously stretched because:
1) length of skeletal muscle is normally shorter than distance between origin and
insertion (muscles are in mild stretch).
2) gravity causes lengthening of musclese specially antigravity: extensors of lower
limbs, trunk and neck & flexors of upper limbs and elevators of jaw
3) Continuous gamma -efferent discharge: stretch of receptor portions of spindles.
-
Role of muscle spindle in muscle tone
• Muscle tone does not cause fatigue because:
1. alternate contraction of different muscle fibres.
2. Contraction is subtetanic.
3. fibres are red (contract slowly and sustain force for a long time).
• Functions of muscle tone
1) Maintain body posture against gravity.
2) Provides a background for voluntary movements.
3) Helps in regulation of body temperature (resting heat production).
4) Helps venous and lymph return (squeezing veins and lymphatic’s).
-
Functions of gamma stimulation:
1) Prevent unloading: Keep spindle taut throughout motion = sensitive to stretch as muscle contracts (loading)
2) maintains muscle tone
3) Servo-Assistant function
-
Supraspinal control of stretch reflex:
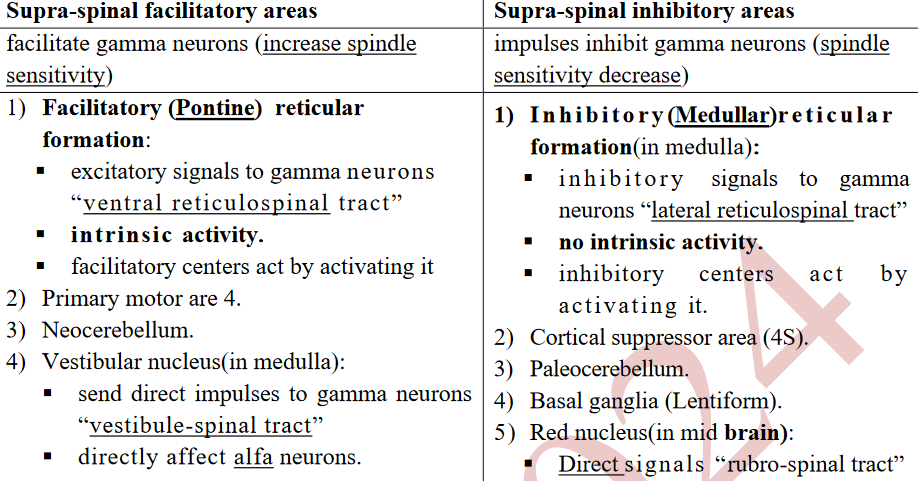
Experimental proof (Decerebrate rigidity): section between pons and mid- brain.
▪ remove input from cortex, red nuclei and basal ganglia that stimulate inhibitory RF.
▪ discharge of facilitatory RF& vestibular nuclei continues but inhibitory RF decrease
▪ gamma efferent discharge is increased and stretch reflex becomes hyperactive
causing marked rigidity of antigravity muscles.
-
Types of stretch reflex (response)
-
Clinical significance
-
Inverse stretch reflex (autogenic inhibition):
• Stimulus: increased tension in muscle
• receptor: Golgi tendon organ
- in series with fibres: stimulated by both passive stretch and active contraction.
- Discharge is regularly produced by contraction of muscle.
• Afferent: Ib (rapid): IPSPS on motor neurons (by inhibitory interneurons)
• Response: contraction suddenly stops and muscle relaxes:
• Function: feedback circuit regulates muscle force
• Importance: transducer in a feedback circuit that regulates muscle force in a
fashion similar to the spindle feedback circuit that regulates muscle length
-
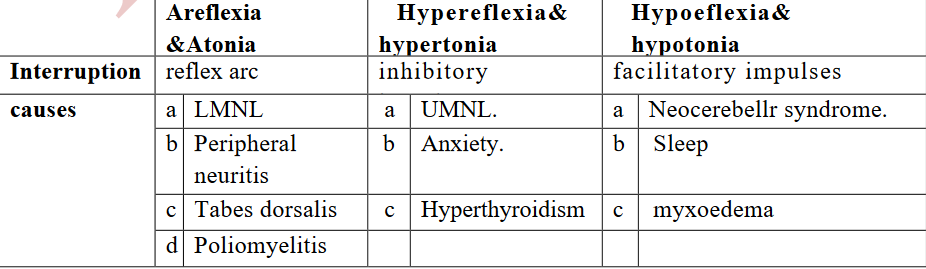
Findings associated with hypertonia
1. Lengthening reaction (response of spastic muscle to lengthening):
• sequence of resistance & give way when a limb is moved passively
• Passive extension meets immediate resistance due to activation of stretch reflex
• Further stretch activates inverse stretch reflex: resistance suddenly disappears
• Known clinically as clasp-knife as it resembles closing a pocket knife.
• More in antigravity muscles (increased gamma discharge)
2. Clonus: regular, rhythmic contractions of muscle subjected to sudden maintained stretch.
• Ankle clonus
▪ initiated by brisk, maintained dorsiflexion of foot
▪ response: rhythmic planter flexion at ankle.
▪ stretch reflex & inverse stretch reflex sequence contribute to this response
-
Spinal cord lesions
complete transection as a result of:
1) road accidents causing fracture of vertebrae.
2) primary tumors or metastasis from malignant tumors.
• higher level of section, more serious consequences:
a) upper cervical: immediate death (paralysis of all respiratory muscles).
b) lower cervical: quadriplegia with diaphragmatic respiration.
c) thoracic region:
- normal respiration
- paralysis of both lower limbs i.e. paraplegia.
- lose all sensations and voluntary activities(section of all sensory and motor tracts
-
Stages with regards to spinal cord reflex(Stage of spinal shock:immediately after transection)
• cause: sudden withdrawal of facilitatory descending tracts
• RMP of spinal motor neurons ( 2-6 mv) greater ( hyperpolarized)
• features (below level of lesion):
1) Loss of all reflexes:
1. superficial
2. Deep (as muscle tone):
▪ loss of muscle tone results in falcidity → decreased muscle pump: reduced
venous return → limbs become cold and blue.
