gene therapy and its potential in treating cystic fibrosis

Meyers 2:00
R01
GENE THERAPY AND ITS POTENTIAL IN TREATING CYSTIC FIBROSIS
Sean O’Connor (
SRO13@pitt.edu
), Kevin Hulbert ( KPH12@pitt.edu
)
Abstract- Genetic Engineering has been changing the world of research and medicine since the late 1900’s. This paper is about the ever-changing field of gene therapy and its potential to cure cystic fibrosis. It will describe the complex processes and transformations involved in the gene therapy treatments of cystic fibrosis. This research done on cystic fibrosis is the best model for gene therapy treatment of other illnesses (Wagner 203). This therapy raises ethical issues with social and political ramifications. These ethical concerns will be discussed in the paper.
Current methods of somatic gene therapy transfer involve the processes of viral and non-viral injections into the cells of the human body. The viral method, using viruses as vectors, has become the more successful of the two
(Dhillon 1). Their viral transformation and how they work in treatment of CF will be discussed in more detail in this paper. Understanding the cystic fibrosis trans-membrane conductance regulator gene (CFTR) is a major aspect in the treatment of CF. This gene is crucial in regulating proteins that secrete chloride ions. When mutated, defective protein processing and production may ensue, as well as defective chloride secretion. This may cause a buildup of protein in the lungs and subsequent fatal lung disease. As a target for gene therapy development, CF is one of the most extensively researched genetic diseases (Wagner 203). Unfortunately, the progress of this gene therapy research has been slowed because of the complexity of multi-genetic diseases (Bosone
1). Research is still in progress
Key Words - Gene Therapy, Cystic Fibrosis, Genetic
Engineering, Ethics, Cystic Fibrosis Trans-membrane
Conductance Regulator, Bioengineering, Animal Research,
Viral Transformation
T HE G ENETIC D ISEASE : C YSTIC F IBROSIS
Before gene therapy, permanent cures for some of the deadliest diseases were hopeless and unlikely to ever occur.
Now with research in gene therapy, these diseases have the opportunity to be permanently cured. Cystic Fibrosis is a genetic disease that is well known and has caused a lot of suffering and death in the United States and around the world. It is fairly common disease, affecting 1 in 2500
Caucasian newborns [1].
Cystic fibrosis is the result in a variety of genetic mutations of the Cystic Fibrosis Trans-membrane
Conductance Regulator gene (CFTR) in the human genome.
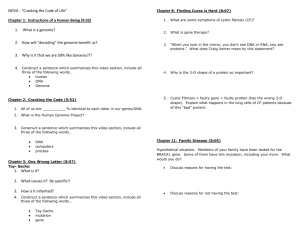
The CFTR gene is found in region q31.2 on the long (q) arm of human chromosome 7.
CHROMOSOME 7
S HOWS THE LOCATION OF THE CFTR G ENE [2]
Two scientists, Collins and Tsui, discovered the location of the gene at Yale University in 1989. When functioning properly, CFTR codes for the production of a protein made up of 1480 amino acids [2]. This protein product is a channel for chloride ions and is located in the epithelial cells lining the lungs, liver, pancreas, reproductive tracts, intestines, and skin. For this gene to fire and secrete Cl- ions, phosphorylation must occur (PO43- ion). The exact structure of the CFTR protein product has not been determined through research but after being compared to other transporter proteins, it is the only one with a fifth regulatory domain.
The vast majority of Cystic Fibrosis cases are due to a deletion mutation of three base pairs in the gene. This deletion causes loss of the amino acid phenylalanine located at position 508 in the protein; therefore, this mutation is referred to as delta F508. The protein will not fold properly and will eventually degrade. Also found is that a mutation in the S341A position can alter the affinity and voltage dependence of the protein, vital to blocking and opening the channels of CFTR [3]. This change in affinity and voltage may cause less phosphorylation, rendering the CFTR protein almost useless. With this being said, mucus and bacteria may build up causing lung disease. The lack of chlorine in the cells of the pulmonary tract, when one has CF, inhibits airway surface liquid (mediated by Cl-) to adjust, in turn preventing periciliar liquid layer (PCL) to from at a correct height [4]. This PCL is what “lubricates” airways allowing mucus and bacteria to pass through without clotting/blocking the airway. Without this CF becomes one of the deadliest diseases on the planet.
