exenatide once weekly - The AstraZeneca Type 2 Diabetes Hub For
advertisement

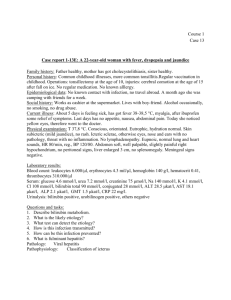
Bydureon® (exenatide once weekly) clinical data slide deck Date of approval: March 2015 | Date of expiry: March 2016 Approval code: 675,057.01 Developed with the guidance and approval of an independent international editorial committee Prescribing information can be found at the end of this slide deck. Content guide • This deck comprises a number of slides, arranged in story order. You may find that some slides are not relevant to your audience. Please hide these as you feel necessary • All graphs have been created in PowerPoint to enable easy amends and translation • HbA1c values and appropriate graphs include both DCCT (%) and IFFC (mmol/mol) units. Please delete where not appropriate for your market DCCT, Diabetes Control and Complications Trial; IFFC, International Federation of Clinical Chemistry and Laboratory Medicine. Executive summary • This slide deck covers the following topics and contains notes to provide further information on: 1. Introduction to Bydureon, microsphere technology and the steady-state principle 2. Overview of the Bydureon clinical trial programme (DURATION studies) 3. Data from the Bydureon DURATION-1, -2 and -3 studies • Overview of study design (primary analysis and extension periods) • Detailed data from long-term extension studies 4. Cardiovascular data from Bydureon studies 5. Bydureon safety and tolerability profiles 6. Dosing, administration and tips for initiating patients on Bydureon Introduction to Bydureon (exenatide once-weekly) About Bydureon • Bydureon is a GLP-1 receptor agonist, and the first once-weekly treatment for Type 2 diabetes – EU marketing authorisation received in June 2006 • Bydureon provides continuous glycaemic control in a single weekly injection • Bydureon is indicated for the treatment of Type 2 diabetes in combination with: – Metformin – SU – TZD – Metformin + SU – Metformin + TZD When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. GLP-1, glucagon-like peptide-1; SU, sulphonylurea; TZD, thiazolidinedione. Bydureon. Summary of product characteristics, 2014. Slide is animated Bydureon’s patented microsphere technology enables once-weekly dosing • Proven microsphere technology provides a continuous level of exenatide1 – Microspheres consist of a biodegradable polymer that dissipates into CO2 and water1 – The technology is also used in other extended-release products such as risperidone and naltrexone2,3 Subcutaneous injection of microsphere suspension of exenatide1 Individual microspheres aggregate and initial release of exenatide1 Microsphere degradation and continued release of exenatide1 Further degradation and metabolism of microsphere polymer provide sustained level of exenatide1 CO2, carbon dioxide. 1. DeYoung MB, et al. Diabetes Technol Ther 2011;13:1145–54; 2. Risperdal Consta. Summary of product characteristics, 2013; 3. Vivitrol. Prescribing information. Alkermes, Inc, 2013. Slide is animated Steady-state exenatide concentrations provide continuous glycaemic control with a single weekly injection • With once-weekly injections of Bydureon, therapeutic concentrations of exenatide are reached in 2 weeks1,2 • Steady state is reached by 6–7 weeks1,2 – At steady state, there are minimal peak-to-trough fluctuations in exenatide levels Steady state is maintained with subsequent weekly doses Plasma exenatide (pg/mL) 450 Weekly Bydureon injection 400 350 Steady state achieved for continuous glycaemic control 300 250 200 150 100 50 0 0 1 2 3 4 5 6 7 8 Time (weeks) 9 10 Figure adapted from Kim D, et al. 2007, showing mean ± standard deviation.2 1. Bydureon. Summary of product characteristics, 2014; 2. Kim D, et al. Diabetes Care 2007;30:1487–93. 11 12 13 14 Bydureon clinical trial programme Core design of DURATION trials • DURATION: Diabetes Therapy Utilisation: Researching Changes in A1c, Weight, and Other Factors Through Intervention with Exenatide Once Weekly • Primary endpoint: Change in HbA1c from baseline1–6 • Secondary endpoints included: Change in bodyweight, blood pressure and CV risk markers from baseline; safety and tolerability1–6 Bydureon 2 mg Patients with: Type 2 diabetes HbA1c 7.1–11.0% (54.1–96.7 mmol/mol) Active comparator agent(s) Optional Bydureon extension 24–30 weeks CV, cardiovascular. 1. Drucker DJ, et al. Lancet 2008;372:1240–50; 2. Bergenstal RM, et al. Lancet 2010;376:431–9; 3. Diamant M, et al. Lancet 2010;375:2234–43; 4. Russell-Jones D, et al. Diabetes Care 2012;35:252–8; 5. Blevins T, et al. J Clin Endocrinol Metab 2011;96:1301–10; 6. Buse JB, et al. Lancet 2013;381:117–24. Slide is animated Overview of DURATION trials Trial Comparator Background Subjects In EU label DURATION-11 Exenatide BID Open label Drug naïve, MET, SU, TZD, or two of these agents 295 DURATION-22 SITA (100 mg QD) or PIO (45 mg QD) Double-blind MET 491 DURATION-33 Insulin glargine Open label MET ± SU 456 DURATION-44 MET (2000 mg QD) or PIO (45 mg QD) or SITA (100 mg QD) Double-blind Drug naïve 820 DURATION-55 Exenatide BID Open label Drug naïve, MET, SU, TZD, or a combination of these agents 252 DURATION-66 Liraglutide (1.8 mg) Open label MET, SU, TZD, or a combination of these agents 911 • Data from DURATION-1, -2 and -3 are shown here as the primary studies included in the Bydureon summary of product characteristics7 – When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia7 Bydureon is not indicated in Europe as monotherapy in patients uncontrolled on diet and exercise alone.7 BID, twice daily; MET, metformin; PIO, pioglitazone; QD, once daily; SITA, sitagliptin; SU, sulphoylurea; TZD, thiazolidinediones. 