3. visceral (micturition, defecation and erection):
▪ walls of urina ry bl a d de r a nd r e ctu m a re pa r aly z ed b ut t on e i n internal
urethral (or anal) sphincter returns very rapidly.
▪ Result: "retention with overflow”: accumulation of urine until pressure
overcomes resistance of internal sphincter: dribbling of urine.
-
Stages with regards to spinal cord reflex(Stage of spinal shock:immediately after transection)
2) Loss of vasomotor tone =fall in blood pressure:
o interruption of fibers that connect vasomotor centers with lateral horn cells.
o relative vasodilatation causes an immediate fall in blood pressure.
o higher the level of section, lower the blood pressure.
3) Bed sores "decubitus ulcers":
o at sites where body weight hinders circulation to skin (over bony prominences i.e. back, heel and gluteal region).
o skin "sloughs off' at these sites, forming ulcers that heal with difficulty
o cause: mobilization and cleaning of these areas is neglected.
• duration : (2-6 w in humans) : depend on degree of encephalization ( dominance of cerebral cortex):higher brain development longer is the duration.
-
stage of recovery of reflexes:
some reflex activity is recovered.
• Cause of recovery :
1) denervation hypersensitivity: to mediators released by remaining excitatory endings.
2) sprouting of collateral from existing neurons with formation of additional excitatory endings on inter neurons and motor neurons.
-
stage of recovery of reflexes:Early recovery
Gradual rise of arterial blood pressure:
▪ regaining of activity in lateral horn cells (spinal vasomotor center)
▪ vasomotor control from medulla is absent: sudden fall in blood-pressure on
being made to sit up or stand.
2. Return of reflexes:
1) Superficial: planter reflex: positive Babinski sign.
2) Deep: e.g. knee jerk also recovers
▪ Flexor reflexes return earlier than extensor ones.
▪ return of flexor tone ”paraplegia in flexion".
▪ return of tone in arterioles and venules improve limb circulation.
3) visceral reflexes:
• return of function of bladder and rectum (automatic),
• voluntary control and sensation of fullness are permanently lost
-
stage of recovery of reflexes:Early recovery
4) Mass reflex:
• Reflects high excitability of spinal cord neurons.
• Stimulus: minor painful to skin of lower limbs
• response:
1) Flexion withdrawal of the limb.
2) Evacuation of bladder and rectum
3) Sweating.
4) Rise of blood pressure.
• used to give degree of bladder and bowel control. “intentional mass reflex”.
5) Sexual reflexes: Genital manipulation produces erection and even ejaculation
-
stage of recovery of reflexes:Advanced recovery =after rehabilitation
• proper management drive patient into a more advanced stage of recovery:
1) tone in extensors gradually returns and becomes greater than flexors,
"paraplegia in extension" .
2) Positive supporting reflex becomes well developed and patient stand without support.
-
stage of recovery of reflexes: Stage of failure of reflexes
• Infection, malnutrition and other complications inhibit spinal reflex activity.
• proper care e.g. mobilization to prevent bedsores, use of antibiotics and attention to
nutrition and fluid balance have reduced mortality from 80% to 6%.
-
Brain stem( Functions: contains centers that:)
1. Regulate cardiovascular, respiratory and GIT functions.
2. major role in control of eye movements.
3. Support body against gravity
4. Control complex reflex movements.
-
Brain stem(reticular formation)
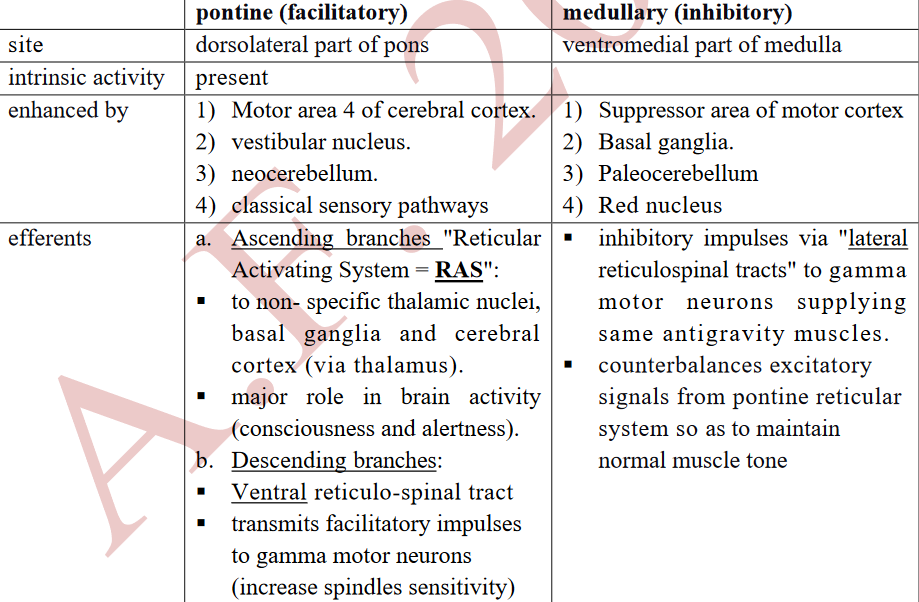
• large structure occupying core of brain stem.
• consists of areas of diffuse neurons of 2 types:
1. Sensory neurons:
▪ greater in number
▪ make multiple connections within reticular formation itself.
2. Motor neurons (reticular system):
▪ larger in size
▪ receive impulses from sensory neurons.
▪ divided into:
-
Equilibrium and vestibular apparatus(Responses to rotational acceleration)(A)
• SCCs on both sides transmit from cristae a continuous series of impulses averaging 200/s.
A. When head suddenly begins to rotate from left to right in horizontal plane
▪ horizontal SCC moves in same plane.
▪ endolymph is stationary because of its inertia: flows in a opposite direction (right to left).
▪ cupula is bent by endolymph and with projecting cilia.
