Chapter 4
PART I: Essential Pathology - Mechanisms of Disease
Neoplasia
Companion site for Molecular Pathology
Author: William B. Coleman and Gregory J. Tsongalis
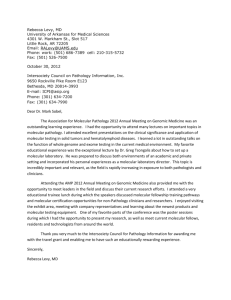
FIGURE 4.1
Cancer incidence and mortality by site for both sexes (United States, 2008).
The relative contributions of the major forms of cancer to overall cancer incidence and cancer-related
mortality (both sexes combined) were calculated from data provided by Jemal et al. [2]. Cancers of the
reproductive organs include those affecting the prostate, uterine corpus, ovary, uterine cervix, vulva,
vagina, testis, penis, and other organs of the male and female genital systems. Cancers of the
digestive system include those affecting esophagus, stomach, small intestine, colon, rectum, anus,
liver, gallbladder, pancreas, and other digestive organs. Cancers of the respiratory system include
those affecting the lung, bronchus, larynx, and other respiratory organs.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
2
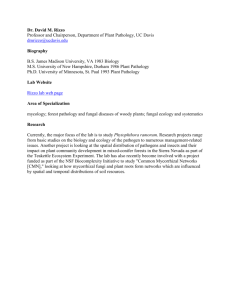
FIGURE 4.2
Age-specific incidence and mortality rates for selected sites, 1992–1996.
The age-specific rates for breast cancer incidence and mortality are for females only. The age-specific
rates for lung cancer and colorectal cancer are combined for both sexes.
These data were adapted from the NCI SEER Statistics Database (http://seer.cancer.gov/index.html).
Rates are per 100,000 population and are age-adjusted to the 1970 standard population of the United
States.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
3
FIGURE 4.3
Progression of dysplasia in the cervix.
(A) Normal squamous epithelium of the cervix. The basal (bottom) layer of cells appears dark, and there is cellular
maturation as the squamous cells move to the surface. (B) Low-grade squamous dysplasia. The basal layer appears
thicker with mild nuclear pleomorphism and mitotic figures involving the lower third of the epithelium. In this image,
several HPV-infected cells, known as koilocytes, are present in the middle third of the epithelium. A koilocyte has a
wrinkled nucleus with cytoplasmic clearing. (C) Moderate squamous dysplasia. The dysplastic squamous cells and
mitotic figures involve the lower two-thirds of the epithelium. There is still some maturation toward the surface of the
epithelium. (D) High-grade squamous dysplasia. Dysplastic squamous cells and mitotic figures involve the full thickness
of the epithelium. There is no invasion into the underlying stroma. (E) Invasive squamous cell carcinoma. Dysplastic
squamous cells invade into the underlying stroma in a haphazard fashion. There is prominent inflammation in the
stroma in response to the invasive carcinoma.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
4
FIGURE 4.4
Progression of neoplastic transformation in the colon.
(A) Low-grade glandular dysplasia. This image is of an adenomatous colon polyp, which is, by
definition, polypoid low-grade dysplasia of the colonic glandular epithelium. The nuclei are
hyperchromatic (dark) with pseudostratification (overlapping) and a higher nuclei to cytoplasmic ratio
(the nucleus is occupying a larger percentage of cell volume than in a normal colon epithelial cell). (B)
High-grade glandular dysplasia. Sometimes adenomatous polyps can harbor high-grade dysplasia.
Features of high-grade dysplasia include both increased architectural complexity, including back-toback glands without intervening stroma, and increased degree of nuclear pleomorphism. (C) Invasive
adenocarcinoma. Glands, lined by dysplastic cells, are haphazardly invading through the musculars
mucosa and into the underlying submucosa.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
5
FIGURE 4.5
Adrenal adenoma.
