Measles
advertisement

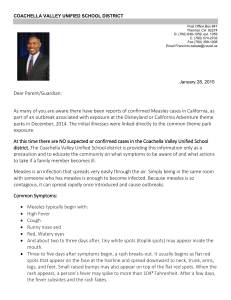
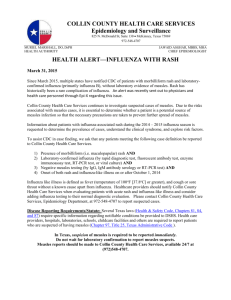
Measles Measles: The Skinny A highly communicable acute viral illness characterized by a maculopapular rash that begins at the head and spreads inferiorly to involve the trunk and extremities The rash is preceded by fever and the classic triad of cough, coryza, and conjunctivitis and a pathognomonic enanthem (Koplik spots). Measles continues to be a major public health problem in the developing world, where it causes significant morbidity and mortality. Measles are the leading cause of vaccine-preventable death and illness worldwide. Systems affected: primarily Hematologic/Lymphatic/Immunologic; Pulmonary; Skin; all systems may be affected by measles virus and/or its complications. Synonym: Rubeola Epidemiology Transmission: Direct contact with infectious droplets or airborne spread Droplets can remain in the air for hours. Highly infectious; 75–90% of susceptible contacts will develop the disease. Infectivity is greatest during the prodromal phase. Patients are considered contagious from 5 days before symptoms until 4 days after rash appears. Incubation period of ~12.5 days from exposure to onset of prodromal symptoms Risk Factors For developing measles: Not being immunized or failure to receive two doses of vaccine Travel to countries where measles is endemic Contact with exposed individuals, travelers, or immigrants General Prevention Totally preventable disease with vaccination usually given in combination with mumps and rubella (MMR); varicella now has been added to the combination Pathophysiology Measles virus enters respiratory mucosa and replicates within respiratory epithelial cells. The virus spreads to regional lymphatic tissues and is thought to disseminate to other reticuloendothelial sites (including conjunctiva, rep tract, urinary tract, small blood vessels, lymphatic system and CNS) via the bloodstream. Most complications are caused by disruption of epithelial surfaces and generalized immunosuppression that follows the disease. Measles may cause croup, pneumonia, diarrhea with protein-losing enteropathy, keratitis with scarring and blindness, encephalitis, and hemorrhagic rashes in malnourished children with poor medical care. Humans are the only natural host. Morphology. The blotchy, reddish brown rash of measles virus infection on the face, trunk, and proximal extremities is produced by dilated skin vessels, edema, and a moderate, nonspecific, mononuclear perivascular infiltrate. Ulcerated mucosal lesions in the oral cavity near the opening of Stensen ducts (the pathognomonic Koplik spots) are marked by necrosis, neutrophilic exudate, and neovascularization. The lymphoid organs typically have marked follicular hyperplasia, large germinal centers, and randomly distributed multinucleate giant cells, called Warthin-Finkeldey cells, which have eosinophilic nuclear and cytoplasmic inclusion bodies. These are pathognomonic of measles and are also found in the lung and sputum. The milder forms of measles pneumonia show the same peribronchial and interstitial mononuclear cell infiltration that is seen in other nonlethal viral infections. In severe or neglected cases, bacterial superinfection may be a cause of death. Medium power view of a lung biopsy from a patient with measles pneumonia shows a nodular pattern with acute and chronic inflammation and areas of necrosis and fibrosis. Multinucleated giant cells with inclusions (arrows) are also shown Diagnosis Diagnosis usually made clinically, or by serology or detection of viral antigen in nasal exudate or urinary sediment. History 1. Incubation period: average 10 days between exposure and prodrome 2. Prodromal period: Usually 2–3 days before rash, but may be up to 8 days: Fever: Begins 8–12 days after exposure; persists until 2–3 days after onset of rash High temperatures, i.e. fever, seen (39–40.5°C); febrile seizures are not uncommon in young children. Classic triad of “croupy” cough, coryza, and conjunctivitis Prodromal symptoms typically intensify over 2–4 days and peak on 1st day of rash before subsiding. Loose stools, malaise, irritability, photophobia (from iridocyclitis), sore throat, headache, and abdominal pain are also common symptoms. Note: corzya is an acute inflammation of the nasal mucosa accompanied by profuse nasal discharge Diagnosis cont. Physical Exam **Koplik spots** Pathognomonic of prodromal measles 2-3mm gray–white, raised lesions on erythematous base that appear on buccal mucosa Occur approximately 48 h before measles exanthum Described as "grains of salt on a red background" [6]. Koplik's spots subsequently may coalesce and generally last 12 to 72 hours 3. Examthem period: Rash (not pathognomonic): Maculopapular, blanches Begins at ears and hairline and spreads head to toe Discrete erythematous patches become confluent over time, with greater confluence on upper body than lower body. Clinical improvement usually occurs within 48 h of appearance of rash. Begins to fade 3–4 days after rash appears, leaving light brown discoloration of the skin Lymphadenopathy and pharyngitis may be seen during exanthem period. Koplik’s spots Early facial rash in a young boy with measles with spread to the neck and upper trunk. Coryza and conjunctivitis may be prominent at this stage. Blanching erythematous rash with some confluent areas on the trunk in a patient with measles. Erythematous rash in measles usually begins on the face and spreads centrifugally. By the time the rash appears on the lower trunk and extremities, it is frequently confluent on the face. Laboratory Most cases of measles are diagnosed clinically but, if necessary, detection of measles-specific IgM in blood or oral fluid, or genome or antigen detection from nasopharyngeal aspirates or throat swabs, can be used to confirm the diagnosis. Treatment Supportive therapy (i.e., antipyretics, antitussives, humidification, increased consumption of oral fluids) Vitamin A may be of benefit for patients with measles in areas where mortality >1%; unsure how it works but it is possible that supplemental vitamin A corrects a virallyinduced state of hyporetinemia Control: All patients with measles should be placed in respiratory isolation until 4 days after onset of rash; immunocompromised patients should be isolated for duration of illness. Notify public health officials of suspected cases. Prognosis Typically self-limited; prognosis good High fatality rates may be seen among malnourished or immunocompromised children, particularly in developing countries. Major causes of Death in Children Under Five in Developing Countries and the Contribution of Malnutrition