▪ kinocilium of horizontal canals present towards utricle: bending stimulates hair cells
▪ frequency of impulses from right canal increased
▪ frequency of impulses from left canal decreased (cilia bent away)
▪ This unbalanced discharge give the sensation of rotation to right.
-
Equilibrium and vestibular apparatus(Responses to rotational acceleration) (B,C)
B. With continued rotation: (constant speed of rotation)
endolymph spins at same rate as canal and cupula swings back into upright position
C. When rotation is stopped:
▪ canals stop rotating: endolymph continues to flow for some time due to its
momentum in same direction 'of rotation i.e. from left to right,
▪ cupula is deformed in a direction opposite to that when rotation was first started
▪ discharge from left canal increases and from right side decreases.
▪ Imbalance in discharge →"vertigo": false sensation of rotation (from right to left side
▪ In seconds, endolymph stops moving and copula recoil to resting position.
▪ Discharge will return to tonic level and (vertigo) disappears.
N.B.: function of SCCs is detection of onset or stoppage of head rotation in one direction.
-
Neural pathway
• cell bodies of neurons in vestibular ganglion.
• vestibular nerve terminates in ipsilateral vestibular nucleus in medulla then to:
1. Reticular formation: sends fibres to spinal cord.
2. Spinal cord: fibers form vestibule-spinal tract
3. Cerebellum: flocculonodular lobe and dentate nucleus.
N.B.: Some fibers pass directly to cerebellum without synapsing in vestibular nucleus.
4. Motor nuclei of cranial nerves 3, 4 and 6: (by medial longitudinal bundle):
to extra-ocular muscles: eye movements help fixing objects in visual fields during rotation
5. Thalamus
-
Effects of stimulation of SCCs
1. Sensation of rotation: In same direction of rotation.
2. Maintenance of balance
• Increased muscle tone of ipsilateral side and a decrease on opposite side.
• Pathway: S C C s - vestibular nuclei - reticula nuclei - vestibulospinal
and reticulospinal tracts - motor neurons of spinal cord
3. Vertigo
• Def: false sensation of rotation that a person feels when rotation is stopped.
• in opposite direction to original rotation.
• Pathway: SCCs - vestibular n. or directly to flocculo- nodular lobe in cerebellum -
fastigial nucleus -opposite thalamus - Superior temporal gyrus (cortical centre for equilibrium).
• Causes:
1) Labyrinthitis: as irritation of SCCS by drugs e.g. streptomycin or toxicity of alcohol.
2) Menier's disease
3) motion sickness (excessive and repetitive labyrinthine stimulation) e.g. sea travel
-
Effects of stimulation of SCCs(continuous)
4. Post-rotatory reactions “past pointing test of Barany”:
• cortical voluntary movements to correct false sensation of vertigo
• aim: prevent falling of body in direction of false sensation of rotation.
• result: falling of body towards opposite side i.e. in direction of original rotation
5. Autonomic changes: nausea, vomiting, bradycardia, hypotension and sweating.
• Cause: stimulation of autonomic centers by impulses from vestibular apparatus
-
Effects of stimulation of SCCs(continuous 2.0)
6. Nystagmus:
• Def: jerky movements of eye observed at beginning and end of rotation.
• Aim: reflex to fix objects in visual field during rotation.
• Pathway from SCCs via medial longitudinal bundle (MLB) to stimulate 3,4,6
cranial nerves, supplying extra-ocular muscles.
• Center: in mid-brain sends impulses also via MLB
• Components:
a. Slow: opposite direction to rotation (vestibule-ocular reflex = VOR).
b. Fast: in same direction of rotation.
▪ direction of eye movement is identified by fast component:
- during rotation: in same direction
- when rotation is stopped: in opposite direction.
▪ Nystagmus is frequently horizontal, but maybe:
1. Vertical: head is rotated sidward
2. Rotatory: head is rotated forward
-
Effects of stimulation of SCCs(continuous 3.0)
Clinically :Nystagmus may be:
1) Physiological:
a) During head movement (Vestibulo ocular reflex "VOR"):
initiated by movement (present in blind)
b) Optokinetic: Initiated by visual impulses e.g. looking from a window of moving train.
2) Pathological:
a) Labyrinthine lesion: irritation of SCC, or vestibular nerve.
b) Menier's disease: increased endolymph pressure
c) Searching nystagmus: In defective vision, continuous movement of eye to focus image.
d) Neocerebellar syndrome.
-
Q. Vestibular functions
Function of utricle and saccule:
1. Maintenance of static equilibrium
1) In vertical position of head
- impulses from right and left utricles balance each other
- no sensation of malequilibrium.
2) When head tilted in space:
- calcium carbonate crystals fall by their weight.
- rate of discharge of impulses increases on that side but decreases on the other.
- Unbalanced discharge from bases of hair cells: malequilibrium
- equilibratory centers in brain stem and cerebellum stimulate appropriate
muscles to restore equilibrium.
-
Q. Vestibular functions(2.0)
2. Detection of linear acceleration
• Linear acceleration = acceleration in straight line:
may be horizontal e.g when a person stands in a bus which suddenly accelerates (sensed by utricle), or vertical e.g. when a lift starting to go up (sensed by saccule).
• When a bus suddenly accelerates:
- statoconia of utricle fall backwards due to its inertia and cilia are bent.
- stimulated group of hair cells cause discharge along vestibular nerve and
person feel falling backward.
- corrected by leaning forward to prevent him from falling.
- observed during running
-
functions of postural reflexes
1. Maintain body in the upright position.
2. Provide stable postural background for voluntary activity.
3. Restore the posture if it is lost, by restoring centre of gravity in relation to feet.
-
Types of postural reflexes
1. Static reflexes: sustained contraction of the musculature.
2. Phasic = dynamic reflexes: Involve transient movements
-
physiological role of different areas:
• Postural reflexes are integrated mainly at cortical centre: superior temporal gyrus.
• Impulses from eyes, vestibular apparatus, body and neck proprioceptors inform the centre about body’s orientation.