The normal cortex of the adrenal gland is yellow-gold in appearance. The white arrow points to a welldelineated, round lesion arising in the adrenal cortex. It does not appear to invade into the adjacent
tissue.
Courtesy of Kirsten Boland, MHS, PA(ASCP).
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
6
FIGURE 4.6
Pancreatic adenocarcinoma.
This is a cut section of a pancreatic tumor. It is poorly delineated (meaning it is difficult to identify the
exact borders of the lesion) and appears to be infiltrating into adjacent adipose tissue (patchy bright
yellow areas along the bottom of the specimen).
Courtesy of Kirsten Boland, MHS, PA(ASCP).
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
7
FIGURE 4.7
Neoplasms of mixed cell type.
(A) Mature teratoma. This example demonstrates mature cartilage (right) and skin (left). (B) Immature
teratoma. This type of teratoma contains areas of primitive-appearing hyperchromatic cells, known as
blastema. There is focal rosette formation (white arrow).
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
8
FIGURE 4.8
Metaplastic change in the stomach.
(A) Normal glandular epithelium of the stomach. (B) Intestinal metaplasia. This image displays
glandular epithelium of the stomach with goblet cells (white arrows). Goblet cells contain a large,
round intracytoplasmic vacuole of mucin and are normally found in the small and large intestine only.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
9
FIGURE 4.9
Epithelial hyperplasia of the breast.
Normal mammary ducts are lined by a single layer of cuboidal epithelial cells (as in the duct second
from the center bottom). The lumens of the remaining ducts in this image are filled with bland
appearing-epithelium cells, representing prominent ductal epithelial hyperplasia.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
10
FIGURE 4.10
Nuclear pleomorphism and abnormal mitotic figures in neoplastic cells.
(A) Pleomorphism. This is an example of leiomyosarcoma. Several of the malignant stromal cells are
very large and different in shape from neighboring cells. (B) Mitotic figure (center). Malignant
neoplasms often have an increased number of mitotic figures.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
11
FIGURE 4.11
Progression of tumorigenesis in the breast.
(A) Ductal carcinoma in situ (DCIS) of the breast. The lumen of this mammary duct is filled with
pleomorphic cells with high nuclear to cytoplasmic ratios. Scattered mitotic figures are noted. This
neoplastic process is in situ carcinoma because the dysplastic cells are confined to the lumen of the
duct and have not invaded into the surrounding tissue. (B) Invasive adenocarcinoma of the breast.
Glands lined by dysplastic cells haphazardly infiltrate into adipose tissue.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
12
FIGURE 4.12
Childhood neuroblastoma.
Neuroblastoma is considered one of the so-called small, round, blue cell tumors, as it is composed of
small, hyperchromatic, monomorphic cells with scant cytoplasm.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
13
FIGURE 4.13
Lymphoma.
This image of lymphoma demonstrates sheets of large cells with prominent nucleoli. Subclassification
of the lymphoma depends on several additional laboratory tests.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
14
FIGURE 4.14
Cellular pleomorphism.
The dysplastic cells in this adenocarcinoma demonstrate marked pleomorphism, meaning the cells
vary widely in size and shape. The arrangement of the dysplastic cells is disordered, with only some
residual gland formation.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
15
FIGURE 4.15
Tumor necrosis.
Necrotic (dead tissue) debris is present within the center of the malignant glands in this
adenocarcinoma.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
16
FIGURE 4.16
Metastatic spread of malignant cells through the lymphatic system.
(A) Metastatic adenocarcinoma to a lymph node, low power. Residual lymph node tissue is present
along the upper portion of the image. Infiltrating glands of adenocarcinoma are noted at the lower
aspect of the image. (B) Metastatic carcinoma to a lymph node, high power. Two nests of plump
malignant epithelial cells are present within the sea of smaller lymphocytes of the lymph node.
Companion site for Molecular Pathology
Copyright © 2009 by Academic Press. All rights reserved.
17