1. Drucker DJ, et al. Lancet 2008;372:1240–50; 2. Bergenstal RM, et al. Lancet 2010;376:431–9; 3. Diamant M, et al. Lancet 2010;375:2234–43; 4. Russell-Jones D, et al. Diabetes Care 2012;35:252–8; 5. Blevins T, et al. J Clin Endocrinol Metab 2011;96:1301–10; 6. Buse JB, et al. Lancet 2013;381:117–24; 7. Bydureon. Summary of product characteristics, 2014. DURATION-1 DURATION-1: Study details DURATION-1: Primary analysis Study details N=295 (ITT population) Randomised, active-controlled, open-label, non-inferiority study Study length 30 weeks Background therapy None (as initial therapy) or treatment with metformin, a SU, a TZD or any combination of these agents Comparator to Bydureon Exenatide BID Primary endpoint HbA1c change from baseline at Week 30 Secondary endpoints Safety and tolerability; analysis of FPG, PPG, bodyweight, fasting glucagon, fasting lipids, blood pressure, exenatide pharmacokinetics, paracetamol absorption Publication type Peer-reviewed journal article When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. BID, twice daily; FPG, fasting plasma glucose; ITT, intent-to-treat; PPG, postprandial glucose; SU, sulphonylurea; TZD, thiazolidinedione. Drucker DJ, et al. Lancet 2008;372:1240–50. DURATION-1: Study details (continued) DURATION-1: 52-week extension study Study details N=258 (entering open-ended assessment period) Extension study after completing a 30-week randomised, activecontrolled, open-label, non-inferiority study Study length 22 weeks after completion of the 30-week primary study Background therapy None (as initial therapy) or treatment with metformin, a SU, a TZD or any combination of these agents Comparator to Bydureon Exenatide BID Bydureon at Week 30 Outcomes Glucose control during the transition from exenatide BID to Bydureon; safety and tolerability; efficacy of Bydureon at Week 52 Publication type Peer-reviewed journal article When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. BID, twice daily; SU, sulphonylurea; TZD, thiazolidinedione. Buse JB, et al. Diabetes Care 2010;33:1255–61. DURATION-1: Study details (continued) DURATION-1: 3-year extension study Study details N=258 (entering open-ended assessment period) Extension study after completing a 30-week randomised, activecontrolled, open-label, non-inferiority study Study length 3-year extension (switch study) Background therapy None (as initial therapy) or treatment with metformin, a SU, a TZD or any combination of these agents Comparator to Bydureon No comparator; pooled population included patients initated on Bydureon and those initiated on exenatide BID and switching to Bydureon at Week 30 Study endpoints Change in HbA1c, FPG, weight, lipid profile and SBP Publication type Peer-reviewed publication When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. BID, twice daily; FPG, fasting plasma glucose; SBP, systolic blood pressure; SU, sulphonylurea; TZD, thiazolidinedione. MacConell L, et al. Diabetes Metab Syndr Obes 2013;6:31–41. DURATION-1: Study details (continued) DURATION-1: 6-year extension study Study details N=258 (entering open-ended assessment period; completer population n=127) Extension study after completing a 30-week randomised, activecontrolled, open-label, non-inferiority study Study length 6-year extension (switch study) Background therapy None (as initial therapy) or treatment with metformin, a SU, a TZD or any combination of these agents Comparator to Bydureon No comparator; pooled population included patients initiated on Bydureon and those initiated on exenatide BID and switching to Bydureon at Week 30 Study endpoints Change in HbA1c, FPG, weight, lipid profile and SBP Publication type Congress abstract and poster presentation When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. BID, twice daily; FPG, fasting plasma glucose; SBP, systolic blood pressure; SU, sulphonylurea; TZD, thiazolidinedione. Henry RH, et al. Poster presented at ADA 2014. 964-P. DURATION-1: Reduced HbA1c with Bydureon versus exenatide BID over 1 year1 • At the primary endpoint of 30 weeks, HbA1c reductions from baseline were –1.9% (–20.8 mmol/mol) with Bydureon and –1.5% (–16.4 mmol/mol) with exenatide BID (p=0.0023)2 • At 1 year, patients receiving Bydureon maintained HbA1c reductions of –2.0% (–21.9 mmol/mol), regardless of whether they started on Bydureon or switched to Bydureon at 30 weeks1 – 71% of all patients achieved HbA1c <7% with Bydureon, irrespective of treatment at initiation 0 Exenatide BID Bydureon BL=8.2% (66.1 mmol/mol) –0.5 –5 –1.0 –10 Change from BL: –2.0% –1.5 –15 (21.9 mmol/mol) * –2.0 –20 * * –2.5 0 6 10 14 18 * * * * 22 26 30 Time (weeks) 33 –2.0% * 36 (21.9 mmol/mol) 40 Figure adapted from Buse JB, et al. 2010, showing least-squares mean ± standard error.1 *p<0.05 versus exenatide BID. BID, twice daily; BL, baseline. 