• The vestibular and neck information function in opposite direction:
a. When a person bends his neck:
- person senses malequilibrium by the vestibular apparatus
- impulses from the neck proprioceptors balance the vestibular information
- person feels that his head is only bent.
-
physiological role of different areas(2,0)
b. When body leans in one direction: impulses from the vestibular apparatus are not balanced by neck proprioceptors→ true sense of malequilibrium.
c. When the head bends forward:
Extension of the limbs by the vestibular reflexes is opposed by neck reflexes
which tend to relax them.
• Loss of any one alone will not cause the person to fall:
- If the vestibular apparatus is destroyed, equilibrium maintained by the eyes.
- During swimming, vestibular receptors are the only functional receptors due to:
a. Water pressure is equal all over the body.
b. Vision is difficult.
So, diving is difficult in disease of the vestibular apparatus.
• During closure of eyes, person keep equilibrium through proprioception: in Tabes dorsalis, when the person closes his eyes, he cannot keep his erect position (positive Romberg sign)
-
Motor Areas of Cerebral Cortex(Motor Cortex)
I. Primary motor area (motor area 4):occupies pre-central gyrus.
• highly excitable due o presence of highly excitable Betz cells. representation:
1) Crossed, unilateral (except for upper face i.e. forehead and eyes by both hemispheres):
each side controls skeletal muscles of opposite side
2) inverted: feet at top and face at bottom.
3 ) area of representation proportional to degree of complexity of movement:
areas for muscles of speech and hand are large while that representing trunk is small.
• Functions of motor area 4:
1) Control of fine discrete skilled movements especially done by distal parts e.g. fingers.
2) Facilitatory to stretch reflex and muscle tone
-
Motor Areas of Cerebral Cortex(Motor Cortex)(2.0)
II. Premotor Cortex (motor association area) (area 6and 8):
• Site: above Sylivian tissue in front of primary motor area
• Body representation: inverted
• no Betz cells, which makes it less excitable than area 4.
• Premotor cortex sends its signals either directly to primary motor cortex or to the basal ganglia, then to
the thalamus and finally to the primary cortex.
• Function:
1) initiates and controls pattern of complex coordinated gross movements involve many
muscles simultaneously to perform tasks as positioning so as hand can perform actions
2) selection of plans directed by external guidance as visual stimuli (mirror neurons).
3) It inhibits stretch reflex (area 4s).
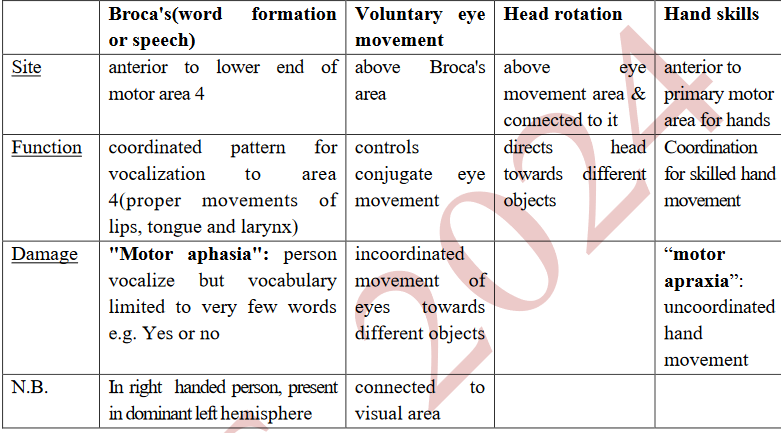
4) It contains specialized areas that control specific motor functions
-
Motor Areas of Cerebral Cortex(Motor Cortex)(3.0)
III. Supplementary Motor Area
• in front of area 4 and above premotor. project to other areas of motor cortex
• functions:
1) temporal planning of sequences: blood flow increases with complex movements
2) help premotor to provide positional stabilization
3) generates self initiated actions according to rehearsal (memory guided tasks)
4) involved in bimanual coordination
-
Connections of motor cortex(Afferent Fibres)
processed in motor cortex, basal ganglia and cerebellum. include:
1) Subcortical fibers from:
a. nearby areas, especially somatic sensory areas.
b. corresponding areas of motor cortex of other side.
2) From thalamus:
a. ventrobasal complex: Somatosensory fibres
b. ventroanterior and ventrolateral nuclei: from basal ganglia and cerebellum
c. non-specific thalamic nuclei: control excitability of cortex
-
Connections of motor cortex(Efferent)

to AHCs and motor cranial nuclei through:
I. Pyramidal System: 3 tracts:
-
Connections of motor cortex(Efferent)(2.0)
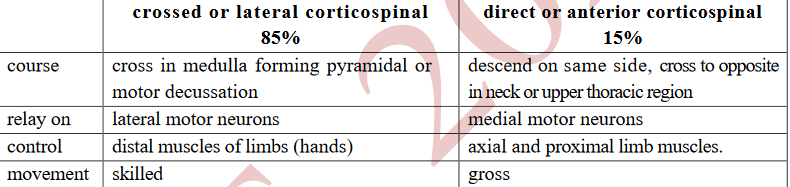
3.Corticospinal tracts: (approximately one million fibers)
• Origin:
a) 30%: primary motor area b) 30%: premotor areas
c) 40%: somatic sensory area.
• 3 % of fibers are large myelinated fibres, derived from large pyramidal Betz cell.
• Course:
- fibers descend in corona radiata then genu and posterior limb of internal capsule
- cerebral peduncle of midbrain and pons, and enter medulla. then
N.B.: Few fibres of anterior corticospinal tract do not cross providing bilateral innervation of
muscles of both sides moving simultaneously e.g. upper face, abdominal and respiratory
-
Connections of motor cortex(Efferent)(3.0)
Functions of Pyramidal System
1. complex fine skilled voluntary movements of fingers, toes and face.
2. facilitatory to strtch reflexe: section in monkeys causes hypotonia.
II. extrapyramidal system:
• Origin: Premotor area, basal ganglia, reticular formation, red and vestibular nuclei.
• Tracts:
1) Rubrospinal tract.
