The Obesity/Diabetes Epidemic:
Adiposopathy & ObesityThe New Disease!
Dx & (Rx) of Insulin Resistance & Early
DM (Part 1)
Stan Schwartz MD, FACP, FACE
Private Practice, Ardmore
Obesity Program
Cardiometabolic Diabetes Center and Affiliate,
Main Line Health System
Emeritus, Clinical Associate Professor
University of Pennsylvania
Disclosures
Advisor
Takeda, Amylin, A-Z, BMS, Novo. Merck, Santarus
Speaker
Lilly, Amylin, Takeda, Novo, BMS, Santarus
Merck, Astra-Zeneca
Lecture Based on Evidence -Based
PRACTICE
EBM=Evidence
Based Medicine
=
Has Led to Students/MDs who don’t Think
Research Evidence
EBM=Eviden
ce
Based
Medicine
=
+
Randomized, Prospective
Publication Trials
Critical Appraisal
Patient-Based
Experience
=Evidence
Based Practice
Clinical expertise
Expert Opinions
Guidelines
Duggal, Evidence-Based Medicine in Practice,, Int’l j. Clinical Practice,65:639-644,201
Defining Obesity- A Disease, ADA 6/2013
• Body Mass Index
– Evaluates weight relative to height (kg/m2)
– Correlates highly with body fat, morbidity, and mortality
• Categories
– Underweight (< 18.5 kg/m2)
– Normal weight (18.5-24.9 kg/m2)
–
–
–
–
Overweight (25.0-29.9 kg/m2)
Class I Obesity (30.0-34.9 kg/m2)
Class II Obesity (35.0-39.9 kg/m2)
Class III Obesity (> 40 kg/m2)
NIH National Heart, Lung, and Blood Institute. Obes Res. 1998;6(suppl 2):51S
Waist Circumference correlates with BMIbut BMI not closely correlated with IR- Leads to….
Even some HIGH BMI FOLK have normal IR
Leads to ConceptMetabolically Healthy Obese
Are Metabolically
Healthy Overweight
and Obesity Benign
Conditions?:
NO!!
THUS=
OXYMORON
Meta-analyses of various clinical
characteristics, by metabolic–body mass
index categories.
Data shown as weighted mean difference
compared with metabolically healthy normalweight persons (reference). To convert
cholesterol, triglyceride, and glucose values
to traditional units (mg/dL), divide by 0.0259,
0.0113, and 0.0555, respectively. HOMA-IR =
Homeostasis Model Assessment of Insulin
Resistance.* P < 0.05.
Date of download:
Ann Intern Med. 2013;159(11):758-769. doi:10.7326/0003-4819-159-11-201312030-00008
12/14/2013
Copyright © American College of Physicians. All rights reserved.
Obesity Paradox
•
some long-term studies have shown that weight loss in overweight and obesity is associated
with increased mortality coupled with many CV studies showing a better prognosis with a
higher BMI
CHF
better if
outcomes
Obese
suggested that purposeful weight loss may not be beneficial and may even be detrimental in patients with CV
diseases
•
In contrast, other studies assessing mortality based on body fat and lean mass suggested that subjects losing body
fat rather than lean mass have a lower mortality
•
Potential adverse effects of weight loss may be explained by wrong methods of wt. loss.
eg: starvation, very-low-calorie diets, liquid protein diets, and obesity surgeries have been associated with
prolongation of the QTc interval and increased risk of malignant dysrhythmias (1), and various pharmacologic
agents have either limited efficacy or considerable toxicity (70-72).
Overwhelming evidence supports the importance of obesity in the pathogenesis and progression
of CV disease. Although an obesity paradox exists,, the constellation of data still support
purposeful weight reduction in the prevention and treatment of CV diseases
Carl J. Lavie, MD; Richard V. Milani, MD; Hector O. Ventura, MDJ Am Coll Cardiol. 2009;53(21):1925-1932.
Obesity Paradox
:Metabolically Healthy Obese Patients still has
Increased CV rates and All Cause mortality
And have other adverse outcomes related to DJD and Sleep Apnea, for example
Outline
•
•
•
•
•
Epidemiology and Economics of obesity/diabetes
Perspectives on Obesity
Consequences of Obesity, Prediabetes, Obesity
Obesity/ Diabetes Risk Factors,
Obesity/ Diabetes Onset can be Prevented or Delayed –
Early Risk Identification and Intervention.
• Medical Benefits to Weight Loss
• Treatment-CDC’s diabetes prevention program and
other Evidence-Based Interventions– Basics,
– Next Lecture in Series
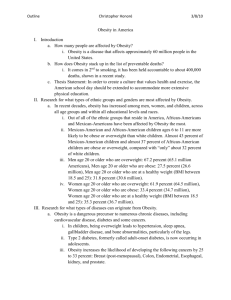
Overweight and Obesity Prevalence
Increasing Among U.S. Adults
70
Obesity
Prevalence (%)
.
60
Overweight
50
40
30
20
10
0
1960-62
1971-74
1976-80
1988-94
1999-2002
2003-2004
NHANES Data Collection Period
Flegal KM et al. JAMA 2002;288:1723-27
Hedley AA et al. JAMA 2004;291:2847-50
Ogden CL et al. JAMA 2006;295:1549-55
Leads to
Diabetes
Epidemic
An Expensive Epidemic
• 56 million Americans have
a BMI of 30-40
– Had healthcare costs
36 percent greater than
normal-weight individuals
– Had pharmacy costs
77 percent greater than
normal-weight individuals
• Nearly 10% of annual
medical spending was for
overweight and obese
patients
• Total medical cost for
obesity in 2003 was
$75 billion.
Finkelstein,Jan/2004Obesity
Sturm,
Research
Ph.D. Archives of Medicine
Direct Cost* of Chronic Diseases
in the United States
60
$53.2
$51.6
50
$38.7
Direct Cost (Billions $)*
40
30
$18.4
20
$18.1
10
0
Type 2
Diabetes
Obesity
Hypertension
Coronary
Heart Disease
Stroke
*Adjusted to 1995 dollars.
Wolf and Colditz. Obes Res 1998;6:97.
Hodgson and Cohen. Med Care 1999;37:994.