University of Pittsburgh
Swanson School of Engineering
1 March 1, 2012
Sean O’Connor
Kevin Hulbert
Treatment of the Disease before Gene Therapy
Before gene therapy research, there seemed to be no hope of curing cystic fibrosis and those who are unfortunately diagnosed with it were cursed to live a shortened life filled with pain and infection. The build of mucous in respiratory canals often caused infection and made it very difficult to breathe. Many patients end up with continuous hospitalizations, endless antibiotics, and enzyme supplements. In the 1990’s, it was predicted that babies diagnosed with cystic fibrosis could live up to about 40 years old [5]. Many antibiotic drugs have been developed to help such as ticarcillin, piperacillin, and ceftazidime. The use of inhaled antibiotics such as coliston has proved to be successful in improving pulmonary function in the past.
However there are usually cons involved with most medical treatments. The development of multidrug resistant microorganisms rises everyday and continues to cause problems in treating cystic fibrosis. This occurs because this treatment method involves large amounts of intakes of antibiotics making it easier to become resistant.
Different methods of physical therapy and exercise have been used to try and clear obstructed airways in patients.
Patients are often put in positions that allow for drainage of the mucus formed in the lungs while a percussion machine pats the back or chest to dislodge mucus from the walls of the airways. Medications such as bronchodilators, mucolytics, and decongestants are available on the market but can prove to be costly [5]. The patient is encouraged to exercise consistently because it also helps clear the lungs.
Children often need to be treated by their family members but with age, may be able to use these techniques on their own.
Another method used is lung transplantation. This is a much more sever method that is very expensive and is hard to come by because of the large need for it. It is suggested mainly for patients that experience severe respiratory failure.
This treatment, if successful, allows for normal CFTR proteins to be formed but normal transplant complications are always possibility. All of the older methods can help prolong the inevitable among patients but over the years, they become very costly and do not provide a permanent solution. An increase in research in gene therapy and the development of higher technologies continues to allow for a promising future. If gene therapy is perfected in treating cystic fibrosis, then a truly permanent treatment may finally be possible.
G ENE T HERAPY AND THE E NGINEERING
T
ECHNOLOGY
I
NVOLVED
Genetic engineering research has and continues to put a lot of work into developing gene therapy and the technology involved with it. Gene therapy is a process involved in genetic engineering that allows for modification of genes internally and externally to treat diseases. The attention of cystic fibrosis is mainly on the respiratory tracts because it proves to be the most problematic. The defect gene for
CFTR is cloned and modified. Chloride transport was made possible and this new product is called wild-type CFTR. The process of cloning the DNA is made easier with real-time quantitative PCR (Q-PCR). PCR is a polymerase chain reaction and its products can now be measured in real time.
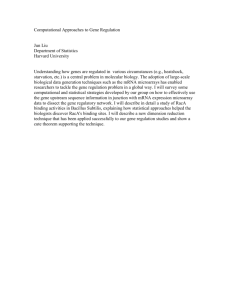
A fluorescent signal is generated from the reaction and is captured by instruments such as TaqMan Probes, Molecular beacons, and SYBR intercalating green dyes. The probes are capable of determining the expression level of specific allele in comparison to the allele one nucleotide away. It measures mRNA expression, DNA copy numbers, transgene copy number and expression analysis, allele discrimination, and viral titers [6]. This technology has only recently become a useful factor in gene therapy and provides for the opportunity of using less expensive instruments. Q-PCR generates exponentially a graph of DNA copies until it plateaus off. The measurements that are collected allow for knowledge of exact placement and expression of the CFTR gene.
PCR GRAPH RESULTS
S HOWS THE E XPONENTIAL R ESULTS C OLLECTED FROM R ESEARCH [6]
External strategies prove harder for the cells of the lungs so an in-vivo process is needed. Vectors must be applied directly to the target cells for in-vivo methods. Vectors are modes of transport for the newly modified healthy genes.
Many different vectors show promise in being successfully taken in by humans, but viral vectors show the most promise. There are many different types of viral vectors, each different from the other in regards to DNA copying, administration into the subject, and how it bonds to the
CFTR. There are retroviruses, adenoviruses, lentiviruses, adeno-associated viruses, and Nano-engineered substances.