2) Reticulospinal tract.
3) Tectospinal tract.
4) Vestibulospinal tract.
5) Olivo spinal tract.
• Functions:
1) gross movements involving a group of muscles required for fixation.
2) Some fibres are facilitatory, others inhibitory to muscle tone
-
Clinical Links: plantar reflex (Center: S 1, 2)
• Stimulus: Scratching outer aspect of the sole by a blunt object.
• Normal response: Planter flexion of all toes.
• Abnormalresponse:"Babinski'ssign":
▪ doriflexion, of big toe and fanning of the other four toes.
▪ primitive response reappears following injury of pyramidal fibres.
▪ Other causes of the Babinski's sign
1) Deep sleep, deep coma and during anesthesia in adults.
2) infants blew one year, due to immaturity of pyramidal tract.
-
Clinical Links: plantar reflex(lesion of internal capsule)
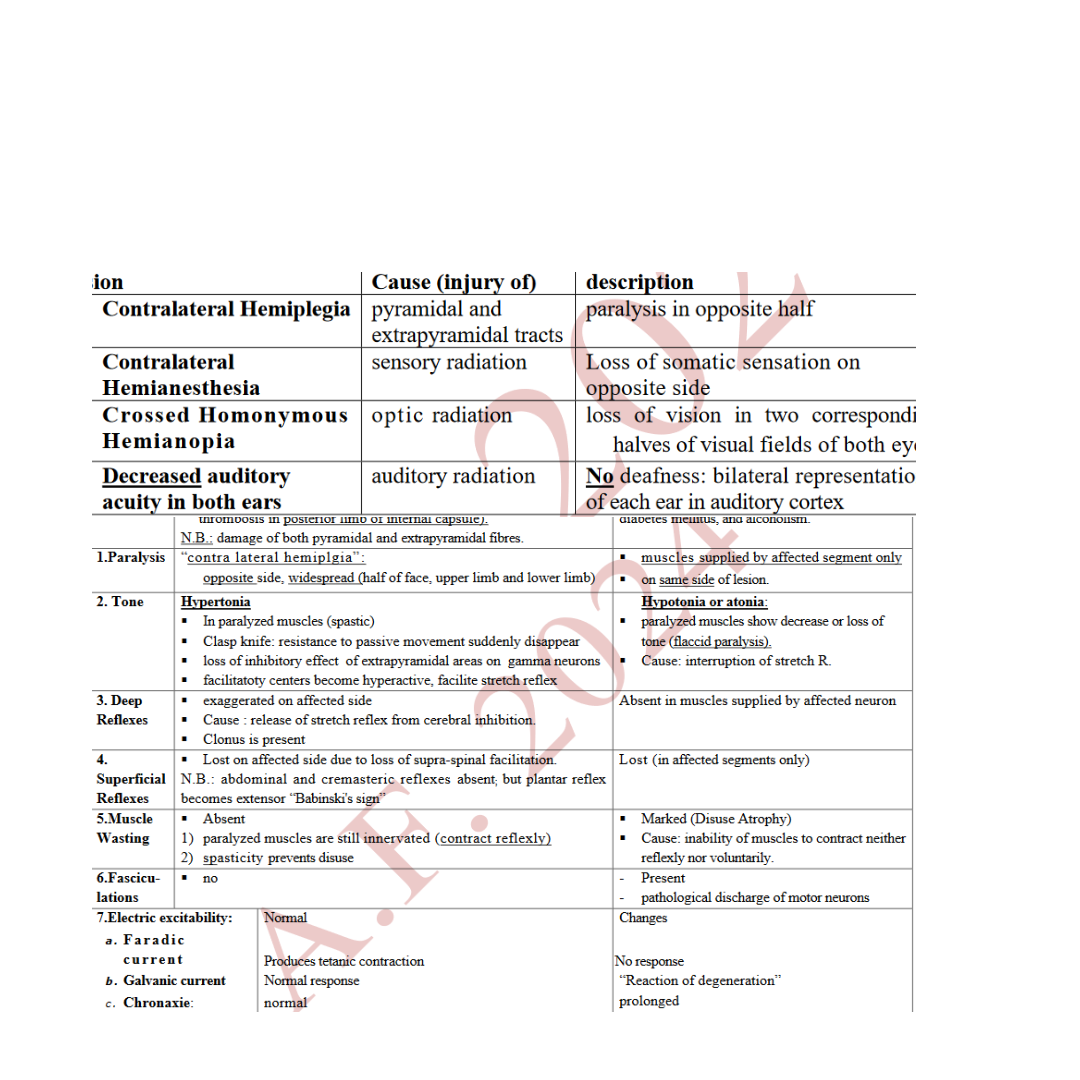
• cause: thrombosis or hemorrhage in lenticular artery affects posterior limb
• Fasciculations: visible spontaneous contractions of bundles of fibers in affected muscles
-
Basal Ganglia(Neuronal connections of basal ganglia)
I. Internal connections: caudate and putamen are regarded as receiving centre, while globus pallidus is discharging center:
1. Striato-pallidal projection: starts from neo-striatum to globus pallidus, secreting GABA
2. Stariato-nigral projection: from neostriatum pass to substantia nigra pars reticularis and secrete GABA.
3. Nigro –striatal projection: from substantia nigra pars compacta to striatum secreting dopamine may be excitatory (D1) or inhibitory(D2) according to receptor.
4. interneurons of striatum: Secretes acetyl choline, may be excitatory or inhibitory according to receptors
-
Basal Ganglia(Neuronal connections of basal ganglia)(2.0)
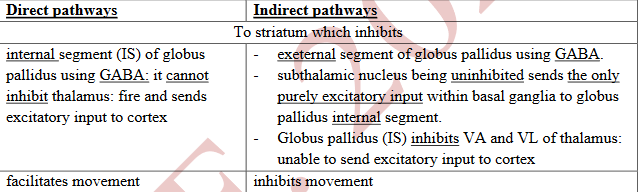
II. Cortical connections:
basal ganglia receive excitatory input from many cortical areas through neurotransmitter Glutamate to striatum then:
• balance of direct & indirect pathways is how basal ganglia involved in control of movement.