1. Buse JB, et al. Diabetes Care 2010;33:1255–61; 2. Drucker DJ, et al. Lancet 2008;372:1240–50. 44 48 52 –25 Change in HbA1c (mmol/mol) 0.0 Change in HbA1c (%) All subjects received Bydureon Bydureon BL=8.3% (67.2 mmol/mol) DURATION-1: Reduced HbA1c with Bydureon sustained over 6 years • HbA1c reductions were sustained over 6 years with Bydureon (mean change in HbA1c from baseline –1.6% [95% CI, –1.9 to –1.4] [–17.5 mmol/mol])3 • 45% of all patients achieved HbA1c <7% with Bydureon, irrespective of treatment at initiation Change in HbA1c (%) –0.5 3 years2 (n=194) 6 years3 (n=127) BL=8.3% (67.2 mmol/mol) BL=8.2% (66.1 mmol/mol) BL=8.2% (66.1 mmol/mol) –5 –10 –1.0 –1.5 0 –1.6% –1.9% –1.6% –1.6% (–17.5 mmol/mol) (–17.5 mmol/mol) (–20.8 (17.5 mmol/mol) mmol/mol) –20 – 2.0 Randomised to Bydureon (evaluable population) –15 Pooled population (all Bydureon completers) Figure adapted from Drucker DJ, et al. 2008,1 MacConell L, et al. 2013,2 and Henry RH, et al. 2014.3 BID, twice daily; BL, baseline; CI, confidence interval. 1. Drucker DJ, et al. Lancet 2008;372:1240–50; 2. MacConell L, et al. Diabetes Metab Syndr Obes 2013;6:31–41; 3. Henry RH, et al. Poster presented at ADA 2014. 964-P. Change in HbA1c (mmol/mol) 0.0 30 weeks1 (n=148) DURATION-1: Weight reductions with Bydureon versus exenatide BID over 1 year* • Powerful HbA1c reductions with Bydureon were accompanied by weight reductions of 4.1–4.5 kg at 1 year1 All subjects received Bydureon Change in bodyweight (kg) 0 Bydureon BL=103 kg –1 Exenatide BID Bydureon BL=102 kg –2 –3 Change from BL: –4.1 kg –4 –4.5 kg –5 0 6 10 14 18 22 26 30 36 40 Time (weeks) Figure adapted from Buse JB, et al. 2010, showing least squares mean ± standard error.1 *Bydureon is not indicated for the treatment of obesity and weight change was a secondary endpoint in clinical trials. 3 BID, twice daily; BL, baseline. 1. Buse JB, et al. Diabetes Care 2010;33:1255–61; 2. MacConell L, et al. Presented at EASD 2013. Abstract 980; 3. Bydureon. Summary of product characteristics, 2014. 44 48 52 DURATION-1: Weight reductions with Bydureon sustained over 6 years* • Weight reductions with Bydureon were sustained over 6 years (mean reductions from baseline –4.3 kg [95% CI, –6.0 to –2.6]) 30 weeks1 (n=148) 3 years2 (n=194) 6 years3 (n=127) BL=102 kg BL=101 kg BL=101 kg Change in bodyweight (kg) 0 –1 –2 –3 –2.3 kg –1.6% (17.5 mmol/mol) –4 –5 –4.0 kg –4.3 kg Randomised to Bydureon (evaluable population) Pooled population (all Bydureon completers) Figures adapted from Drucker DJ, et al. 2008,1 MacConell L, et al. 2013,2 and Henry RH, et al. 2014.3 *Bydureon is not indicated for the management of obesity and weight change was a secondary endpoint in clinical trials. 4 BID, twice daily; BL, baseline. 1. Drucker DJ, et al. Lancet 2008;372:1240–50; 2. MacConell L, et al. Diabetes Metab Syndr Obes 2013;6:31–41; 3. Henry RH, et al. Poster presented at ADA 2014. 964-P; 4. Bydureon. Summary of product characteristics, 2014. DURATION-2 DURATION-2: Study details DURATION-2: Primary analysis Study details N=491 (ITT population) Randomised, double-blind, double-dummy, active-controlled superiority trial Study length 26 weeks Background therapy Metformin Comparators to Bydureon Sitagliptin 100 mg QD Pioglitazone 45 mg QD Primary endpoint Change in HbA1c from baseline at Week 26 Secondary endpoints Proportion of patients achieving HbA1c ≤6.5% (≤47.5 mmol/mol) or ≤7.0% (≤53.0 mmol/mol); FPG; six-point SMBG profile; bodyweight; fasting lipid profile; fasting insulin profile; blood pressure; CV risk markers; patientreported HRQoL; safety and tolerability Publication type Peer-reviewed journal article CV, cardiovascular; FPG, fasting plasma glucose; HRQoL, health-related quality of life; ITT, intent-to-treat; SMBG, self-monitored blood glucose; QD, once daily. Bergenstal RM, et al. Lancet 2010;376:431–9. DURATION-2: Study details (continued) DURATION-2: 52-week extension study Study details N=364 (entering extension study) Extension study after completing a 26-week randomised, double-blind, double-dummy, superiority trial Study length 26 weeks with a 26-week extension (switch study) Background therapy Metformin Comparators to Bydureon Patients initiated on sitagliptin 100 mg QD Bydureon at Week 26 Patients initiated on pioglitazone 45 mg QD Bydureon at Week 26 Outcomes Change from baseline at Weeks 26 and 52 and from Week 26 to Week 52 in: HbA1c; patients achieving HbA1c <7.0% (<53.0 mmol/mol) and ≤6.5% (≤47.5 mmol/mol); FPG; bodyweight; fasting lipids; fasting insulin; blood pressure; CV risk markers; safety and tolerability Publication type Peer-reviewed journal article CV, cardiovascular; FPG, fasting plasma glucose; QD, once daily. Wysham C, et al. Diabet Med 2011;28:705–14. DURATION-2: Reduced HbA1c with Bydureon versus sitagliptin and pioglitazone • At the