Adenoviral and retroviral vectors have been more successful when tested than other forms of viral vectors. When the viral vector route is taken, the virus DNA originally starts in the form of a plasmid, a ring of DNA. The goal is to get this
2
Sean O’Connor
Kevin Hulbert virus to deliver the healthy CFTR to a target cell but not to replicate or form more viruses. The replication gene and the capsid gene are removed from the virus. A capsid is a shell that surrounds the virus. The removal of these genes can be done recombinant DNA (rDNA) technology. Restriction enzymes are used to cleave the DNA at a specific site. This leaves two “sticky” ends on the plasmid. The CFTR gene is then inserted into the plasmid and is joined by a DNA ligase enzyme [7]. Once the vector has been built. The vector is placed into a packaging cell line that contains a helper virus and the replication and capsid genes that were removed. This packaging cell line combines the elements with the vector and aids in replicating the virus with the new plasmid in it.
Cells become full of the virus and they burst. This is when they are collected into a pure liquid solution of viruses. The new virus vector is then put into the infected unhealthy cells of the lungs. Methods of injection into cells for gene therapy include heat shock, electroporation, viruses (produced by above description), and a gene gun. Heat shock involves heating the host cells suddenly causing its membrane to become permeable enough for the new DNA to pass through. Electroporation involves a similar process where electric shock allows for increased permeability. A gene gun fires gold particles coated with foreign DNA segments. The virus or injected DNA infects the cells and the new DNA becomes integrated into a specific location on chromosome
19. This new DNA successfully codes for the correct mRNA to produce healthy CFTR cells. This is the general way a viral vector works, but adenoviral and retroviral vectors work slightly differently.
Adenoviruses are medium sized icosahedral viruses composed of a nucleocapsid and a double-stranded DNA genome [8]. A nucleocapsid is a viral sac that is made up of a nucleic acid and protein coat. The nucleic acid is what holds the DNA. Adenoviruses represent the largest nonenveloped virus, as it is just small enough to be transmitted through the endosome of the epithelial. These viruses are transmitted into the subject through respiratory droplets or through fecal routes. Once inside the cell the adenovirus attaches onto the coxsackie-adenovirus receptor (CAR) on the mutated cell’s surface through one of its sharp fibres [8].
The CAR is a protein that acts like a hand, grabbing the adenovirus and pull it into the epithelial cells of the mutated gene. After it passes through the surface of the host cell, the virus lets the DNA free into the nucleus of the host. This process has two parts to it. The first interaction with the host involves the fibre of the virus binding to the cox-sackie receptor of the host. This first process is fairly simple, but the second process is far more complex. Once the adenovirus is bonded to the CAR, a penton base protein in the adenovirus binds to an integrin molecule, which acts as a co-receptor to the CAR. This binding causes internalization of the virus into the host cell. This binding stimulates the cell to signal and causes actin polymerization to occur, in turn allowing the virus to enter an endosome of the host cell.
Actin polymerization is the process of combining DNA monomers into a polymer so the actin protein in the host can move the virus into the cell endosome. After this the endosome can acidify and break apart releasing the adenovirus into the cytoplasm of the host. The virus is then transported to the nuclear pore complex (openings in the nucleus), where the adenovirus can break open allowing the
DNA of the virus to finally enter the nucleus of the mutated cell [8].
There are some disadvantages to gene therapy. Cost is one of the major problems. This kind of treatment will become expensive if the patient needs to keep receiving the treatment. The issue of response to the treatment is another factor. The more times the treatment is administered to try and achieve long-term affects, the more likely the body is to become immune to the treatment. Current treatments of cystic fibrosis have not proven to be permanent. The affects will work for a few days but then the cells will turn back to their incorrect coding of CFTR. The target cells have been debated a lot and determination of the exact “parent” cells has not occurred. Studies have shown that some patients have defections in 100% of their CFTR genes, and other patients have defections in as little as six percent [9]. The natural response of the body when foreign material enters it is to fight it and either kill or remove it. Infecting cells with the new foreign DNA in the vectors may cause the patients body to produce an immune response against it causing the patient to become ill. Using viruses as vectors also creates a risky situation because there is always the chance that the virus will regain its old ability to spread disease in the patient. The new DNA may not make it to the right cells that need to be altered and if it does make it to the right cell, the vector DNA might not be placed correctly into the incorrect
DNA. There are barriers in the lung that make it more difficult to get the new DNA to the correct lung cells in the patient. The mucocillary clearance defense system can be slowed down with new drugs such as rhDNase [1]. Finding a safe method to apply this treatment to the patients mucus filled lungs has been the main challenge in gene therapy being affective for good. A lot of research has been going on in current and recent years to help find the best way to administer the healthy gene into the cell and once that occurs, making the cure permanent. Both are detrimental to making gene therapy a trusted cure for diseases, but advances are being made.