• N.B.: Dopamine secreted from substantia nigra to striatum:
- primarily through D1 (exciting) receptors participate in direct pathway
- D2 (inhibitory) receptors involved in indirect pathway.
- result: increase faciliatory inputs to motor regions.
-
Basal Ganglia(Neuronal connections of basal ganglia)(3.0)
III. Efferent pathway from basal ganglia :
• globus pallidus external segment projects to subthalamus and brain stem, secreting GABA:
From these areas fibers pass to reticular formation sends impulses via extrapyramidal tracts
(reticulospinal, vestibulospinal and rbrospinal tracts) to motor neurons of spinal cord.
• globus pallidus internal segment axons secrete GABA to thalamus (ventrolateral and ventro
anterior nuclei) and then to cortex.
-
Q. Functions of basal ganglia
1. Cognitive control of motor activity:
• thoughts and information stored in the memory are used for selection of an action, modifying
the timing (rapid or slow) and spatial dimensions (very small or very large letter)
• Proof: Neurons in BG discharge before movements begin. This observation led to the idea
that BG are involved in planning and programming of movement: the processes by which an
abstract thought is converted into voluntary action.
• Voluntary movements are stored as motor programs in the Motor cortices. BG facilitates the
selection of an appropriate motor program using the direct pathway and inhibits other
programs by inhibiting the cortex using the indirect pathway.
• Example: when one is subjected to a danger, he responds immediately by turning away from
it then begins to run.
-
Q. Functions of basal ganglia(2.0)
2. Help the corticospinal system in executing subconscious learned patterns of movement such as writing letters of the alphabet, cutting with scissors and some aspects of vocalization.
3. Initiation and regulation of the automatic associated movements of the body e.g. swinging of the arms while walking and facial expressions.
4. Globus pallidus is thought to be responsible for the posture taken by the body to perform a particular voluntary movement i.e. it locks the different parts of the body into a specific position so as to facilitate the fine movements of the hand.
5. mainly inhibitory to the muscle tone.
6. involved in control of behavior, at the level of motivation
7. have a role in saccadic eye movement
-
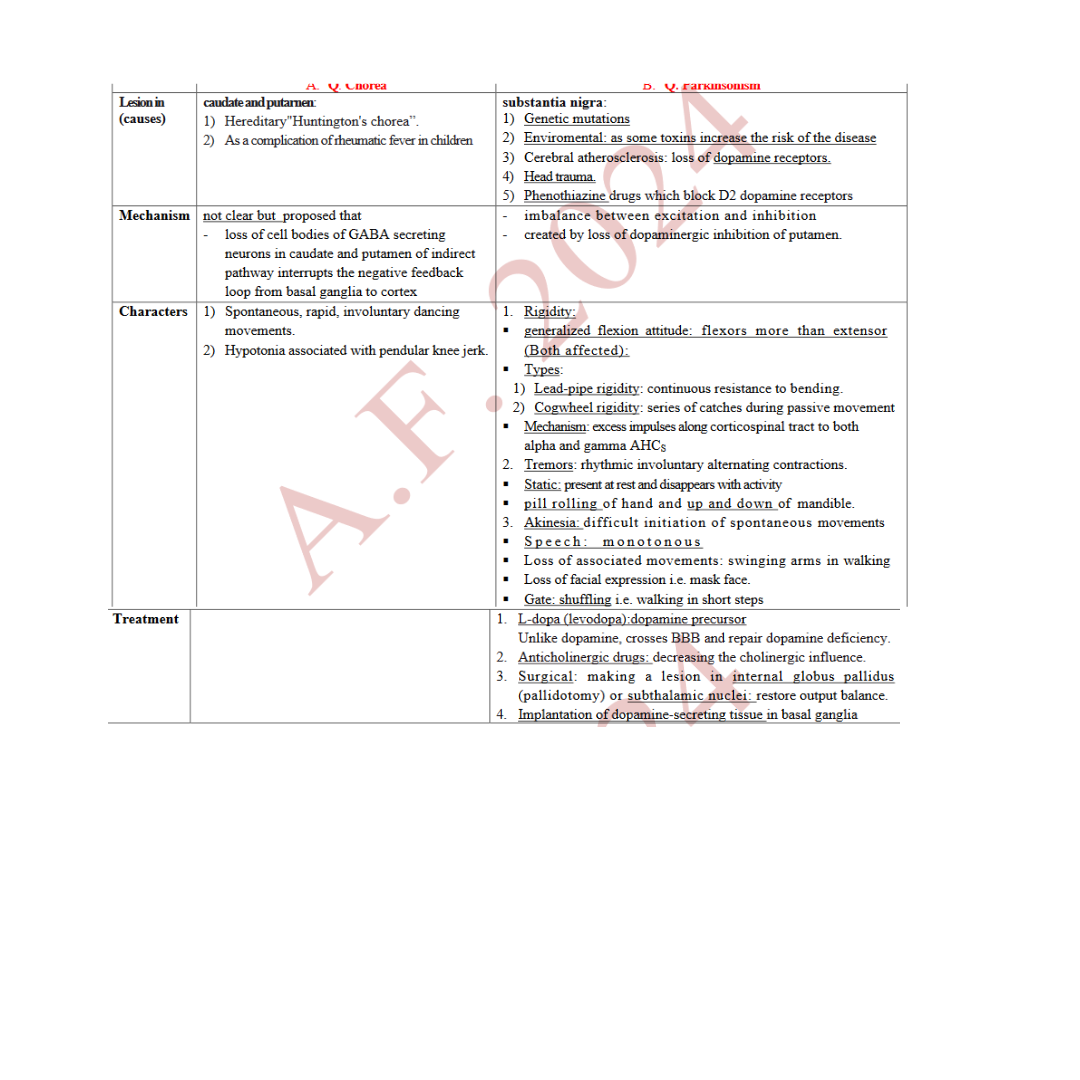
Diseases Of basal ganglia
-
Cerebellum(Functions)
was called silent area: its stimulation didn’t give sensation or movement.