primary endpoint of 26 weeks, HbA1c changes from baseline were –1.5% (–16.4 mmol/mol) with Bydureon, –0.9% (–9.8 mmol/mol) with sitagliptin and –1.2% (–13.1 mmol/mol) with pioglitazone (p<0.05 for Bydureon vs both comparators)1 • Significant HbA1c reductions with Bydureon were achieved at 1 year, regardless of initial therapy2 Bydureon, BL=8.6% (70.5 mmol/mol) Sitagliptin Bydureon, BL=8.5% (69.4 mmol/mol) Pioglitazone Bydureon, BL=8.5% (69.4 mmol/mol) 0 Change from Week 26 to Week 52: –0.31% (95 % CI, –0.50 to –0.13)* (–3.4 mmol/mol) 0.06% (95 % CI, –0.13 to 0.25) (0.7 mmol/mol) –0.10% (95 % CI, –0.29 to 0.09) (–1.1 mmol/mol) –0.5 –5 –10 –1.0 –15 –1.5 –20 –2.0 0 4 6 10 14 18 22 26 30 34 40 46 52 Time (weeks) Graph adapted from Wysham C, et al. 2011, showing data for the evaluable population as least squares mean ± standard error.2 *p<0.05 versus Week 26. BL, baseline; CI, confidence interval. 1. Bergenstal RM, et al. Lancet 2010;376:431–9; 2. Wysham C, et al. Diabet Med 2011;28:705–14. Change in HbA1c from baseline (mmol/mol) Change in HbA1c (%) 0.0 DURATION-2: Weight change* with Bydureon versus sitagliptin and pioglitazone • Patients treated with Bydureon achieved significant weight reductions at 26 weeks*1 – Individuals who switched to Bydureon from sitagliptin or pioglitazone at the end of the blinded period experienced further weight reductions2 Blinded period Open-label period Change in bodyweight (kg) 5 Bydureon, BL=90 kg Sitagliptin Bydureon, BL=86 kg Pioglitazone Bydureon, BL=86 kg 4 3 2 1 Change from Week 26: 0 –3.0 kg (95 % CI, –3.7 to –2.3)† –1 0.7 kg (95 % CI, 0.1 to 1.4)† –2 –1.1 kg (95% CI, –1.8 to –0.5)† –3 0 4 6 10 14 18 22 26 30 34 40 46 52 Time (weeks) Graph adapted from Wysham C, et al. 2011, showing data for the evaluable population (least squares mean ± standard error).2 †p<0.05 versus Week 26. *Bydureon is not indicated for the treatment of obesity and weight change was a secondary endpoint in clinical trials. 3 BL, baseline; CI, confidence interval. 1. Bergenstal RM, et al. Lancet 2010;376:431–9; 2. Wysham C, et al. Diabet Med 2011;28:705–14; 3. Bydureon. Summary of product characteristics, 2014. DURATION-3 DURATION-3: Study details DURATION-3: Primary analysis Study details N=456 (ITT population) Open-label, randomised, parallel-group study Study length 26 weeks Background therapy Metformin ± SU Comparator to Bydureon Insulin glargine (starting dose: 10 IU/day) Primary endpoint Change in HbA1c from baseline at Week 26 Secondary endpoints Patients achieving HbA1c <7.0% (<53.0 mmol/mol) and ≤6.5% (≤47.5 mmol/mol); FPG; SMBG; bodyweight; fasting plasma lipids; urinary ACR; CRP; HOMA β-cell function and insulin sensitivity; AAT; HRQoL; 1,5anhydroglucitol; safety and tolerability Publication type Peer-reviewed journal article When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. AAT, alanine aminotransferase; ACR, albumin-to-creatinine ratio; CRP, C-reactive protein; FPG, fasting plasma glucose; HOMA, homeostasis model assessment; HRQoL, health-related quality of life; SMBG, self-monitored blood glucose; SU, sulphonylurea. Diamant M, et al. Lancet 2010;375:2234–43. DURATION-3: Study details (continued) DURATION-3: Planned interim analysis at 84 weeks of open-ended extension study Study details N=390 (entering extension study) Open-label, randomised, parallel-group study Study length 26 weeks with open-ended extension study; interim analysis at 84 weeks Background therapy Metformin ± SU Comparator to Bydureon Insulin glargine (starting dose 10 IU/day; target glucose range, 4.0–5.5 mmol/L) Key efficacy measure Change in HbA1c from baseline to study treatment endpoint Secondary efficacy measures Time to failure to maintain glycaemic control; patients achieving HbA1c <7.0% (<53.0 mmol/mol) and ≤6.5% (≤47.5 mmol/mol); bodyweight; FPG; SMBG, fasting serum lipids Exploratory measures Urinary ACR; HOMA β-cell function; WHR; anti-exenatide antibody titre; safety and tolerability Publication type Peer-reviewed journal article When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. ACR, albumin-to-creatinine ratio; FPG, fasting plasma glucose; HOMA, homeostasis model assessment; SMBG, self-monitored blood glucose; SU, sulphonylurea; WHR, waist-to-hip ratio. Diamant M, et al. Diabetes Care 2012;35:683–9. DURATION-3: Study details (continued) DURATION-3: 3-year extension study Study details N=390 (entering extension study; completer population n=287) Open-label, randomised, parallel study Study length 26 weeks with 3-year extension Background therapy Metformin ± SU Comparator to Bydureon Insulin glargine (starting dose 10 IU/day; target glucose range, 4.0–5.5 mmol/L) Key efficacy measure Change in HbA1c from baseline to study treatment endpoint Secondary measures Patients achieving HbA1c <7.0% (<53.0 mmol/mol) and ≤6.5% (≤47.5 mmol/mol); bodyweight; FPG; SMBG, fasting serum lipids; patient-reported outcomes; safety and tolerability Exploratory measures Blood CRP concentrations; urinary ACR; WHR Publication type Peer-reviewed publication When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. ACR, albumin-to-creatinine