R ECENT AND C URRENT R ESEARCH
Researchers have been working very hard to find out a way to make gene therapy successful. If it were to be found successful, a plethora of deadly diseases all across the world would have a great opportunity to be cured. Diseases such as: AIDS, cancer, Alzheimer’s might be things of the past.
That is why a lot of research goes into gene therapy. In
1989, after it was found that the CFTR gene was the cause of cystic fibrosis [5], gene therapy research began on a large
3
Sean O’Connor
Kevin Hulbert scale. Was it just a coincidence? Or was the fact that a mutated CFTR gene was found to be the culprit of the disease, which resulted in the first trials of gene therapy on humans to occur that same year. In 1989, Dr. Steven A.
Rosenberg administered the first trial of gene therapy to be done on a human [9]. The Rosenberg trial involved introducing a retrovirus into five patients with melanoma.
This trial didn’t involve cystic fibrosis, yet it was a huge step in curing the disease, as the number of trials in administering gene therapy rose exponentially. “This study demonstrated the feasibility of using retroviral gene transduction in humans and set the stage for further studies” [9]. Since the first study in 1989, almost 1,000 clinical gene therapy trials have been completed or have been approved by doctors and researchers all over the world. In 1990, another major gene therapy trial ensued. The first therapeutic gene therapy trial was allowed to be performed. Up until 2004, there had been gene therapy trials in 24 different countries, with the United
States administering the majority of them. These trials used many different vectors to send the healthy genes into the cells of subjects. The majority of these being viral vectors
(70%). Of all trials, 28% of trials involved retroviral vectors and 26% involved adenoviruses [9]. Non-viral vectors are used because they are less dangerous to the subject than viral vectors, yet aren’t as effective. Many diseases had been tested upon as well; cancer being the most common. Ten percent of the trials were involved in monogenetic diseases, with one-third of those being cystic fibrosis [9].
Adenoviral Vectors
In 1995 a clinical trial involving adenoviral vectors in treating cystic fibrosis was directed on 12 patients with cystic fibrosis [10]. The adenovirus was inserted into the right nostril first, then the left nostril of the subjects. The adenovirus was administered in the epithelial of the nostrils with increasing dosage. After about an hour it was found that only 58% of the adenovirus solution remained in the nose.
After the trials statistics showed that there was no real potential difference in the epithelial of the nostril between the four cohorts of subjects. The fourth cohort (most dosage), didn’t differ much at all from the first cohort (least dosage). The researchers at the end of the study concluded that the gene transfer through adenoviruses in the nostrils was not efficient [10]. Chloride ion transport was not increased in the CFTR, only inflammation was. All in all it was not a successful test, but in 1999, a test using a similar transport method was successful.
At Stanford University researchers began a clinical trial in which adeno-associated viruses were administered to the patient via aerosols [11]. These aerosols were inserted through the nostrils of the patients. Including inflammation of the lungs in patients with CF, the sinuses are affected negatively as well. When the adeno-associated virus was inserted into the nostrils, it was found that there was a
“significant reduction in inflammation” [11]. This study didn’t show gene transfer would be successful in the epithelial of the lungs and cells, but it was a big confidence booster, that would help pave the way for more CF gene therapy research in the coming years.
Cationic Liposomes
Current research falls heavily on new ways of delivering the genes efficiently. Whit regards to efficiency, a lot of research has turned to developing viral psuedotyping, a new generation of cationic liposomes, and the use of non-viral vectors with a powerful transfection levels such as the
Sendai virus [1]. Cationic liposome research involves mixing cationic lipids with cholesterol and dioleoylphosphatidyl-ethanolamine. These are bonded to
DNA electrostatically and are allowed to interact and pass through cell membranes. Research has proven that this method has shown transfection in the lungs epithelial cells of mice. This was tried in a human trial by nasal perfusion and resulted in partial correction of nasal differences but the patient did succumb to a fever. Other trials had similar results and modifications of the cationic liposomes are needed. Some ideas for modification include reducing nonessential CpG to reduce inflammatory response by patients
[12]. Research on extending the length of time of the effects is also crucial because the main goal is for this treatment to cure cystic fibrosis permanently. Adenovirus vectors have proven to be the most efficient with this part of the process.