A. in voluntary movements:
1. Servo- comparator function:
• motor cortex transmits same information to:
1) group of muscle to execute a particular movement
2) intermediate zone of cerebellum of opposite side (Cortico–Ponto-cerebellar)to inform about order given
• As muscles respond, muscle spindles transmit signals along spino-cerebellar tract.
• cerebellum compares performance with orders
• If not ideal, cerebellum sends corrective signals to motor cortex via (cerebello-thalamo-cortical)
• Climbing fibers from inferior olivary nucleus modulate sensitivity of Purkinje cells to granule cell excitation allowing deep nuclei to send error signals
2. braking effect: stop movements at precise intended point:
• assesses rate of movement, calculates time needed to reach intended point
• inhibitory impulses to motor cortex inhibit agonist and excite antagonist muscles.
-
Cerebellum(Functions)(2.0)
. Function in performance of rapid movements:
• cerebral cortex or brain stem 1st increases deep nuclear excitation to enhance movement,
• after few ms inhibitory signals from Purkinje cells arrive: stop muscle very rapidly
4. Planning and timing:
• cerebrocerebellum = lateral zones receive afferents from cortical association areas
• with other areas, plans movements: sends signals to motor area of cerebral cortex.
• Smooth progression from movement to next depends on lateral cerebellum: plans
next movement at time the present is occurring.
• also provides appropriate timing for each movement.
• lesion: inability to judge distance moved by particular part in given time
-
Cerebellum(Other functions)
1. in equilibrium:
• flocculondular lobe connected by a feedback circuit with vestibular apparatus.
• Inputs from vestibular apparatus used by cerebellum to send signals to brain stem (reticulospinal and vestibule spinal tracts): maintain equilibrium through changes in tone of axial and girdle muscles.
• Lesion: disturbance of equilibrium.
2. in muscle tone:
• neocerebellum is facilitatory while paleocerebellum inhibitory to stretch reflex.
• Its feedback time is longer than simple cord stretch reflex: prolongs effect.
• Helps in maintenance of posture
-
“Neocerebellar syndrome”
manifestations on same side of lesion because: each cerebellum hemisphere acts on ipsilateral muscles: dentato-rubrospinal tract is a double crossing tract:
- arises from dentate nucleus and passes to red nucleus of opposite side.
- From red nucleus of each side arises rubrospinal tract, which crosses to opposite side
and passes down brain stem to spinal cord.
• manifestations:
A. Ataxia: incoordination of movements in absence of paralysis:
due to errors in rate, range, force and direction of movement. damage of:
1. Cerebellar cortex: If only involved: abnormalities gradually disappear.
2. cerebellar nuclei: generalized permanent defects
-
“Neocerebellar syndrome”(others)
1. Disturbance of posture: head tilted &patient tends to fall to side of lesion
2. Gait: wide-based, unsteady drunken gait.
3. Slurred or scanning speech: due to defects of skilled movements
4. Dysmetria or past-pointing: voluntary movements are abnormal e.g. attempting to touch an object with a finger results in overshooting to one side or the other.
• tested by finger– nose test.
5. Intention tremor :
• Dysmetria, initiates correction action, but correction overshoot to the other side.
• finger oscillates back and forth causing tremors.
• Kinetic: absent at rest and appears during voluntary action
-
“Neocerebellar syndrome”(others)(2.0)
6. Rebound phenomenon = Inability to brake (to stop movement promptly):
• Test: Normally, flexion of forearm against resistance is quickly checked when
resistance force is suddenly broken off.
• in cerebellar disease: can not brake movement of limb: forearm flies backward.
7. Adiadokokinesia: inability to perform rapidly alternating opposite movements such as
repeated pronation and supination.
8. Decomposition of movements: Difficulty in actions involving simultaneous motion at more than one joint. (tested by heel-knee test).
9. Nystagmus: tremor of eye ball due to absence of damping function.
• When patient attempts to fix gaze on object to side of his head (Horizontal).
10. Hypotonia: due to marked decrease of facilitatory effect on stretch reflex.
• knee jerk is reduced and pendula
-
Electric activity of brain:
I. Evoked cortical responses:
• produced in cortex in response to stimulation of a receptor
• electrodes placed on surface of cerebral cortex of an anaesthetized animal
• consists of 2 positive waves separated by a negative wave
II . spontaneous potential “ Electro - encephalogrm ( E E G ) ” :
• setting: calm room at a comfortable temperature with complete physical and mental rest
• recorded by applying electrodes on scalp.
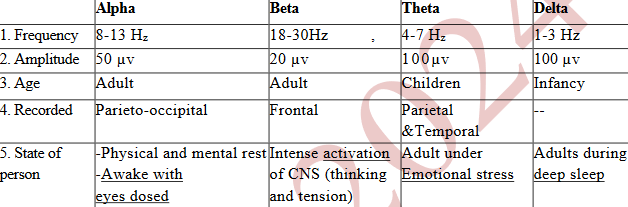
• Normal EEG waves:
N.B.
1. theta and delta waves in an adult during waking =abnormality.
2. hyperventilation decreases frequency of alpha waves, becomes theta or delta.
-
Electric activity of brain:(2.0)
• Desynchronization” or alpha block" arousal or alerting response":
o replacement of regular alpha rhythm with irregular low-voltage activity beta:
▪ eyes closed: synchronous discharge of many cerebral neurons produces alpha
▪ eyes opened: faster low voltage irregular beta waves
o called "arousal or alerting response" because it is correlated with alert state.
o Called "de-synchronization" because it represents breaking up of the synchronized neural activity necessary to produce regular waves
Clinical Uses of EEG:
1. Localizing brain tumors:
a. Large: blocks (reduces)electric activity from portion of cerebral cortex
b. Smaller: compresses and excites areas surrounding tumor: very high voltage.