ratio; CRP, C-reactive protein; FPG, fasting plasma glucose; SMBG, self-monitored blood glucose; SU, sulphonylurea; WHR, waist-to-hip ratio. Diamant M, et al. Lancet Diabetes Endocrinol 2014;2:464–73. DURATION-3: Reduced HbA1c with Bydureon versus basal insulin over 3 years • At the primary endpoint of 26 weeks, HbA1c reductions from baseline were –1.5% (–16.4 mmol/mol) with Bydureon and –1.3% (–14.2 mmol/mol) with insulin glargine (p=0.017)1 • Bydureon-treated patients experienced significantly greater HbA1c reductions at 3 years than those treated with insulin glargine2 Change from BL: 9 70 –0.81 ± 0.07% (–8.9 mmol/mol) 8 60 HbA1c (%) –1.01 ± 0.7% (–11.0 mmol/mol)* 6 50 5 40 4 30 3 20 2 1 Bydureon, BL=8.3% (67.2 mmol/mol; n=228) Insulin glargine, BL=8.3% (67.2 mmol/mol; n=220) 10 0 0 0 8 18 26 36 48 60 96 72 84 Time (weeks) 108 120 132 144 156 Graph adapted from Diamant M, et al. 2014, showing data for the modified intent-to-treat population as least squares mean ± standard error.2 *p=0.03. BL, baseline. 1. . Diamant M, et al. Lancet 2010;375:2234–43; 2. Diamant M, et al. Lancet Diabetes Endocrinol 2014;2:464–73. HbA1c (mmol/mol) 7 DURATION-3: Weight change with Bydureon versus basal insulin over 3 years • Treatment with Bydureon resulted in significant weight reduction instead of weight gain with insulin glargine over 3 years1 Bydureon, BL=91.2 kg (n=233) Insulin glargine, BL=90.6 kg (n=222) Change in bodyweight (kg) 4 Change from BL: +2.01 ± 0.28 kg 2 0 –2 –2.49 ± 0.28 kg* –4 0 8 18 26 36 48 60 72 84 96 Time (weeks) 108 120 132 144 156 Graph adapted from Diamant M, et al. 2014, showing data for the modified intent-to-treat population as least squares mean ± standard error.1 *p<0.001. BL, baseline. Bydureon is not indicated for the treatment of obesity and weight change was a secondary endpoint in clinical trials. 2 1. Diamant M, et al. Lancet Diabetes Endocrinol 2014;2:464–73; 2. Bydureon. Summary of product characteristics, 2014. DURATION-3: Individual associations between HbA1c and body weight with Bydureon versus insulin glargine at 26 weeks*1 Weight change from baseline (kg) 16 12 16% 0% 63% 5% 8 Bydureon Insulin glargine 4 0 –4 –8 –12 79% 4% 31% 1% –16 –6 –4 –2 0 2 HbA1c (%) change from baseline Modified ITT population, N=448. *Figure adapted from Diamant M, et al. Lancet 2010.1 *Bydureon is not indicated for the management of obesity and weight change was a secondary endpoint in clinical trials. 2 1. Diamant M, et al. Lancet 2010;375:2234–43; Bydureon. Summary of product characteristics, 2014. 4 6 DURATION-3: Incidence of minor hypoglycaemia versus insulin glargine • Bydureon was associated with a lower rate of minor hypoglycaemia than insulin glargine at 84 Patients reporting minor hypoglycaemia (%) weeks1 100 90 80 70 60 50 40 30 20 10 0 Bydureon (n= 233) Insulin glargine (n=223) 54% 32% * 8% n=13 n=51 Metformin background * 24% n=36 n=17 Metformin + SU background Graph adapted from Diamant et al. Diabetes Care 2012.1 *p<0.001. Minor hypoglycaemia was defined any time a paitent felt that he or she had a sign or symptom of hypoglycaemia that was associated with concurrent blood glucose <3.0 mmol/L and that was either self-treated by the patient or resolved independently.1 Three patients (one Bydureon + metformin, one insulin glargine + metformin and insulin glargine + metformin and SU) had an episode of hypoglycaemia requiring the assistance of another person, but not involving loss or severe impairment of consciousness, during the first 26 weeks. 1 • The exposure-adjusted rate of overall hypoglycaemia at 3 years was three times higher with insulin glargine (0.9 events/patient/year) than with Bydureon (0.3 events/patient/year)2 – SUs are associated with a higher risk of hypoglycaemia; when Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia 3 SU, sulphonylurea. 1. Diamant M, et al. Diabetes Care 2012;35:683–9; 2. Diamant M, et al. Lancet Diabetes Endocrinol 2014;2:464–73; 3. Bydureon. Summary of product characteristics, 2014. Change in CV risk markers with Bydureon Evidence from DURATION-1 Bydureon is not indicated for the management of blood pressure or cholesterol.1 CV, cardiovascular. 1. Bydureon. Summary of product characteristics, 2014. DURATION-1: Changes in blood pressure over 1 year with Bydureon • Over 1 year in the DURATION-1 study, improvements from baseline in blood pressure were seen with Bydureon treatment1,2 SBP Baseline Week 301 n=148 128 Year 12 n=148 129 DBP Week 301 n=148 78 Year 12 n=148 78 Change in BP (mmHg) 0 –1.7 mmHg –1 –2.8 mmHg –2 –3 –4 –4.7 mmHg –5 –6 –6.2 mmHg –7 Figure adapted from Drucker DJ, et al. 20081 and Buse JB, et al. 2010,2 showing ITT population of patients randomised to Bydureon (n=148). • At 1 year, 50% of patients with a high baseline SBP (≥130 mmHg) achieved a normal SBP2 Bydureon is not indicated for the management of blood pressure or cholesterol.3 DBP, diastolic blood pressure; SBP, systolic blood pressure. 