The latest of developments in adenovirus vectors has shown high transgenic effects from treatment lasting up to 15 weeks in mice [12]. This is good progress but is still a long step from the intended goal.
Non-epithelial Cells
Research on treating alternative non-epithelial cells is also currently in progress. The CFTR defect in immune cells can prevent them from clearing pathogens. Because of this defect, patients become considerably more vulnerable to pathogens in the air that may cause illness. Correcting the defect in these cells would prove to be effective and beneficial to the patient. Research in mutated, CFTR lacking, mice has risen questions about whether or not inflammatory signals are due to mutated epithelial cells or deficient lymphocytes [12]. Correcting CFTR can cause the lymphocyte channel to work properly again. It is important to protect the effectiveness of the immune system in a patient with cystic fibrosis because they are consistently faced with mucus build up and respiratory infection. Studies on cystic fibrosis lung-transplant recipients have shown that they exhibit a larger decline in health than those without the transplant. Correcting the CFTR in non-epithelial cells has been relatively unexplored but offers potential in aiding against treating patients with cystic fibrosis.
4
Sean O’Connor
Kevin Hulbert
E
THICAL
C
ONSIDERATIONS
Genetic Engineering is a big part of the medical field. The medical field has always been limited due to ethics and laws passed by the government. Many of the considerations that go into aspects of the medical field apply to genetic engineering as well. It is important to realize that not everyone agrees with genetic engineering, specifically when it comes to altering the DNA of a fetus. The government has passed laws on any time of germ line therapy in humans because the alterations would affect future outcomes of many generations [13]. The government has not chose to prevent somatic gene therapy to treat disease so this gives research the potential to improve. Genetic engineering is a fearful advancement because of its risk and its potential.
Many fear that the excitement of the potential of this type of treatment has led to research trials that may have been too risky. Researchers are not sure of what the best way to transfer the correct genes is and it will take many years of trials to determine it. Researchers have to make sure of all there research and answer many questions before being allowed access to human trials. Many people hold the belief that we should be fated to what we were born with and that it is unnatural to try and alter nature’s course. Some find that going against the natural way of things is unethical and that people should not try and play “god”. People are afraid that instead of gene therapy being used to cure diseases that the rich will take it to the extreme and try to purchase “super” children. Many are in favor of gene therapy as long as it is restricted to curing diseases that causes pain and suffering to the families and the public [13]. It is normal for people to want the medical field to continue to advance so that all disease will be cured. It is also understandable that there are real fears among people about growing technologies in the medical field. If the wrong people in government decided to change the laws, then all around the world, super-humans will begin to rise. Many people also worry about insurance companies using genetic testing to determine who gets covered and who does not get covered [13]. This is a real concern because insurance companies could potentially condemn those with “bad” genes to poor medical care and the inability to afford medical treatment.
Many religious people say that it is unholy to alter the genes that god gave a person. It is a sin and is wrongful to alter nature with new genetic engineering technology. Polls that have been taken show that 58% of people disagree with the religious view on gene therapy [13]. It is understandable to take into account people’s religious beliefs but when it comes to passing laws against it, their beliefs cannot influence the decision because of separation of church and state. Who gets to decide what diseases are worthy of being treated by gene therapy? This is a common question brought up because it concerns ethics. It is tough to decide specifically what is a suitable disease for gene therapy because restricting another disease may cause a person pain and suffering when there is the potential to cure that person.
It is important for the citizens of the world to stay active in the debates on gene therapy and to voice their opinions because it is not right for any one man to make the decisions concerning gene therapy.