2. Diagnosis of epilepsy
3. Diagnosis of sleep disorders.
4. Confirmation of brain death (flat EEG)
-
Arousal Mechanism "Wakefulness"
reticular activating system (RAS):
• function: Control brain activity, consciousness, alertness and electric activity
• composed of multi-synaptic pathway within reticular formation of brain stem.
• Some branches pass directly but most synapse in non-specific thalamic nuclei before passing to cortex.
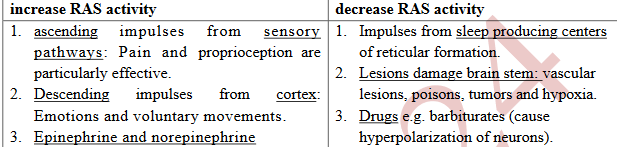
• Factors affecting activity of RAS:
-
SLEEP
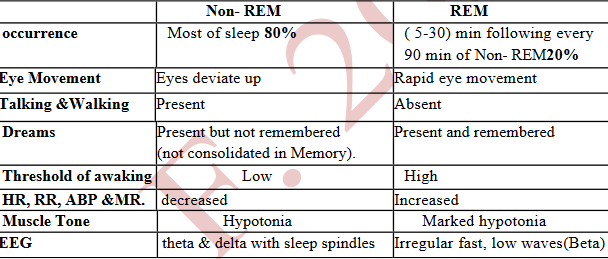
▪ loss of consciousness from which a person can be aroused by proper stimuli.
-
Distribution of sleep stages:
o young adult enters NREM sleep:
▪ passes through stage 1 and 2 then spends 70-100 minutes in stages 3 and 4.
o then a REM period follows (four to six periods per night).
o cycle repeated at intervals of 90 min throughout the night.
o percentage of REM sleep falls as we approach old age
-
Sleep disorders
1. Insomnia: insufficient sleep due to psychological factors (anxiety) or analeptics (coffee)
2. Somnambulism: "sleep walking”: eyes opened, and when awaken can not remember (More common in male children).
3. Narcolepsy: Irresistible sleep during daytime activities (Starts with REM sleep)
4. Sleep apnea: Caused by obstruction of airways during sleep.
5. REM behavior disorder: Hypotonia fails to occur: patients act out their dreams (jump)
-
Thalamus(Functions)
1. relay station for all types of sensation (except olfaction): on their way to their respective centers in the cerebral cortex.
2. relays signals of motor function from basal ganglia and cerebellum to motor areas.
3. relays autonomic signals and those related to emotional reactions through their ways to the hypothalamus and limbic system.
4. role in coding, storing and recalling memories.
5. excitability of cortex by Impulses from non-specific thalamic nuclei.
-
Thalamus(Thalamic Syndrome)
• Cause: thrombosis of arterial supply of thalamus,
• presentation:
1) Loss of all sensation on opposite side.
2) Sensory ataxia similar to that seen in tabes dorsalis.
3) 2ry hyperalgesia: pain threshold increased but pain is prolonged, severe.
4) Emotional disturbance
-
Hypothalamus(Functions)
1. Autonomic functions
o anterior nuclei produces parasympathetic effects,
o posterior dorsomedial and lateral nuclei produces sympathetic effects.
2. Food intake regulation: balance between two centers:
a. feeding centre: in lateral hypothalamus (hunger).
b. satiety centre: in ventromedial nucleus (anorexia).
3. Control of sexual function: influence anterior pituitary
4. Body water regulation thirst centre in supra-optic region
5. Temperature regulation
a. responses to cold (Cusanecus VC, shivering) by posterior hypothalamus.
b. Heat losing (Cutaneuos VD & sweating) by anterior hypothalmus
-
Hypothalamus(Functions)(2.0)
6. Behavioral function (part of limbic system):
o concerned with affective nature of sensation.
o certain areas pleases while others cause unpleasant response (terror, pain, fear)
7. Defensive reaction (part of limbic system): involved in rage and fear.
8. Relation to circadian rhythm: adjusts bodily rhythms to the 24- hour light-dark cycle.
9. Neuro-endocrine function
a. posterior pituitary: synthesis of ADH and oxytocin.
b. Control of anterior pituitary: releasing and inhibiting hormones
10. Wakefulness and sleep
a. part of RAS: initiates and maintains wakefulness.
b. anterior hypothalamus promotes sleep.
-
Hypothalamus(Speech)
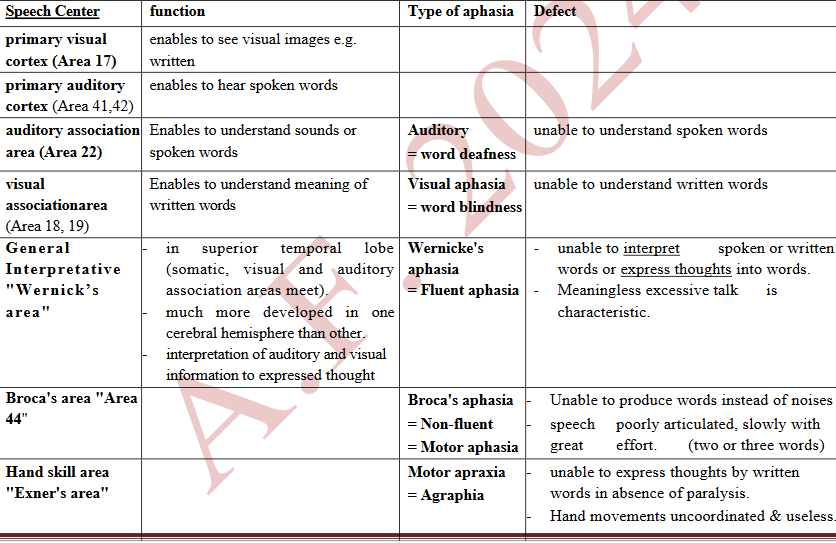
Def:Understanding spoken and printed words, besides expressing ideas in speech and written words.
▪ highest function of nervous system.
Aphasia: abnormalities of speech (language) functions due to injury of speech (language) centers.
• usually follows thrombosis or embolism of cerebral vessels