1. Drucker DJ, et al. Lancet 2008;372:1240–50; 2. Buse JB, et al. Diabetes Care 2010;33:1255–61; 3. Bydureon. Summary of product characteristics, 2014. DURATION-1: Changes in lipid profile at 1 year with Bydureon • Over 1 year in the DURATION-1 study, improvements from baseline in plasma lipids were observed with Bydureon treatment1,2 Total cholesterol BL=4.49 –0.1 –0.2 –0.3 –0.31 mmol/L BL=4.40 –0.25 mmol/L –0.4 HDL-C Week 301 Year 12 BL=2.37 –0.13 mmol/L BL=2.30 Week 301 Year 12 BL=1.88 BL=1.82 0.1 0.0 –0.1 –0.09 mmol/L –0.2 –0.3 Triglycerides 0.1 Change from BL (mmol/L) Change from BL (mmol/L) 0.0 Year 12 0.0 –0.1 Week 301 Year 12 +0.02 mmol/L BL=1.14 BL=1.14 –0.02 mmol/L Change from BL (%) Change from BL (mmol/L) Week LDL-C 301 0 –5 –15% –10 –15 –15% Figures adapted from Drucker DJ, et al. 20081 and Buse JB, et al. 2010,2 showing ITT population of patients randomised to Bydureon (n=148). • Improvements were maintained for up to 6 years3 Bydureon is not indicated for the management of blood pressure or cholesterol.4 BL, baseline; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NR, not reported; TG, triglycerides. 1. Drucker DJ, et al. Lancet 2008;372:1240–50; 2. Buse JB, et al. Diabetes Care 2010;33:1255–61; 3. Henry RH, et al. Poster presented at ADA 2014. 964-P; 4. Bydureon. Summary of product characteristics, 2014. Bydureon safety and tolerability profile Bydureon: Summary of safety and tolerability profile • As with other GLP-1 receptor agonists,1–4 the most frequent adverse drug reactions (≥5% of patients treated with Bydureon) were mainly gastrointestinal-related (nausea, vomiting, diarrhoea and constipation) • In addition, injection-site reactions (pruritus, nodules, erythema), hypoglycaemia (with a SU) and headache occurred1 • Most adverse reactions associated with Bydureon were mild to moderate in intensity1 • There have been rare, spontaneously reported events of acute pancreatitis and renal failure. If pancreatitis is suspected, Bydureon should be discontinued1 Data source comprises two placebo-controlled studies (10 and 15 weeks) and three studies of Bydureon versus exenatide BID (30-week study), sitagliptin and pioglitazone (26-week study) or insulin glargine (26-week study). Background therapies included diet and exercise, metformin, a SU, a TZD or a combination of oral antidiabetic agents. BID, twice daily; SU, sulphonylurea; TZD, thiazolidinedione. 1. Bydureon. Summary of product characteristics, 2014; 2. Byetta. Summary of product characteristics, 2014; Victoza. Summary of product characteristics, 2014; 4. Lyxumia. Summary of product characteristics, 2014. Very common and common adverse reactions reported with Bydureon in clinical trials • Most adverse reactions associated with BYDUREON were mild to moderate in intensity and only infrequently* led to discontinuation System organ class/adverse reaction terms Metabolism and nutrition disorders Frequency of occurrence† Very common (≥1/10) Hypoglycaemia (with a SU)‡ Nausea‡ Vomiting‡ Diarrhoea‡ Constipation Dyspepsia‡ Abdominal pain‡ Gastroesophageal reflux disease‡ Abdominal distension‡ Eructation Flatulence‡ Hyperhidrosis‡ Skin and subcutaneous tissue disorders General disorders and administration site conditions Decreased appetite‡ Headache‡ Dizziness‡ Nervous system disorders Gastrointestinal disorders Common (≥1/100 to <1/10) Injection-site pruritus Fatigue‡ Injection-site erythema Injection-site rash Somnolence *The incidence of withdrawal due to adverse events in Bydureon-treated patients during the 30-week controlled trial was 6%. †Rate based on Bydureon clinical trial data (N=592 total; n=135 patients on SU) When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. ‡Reactions were in the same frequency grouping in the exenatide BID group. Data source comprises two placebo-controlled studies (10 and 15 weeks) and three studies of Bydureon versus exenatide BID (30-week study), sitagliptin and pioglitazone (26-week study) or insulin glargine (26-week study). Background therapies included diet and exercise, metformin, a SU, a TZD or a combination of oral antidiabetic agents. • There have been rare, spontaneously reported events of acute pancreatitis and renal failure. If pancreatitis is suspected, Bydureon should be discontinued BID, twice daily; SU, sulphonylurea; TZD, thiazolidinedione. Bydureon. Summary of product characteristics, 2014. Very common and common adverse reactions observed from clinical trial experience that were not observed with Bydureon at an incidence of ≥1% System organ class/adverse reaction terms Frequency of occurrence* Very common (≥1/10) Common (≥1/100 to <1/10) Skin and subcutaneous tissue disorders Hyperhidrosis General disorders and administration site conditions Asthenia Feeling jittery *Rate based on Bydureon clinical trial data (N=592 total; n=135 patients on SU). Data source comprises two placebo-controlled studies (10 and 15 weeks) and three studies of Bydureon versus exenatide BID (30-week study), sitagliptin and pioglitazone (26week study) or insulin glargine (26-week study). Background therapies included diet and exercise, metformin, a SU, a TZD or a combination of oral antidiabetic agents. When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. BID, twice daily; SU, sulphonylurea; TZD, thiazolidinedione. Bydureon. Summary of product characteristics, 2014. Handling nausea that may occur with Bydureon treatment Incidence of nausea (%) • Nausea is a frequent side effect with all GLP-1 receptor agonists1–4 • <1% of patients discontinued Bydureon due to nausea1 • Most episodes of nausea were mild to moderate and decreased over time1,5 100 80 60 40 20 0 Weeks Figure adapted from Maggs D, et al. 2012.5 • In a 52-week trial, even when patients experienced nausea, it did not affect their reported level of treatment satisfaction with Bydureon6 GLP-1, glucagon-like peptide-1. 