Gene therapy has not been perfected so it can be unpredictable at times. Using treatment on humans where there is the potential of viral vectors turning to their natural viral tendencies is unethical because it could cause the patient to become even sicker with allergic reaction or inflammation. It has become one of the main goals of gene therapy researchers to perfect making the transfer of healthy genes safe and consistent. People believe that treating patients with gene therapy may be unethical because of all the risks involved [13]. In the medical field, there are always risks. Progress has been made over the years because risks have been taken. It is important to take the right risks. After a considerable amount of research has been conducted and the animal trials have been successful, human trials are necessary for the advancement of the medical field. People have always dreamed about a world without cancer, aids, and other painful diseases such as cystic fibrosis. The same risks are often involved in other medical procedures. A lung transplant to try and treat cystic fibrosis has many of the same risks as gene therapy if not more risks. They both share the possibility of rejection by the immune system and inflammation. The lung transplant will be very expensive and will require many treatments to make sure that everything is working correctly and that the body is accepting it. There is always the risk that the new DNA will make its way to the egg and sperm cells. This causes a lot of concern because that would affect future generations. There has been know indication of egg or sperm cells being affected in conducted research trials [13]. Gene therapy, when perfected, will involve one treatment that may be painless and will cure cystic fibrosis for the rest of the patient’s life.
L OOKING TO THE F UTURE
Genetic engineering has a very promising future. Research continues to be well funded and new breakthroughs and positive results are imminent. Using gene therapy to treat diseases and cancers will transform the medical field and the world. If scientists and engineers can perfect the vector methods used to administer healthy CFTR genes into a patients cell, cystic fibrosis can be cured. The gene gun and aerosol injection are prominent technologies for delivering the vector but better methods need to be found. New ideas to aid in the treatment of cystic fibrosis are being developed such as treating non-epithelial affected cells and cationic liposomes. Developing newer and more efficient technology for delivery is essential in the progress of the therapy.
Research needs to be geared towards finding away for cells to sustain the effects of gene therapy treatment permanently
5
Sean O’Connor
Kevin Hulbert or for long periods of time. Fifteen weeks of positive results is nice but is nowhere near as good as giving a patient suffering with cystic fibrosis a lifetime without the disease.
Overcoming the barriers provided by the immune response is also one of the tougher tasks. The body is always going to try and fight foreign substances that enter it. This significantly increases the risks of gene therapy and slows down trials and research. Many suffer from the disease and many would like to see it as well as other diseases eliminated from the world. Gene therapy faces many struggles such as religious beliefs, government laws and ethics, and the public fear of the its potential to play the role of god. New technology, new treatments, and new ideas scare a lot of the general public. Majorities of people do not like change even if it is for the greater good. More human and animal trials need to be conducted and the government needs to continue to supply sufficient funding. It is clear that since the discovery of the human genome the future of medicine would be involved with it. Gene therapy is the solution that mankind has been waiting for many years and its technology and processes need to be fully supported by the public in order for it to be successful.
R EFERENCES
[1] Davies, Jane C and Geddes, Duncan M. (July 6, 2001). “Gene Therapy for Cystic Fibrosis”. The Journal of Gene Medicine . [Online Article].
Available: http://onlinelibrary.wiley.com/doi/10.1002/jgm.200/full
[2] “CFTR: The Gene Associated with Cystic Fibrosis”. The US
Department of Energy, Biological, and Environmental Research. September
12, 2003. [Online Site]. Available: http://www.ornl.gov/sci/techresources/Human_Genome/posters/chromosom e/cftr.shtml
[3] Gadsby, David and Angus Nairn. “Control of CFTR Channel Gating by
Phosphorylation and Nucleotide Hydrolysis”. Physiological Reviews.
New
York, New York. Vol. 79. January, 1999. [Online Article]. Available: http://physrev.physiology.org/content/79/1/S77.full.pdf
[4] Boucher, RC. “New Concepts of the Pathogenesis of Cystic Fibrosis
Lung Disease”.
European Respiratory Journal.
January 1, 2004. Chapel
Hill, USA. [Online article]. Available: http://www.ersj.org.uk/content/23/1/146.full
[5] Zoidis, John D. “Treatment Strategies for Patients with CF”. RT
Magazine . June/July, 2012. [Online article]. Available: http://www.rtmagazine.com/issues/articles/2002-06_04.asp
[6] Ginzinger, David G. (Dec 10, 2001) “Gene quantification using realtime quantitative PCR: An emerging technology hits the mainstream”.
ISEH . [Online Article]. Available: http://www.sciencedirect.com/science/article/pii/S0301472X02008068
[7] Rao, Sridhar. “Genetic Engineering / Recombinant DNA Technology”.
JJMMC . [Online PDF]. http://www.microrao.com/micronotes/genetic_engineering.pdf
Available:
[8] Wagner, John A and Phyllis Gardner. “Towards Cystic Fibrosis Gene
Therapy”.
Annual Reviews.
Copyright 1997: 203-213. [Online Article].
Available: http://cmgm.stanford.edu/biochem118/Papers/Gene_Therapy/cystic_fibrosi s_gene.pdf
[9] Edelstein, Michael L, Abedi, Mohammed R, Wixon, Jo, and Edelstein,
Richard M. (May 26, 2004). “Gene therapy clinical trials worldwide 1989-
2004- an overview”. The Journal of Gene Medicine . [Online Article].
Available: http://onlinelibrary.wiley.com/doi/10.1002/jgm.619/full
[10] Knowles, Michael. “A Controlled Study of Adeno-Viral Vector
Medicated Gene Transfer In the Nasal Epithelium of Patients with Cystic
Fibrosis”.
The New England Journal of Medicine. September 28, 1995.
[Online article]. Available: http://www.nejm.org/doi/full/10.1056/NEJM199509283331302#t=article
[11] Tanne, Janice Hopkins. “US Trial of Gene Therapy for Cystic
Fibrosis”.
British Medical Journal. New York. April 24, 1999. [Online article]. Available: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1115504/
[12] Mueller, Christian and Terrence R Flotte. “Gene Therapy for Cystic
Fibrosis”. Human Press Inc. July 4, 2008. [Online PDF]. Available: http://www.springerlink.com/content/1037374733410x15/fulltext.html
[13] Berguson, Emilie. “The Ethics of Gene Therapy”. NDSU. Copyright
1997. [Online Article]. Available: http://www.ndsu.edu/pubweb/~mcclean/plsc431/students/bergeson.htm
A
DDITIONAL
S
OURCES
Chang, Patricia L. “Somatic Gene Therapy”. CRC Press Inc. 1995.
[Online
Article]. Available: http://books.google.com/books?id=SHxjTBzrVxUC&printsec=frontcover& dq=somatic+gene+therapy&hl=en&sa=X&ei=WGEOT5yRF8fo0QHNx-
XLAw&ved=0CDsQuwUwAA#v=onepage&q=somatic%20gene%20therap y&f=false
“Choosing a Vector for CF Gene Therapy”.
The University of Utah. 2012.
[Online Interaction]. Available: http://learn.genetics.utah.edu/content/tech/genetherapy/cysticfibrosis/vector.
html
“Cystic Fibrosis gene therapy: possible cure?” About Cystic Fibrosis .
[Online Article]. Available: http://www.aboutcysticfibrosis.com/cysticfibrosis-gene-therapy.htm
Gene Therapy.net. (2012). “Adenoviral Vectors”. [Online Article].
Available: http://www.genetherapynet.com/viral-vectors/adenoviruses.html
Ginzinger, David G. (Dec 10, 2001) “Gene quantification using real-time quantitative PCR: An emerging technology hits the mainstream”. ISEH .
[Online Article]. Available: http://www.sciencedirect.com/science/article/pii/S0301472X02008068
Richter, Gerd, and Matthew D. Bacchetta. "Interventions In The Human
Genome: Some Moral And Ethical Considerations." Journal Of Medicine &
Philosophy 23.3 (1998): 303-317. Academic Search Premier. Web. 10 Jan.
2012. [Online PDF File].
Schoenstadt, Arthur. (June 23, 2009). “Cystic Fibrosis Gene Therapy”. eMedTv . [Online Article]. Available: http://cysticfibrosis.emedtv.com/cystic-fibrosis/cystic-fibrosis-gene-therapy.html
Wolf, Erik De. “Gene Therapy: A New Generation of Molecular Medicine”.
NDSU . 1997.
10 Jan. 2012. [Online Article]. Available: http://www.ndsu.edu/pubweb/~mcclean/plsc431/students/dewolf.htm
.
A CKNOWLEDGEMENTS
Kevin and I would like to thank our grader, Carol, for all of her insight and advice on our paper. We would like to thank
Janelle for meeting with Kevin and I and discussing ways to improve our paper throughout the process. Finally, we would like to thank our co-chair for her encouragement and insight.
6
Sean O’Connor
Kevin Hulbert
7