1. Bydureon. Summary of product characteristics, 2014; 2. Byetta. Summary of product characteristics 2014 3. Victoza. Summary of product characteristics, 2014; 4. Lyxumia. Summary of product characteristics, 2014; 5. Maggs D, et al. Presented at EASD 2012. Presentation #4; 6. Best JH, et al. Diabet Med 2009;26:722–8. Handling injection-site reactions that may occur with Bydureon treatment Injection-site reactions versus bumps Injection-site bumps • Injection-site reactions associated • Small, raised nodules that very • • • with symptoms were categorised as adverse events (erythema, pruritus, rash) Occurred in 16% of patients in Phase III studies Mostly mild to moderate Usually did not lead to withdrawal from studies frequently occur at the injection site – These are consistent with known properties of poly (D,L-lactide coglycolide) polymer microsphere technology Size of bump • Bumps are normally harmless and resolve over 4–8 weeks Bydureon. Summary of product characteristics, 2014. Contraindications and special warnings and precautions Contraindications Hypersensitivity to the active substance or to any of the excipients. Warnings and precautions Not to be used in patients with Type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis. Bydureon must not be administered by intravenous or intramuscular injection. • Renal impairment Rare, spontaneously reported events of altered renal function with exenatide, including increase serum creatinine, renal impairment, worsened chronic renal failure and acute renal failure, sometimes requiring haemodialysis. Some occurred in patients experiencing events that may affect hydration and/or receiving medicinal products known to affect renal function/hydration status, including angiotensin converting enzyme inhibitors, angiotensin-II antagonists, non-steroidal anti-inflammatory medicinal products and diuretics. Reversibility observed with supportive treatment and discontinuation of potentially causative medicinal products, including exenatide. No dose adjustment required for patients with mild renal impairment (CrCl 50–80 mL/min). Very limited experience in moderate renal impairment (CrCl 30–50 mL/min). Not recommended in patients with moderate renal impairment, severe renal impairment (CrCl <30 mL/min) or end-stage renal disease. • Severe gastrointestinal disease Not recommended. Please see the Bydureon summary of product characteristics for full safety information. CrCl, creatinine clearance. Bydureon. Summary of product characteristics, 2014. Contraindications and special warnings and precautions (continued) • Acute pancreatitis Rare, spontaneously reported events of acute pancreatitis. Inform patients of the characteristic symptom of acute pancreatitis: Persistent, severe abdominal pain. Resolution of pancreatitis has been observed with supportive treatment, but very rare cases of necrotising or haemorrhagic pancreatitis and/or death have been reported. If pancreatitis suspected, discontinue use of Bydureon and other potentially suspect medicinal products. Do not resume Bydureon after pancreatitis has been diagnosed. • Concomitant medicinal products Concurrent use of Bydureon with insulin, meglitinides, alpha-glucosidase inhibitors, dipeptidyl peptidase-4 inhibitors or other GLP-1 receptor agonists has not been studied. The concurrent use of Bydureon and exenatide BID has not been studied and is not recommended. • Weight loss Rapid weight loss at a rate of >1.5 kg per week has been reported with exenatide, which may have harmful consequences. • Discontinuation of treatment The effect of Bydureon may continue as plasma levels of exenatide decline over 10 weeks. Choice of other medicinal products and dose selection should be considered accordingly until exenatide levels decline. Please see the Bydureon summary of product characteristics for full safety information. BID, twice daily; GLP-1, glucagon-like peptide-1. Bydureon. Summary of product characteristics, 2014. Drug interactions No dose adjustment required for medicinal products sensitive to delayed gastric emptying. • Warfarin and cumarol derivatives Increased INR reported during concomitant use of warfarin and exenatide. INR should be monitored during initiation of Bydureon. • HMG CoA reductase inhibitors Concomitant use with exenatide was not associated with consistent changes in lipid profiles. Lipid profiles should be monitored as appropriate. Please see the Bydureon summary of product characteristics for full safety information. AUC, area under curve; BID, twice daily; HMG, hydroxy methyl glutaryl coenzyme A; INR, international normalised ratio. Bydureon. Summary of product characteristics, 2014. Anti-exenatide antibodies • Patients may develop antibodies to Reduction in mean HbA1c by antibody status2 exenatide following treatment with Bydureon • Four clinical trials showing clinically relevant HbA1c reduction regardless of antibody status2 A small proportion of patients (2.6%) had higher titres and showed no glycaemic improvement1 Change in HbA1c (%) • 0.0 Antibodynegative patients Antibodypositive patients n=280 n=371 –5 –0.5 –1.3% –1.0 –1.6% –1.5 0 (–15.5 mmol/mol) –2.0 1. Bydureon. Summary of product characteristics, 2014; 2. Fineman MS, et al. Diabetes Obes Metab 2012;14:546–54. –10 (–14.2 mmol/mol) –15 –20 Change in HbA1c (mmol/mol) – Consistent with the potentially immunogenic properties of protein and peptide pharmaceuticals1 – In clinical studies of Bydureon, approximately 45% of patients had low-titre antibodies at the study endpoint1 – Antibody titres usually diminish over time1 Bydureon dosing, administration and initiation Bydureon dosing • Bydureon comes in a convenient single-dose kit that contains everything patients need to prepare and deliver their once-weekly injection – Injection can be administered at any time of the day, independently of meals – Fixed dose with no titration required – Patients can change their day of weekly dosing as long as doses are 1 day apart* CONNECT SHAKE INJECT Connect the parts securely before mixing Shake vigorously to mix the medicine with the liquid Attach the needle, line up the plunger with the dose line, and inject *If a dose is missed, it should be administered as soon as practical. Thereafter, patients can resume their once-weekly dosing schedule. The use of Bydureon does not require additional self-monitoring of blood glucose. Bydureon. Summary of product characteristics, 2014. Bydureon device: Overview of the Connect, Shake, Inject process • Contains an overview of the injection device – Straightforward dosing: Connect, Shake, Inject – Remember: Patients should follow all of the steps in the instructions for the user that comes with the single-dose kit Bydureon. Summary of product characteristics, 2014. The Bydureon usability study • A usability study of 102 individuals with Type 2 diabetes found that 88% of patients were able to prepare and deliver a dummy dose of Bydureon Subjects who succeeded in preparing and delivering a dose of Bydureon Questionnaire responses to ‘If I only had the instructions for use, I could use the single-dose kit at home’ 2% Did not complete (n=2) 7% 11.8% (n=7) (n=12) With use of customer 15.7% support (n=16) helpline Strongly agree Agree Neutral Disagree/ strongly disagree 22% (n=22) 72.6% (n=74) (n=70) Without assistance Adapted from Lorenzi G, et al. Clin Diabetes 2010;28:157–62. 69% Expectation setting: Benefits • To maximise adherence, a care plan should be agreed with the individual patient, including setting of expectations by the HCP, upon initiation of treatment • Explain to patients that, due to its unique once-weekly formulation, they need to give Bydureon time to work When you may see an effect Changes patients may notice After four doses1,2 • FPG improvements • PPG improvements After six or seven doses1,3 • HbA1c reductions Over time1 • Feeling less hungry and eating less • Most patients will experience weight reduction* *Bydureon is not indicated for the management of obesity and weight change was a secondary endpoint in clinical trials. 1 FPG, fasting plasma glucose; HCP, healthcare professional; PPG, postprandial glucose. 1. Bydureon. Summary of product characteristics, 2014; 2. Blevins T, et al. J Clin Endocrinol Metab 2011;96:1301–10; 3. Drucker DJ, et al. Lancet 2008; 372:1240–50. Once-weekly Bydureon: Continuous glycaemic control for your patients • Bydureon provides powerful efficacy with HbA1c reductions, sustained for up to 6 years1 • Potential for sustained weight reduction over 6 years* and low risk of hypoglycaemia†1,2 • Withdrawal rate of <1% due to nausea and vomiting2 • The most frequent adverse reactions (≥5% of Bydureon patients) were mainly gastrointestinal related (nausea, vomiting, diarrhoea and constipation)2 – In addition, injection-site reactions (pruritus, nodules, erythema) were observed • Straightforward administration that patients can manage in a once-weekly injection2,3 *Bydureon is not indicated for obesity and weight change was a secondary endpoint in clinical trials.2 †SUs are associated with an increased risk of hypoglycaemia. When Bydureon is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia.2 1. Henry RH, et al. Poster presented at ADA 2014. 964-P; 2. Bydureon. Summary of product characteristics, 2014; 3. Lorenzi G, et al. Clin Diabetes 2010;28:157–62. This information is consistent with the UK marketing authorisation. Please refer to your local prescribing information for full details. This information is consistent with the UK marketing authorisation. Please refer to your local prescribing information for full details.