Lecture 9
advertisement

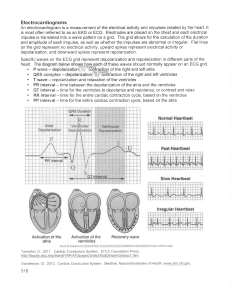
CARDIOVASCULAR PHYSIOLOGY Lecture 9 ECG Paper ECG paper is a long, continuous roll of graph paper, usually pink (but any color will do), with light and dark lines running vertically and horizontally. The light lines circumscribe small squares of 1 X 1 mm; the dark lines delineate large squares of 5 X 5 mm.The horizontal axis measures time. The distance across one small square represents 0.04 seconds. The distance across one large square is five times greater, or 0.2 seconds. The electrocardiogram is recorded on to standard paper travelling at a rate of 25 mm/s. Figure1: time scale of ECG paper The vertical axis measures voltage. The distance along one small square represents 0.1 mV, and along one large square, 0.5 mV. The electrocardiogram machines are calibrated so that a signal with an amplitude of 1 mV moves the recording stylus vertically10 mm( 2 large squares). Figure2:Standard calibration signal 1 Configuration( shape and appearance of ECG wave). When one portion of the atria or ventricles depolarized it becomes electronegative with respect to the remainder polarized area, thus a dipole is formed and electrical current flows. This currents can flow freely to the surface of the body through the body fluids and tissues which are relatively good volume conductor. The pattern of deflection recorded by the leads on the surface of the body depend on relation of the exploring (active) electrode of a given lead to the depolarization or repolarization wave (vector).This vector is represented as an arrow between the two poles with the head of arrow(vector) in positive direction ( + ). Figure3 : Arrows(vector) show the direction of depolarization wave. The record will show positive(upward) deflection when the exploring electrode of a given lead faces the head of the depolarization or repolarization vector, while it record negative deflection, when the exploring electrode of a given lead faces the tail of the depolarization or repolarization vector regardless of whether or not the electric force is going towards or away from the positive pole of the lead(Note: The record will be equiphasic, when the wave of depolarisation is at right angles to the lead). Figure 4 :The direction of the deflection of ECG wave depends on orientation of active electrode in relation to wave of depolarization or repolarization. The amplitude of the wave form recorded in any lead may be influenced by the myocardial mass, the net vector ( ) of depolarization or repolarization wave, the thickness and properties of the intervening tissues, and the distance between the electrode and the myocardium. Patients with ventricular 2 hypertrophy have a relatively large myocardial mass and are therefore likely to have high amplitude waveforms. In the presence of pericardial fluid, pulmonary emphysema, or obesity, there is increased resistance to current flow, and thus waveform amplitude is reduced. The direction of the deflection on the electrocardiogram depends on whether the depolarization or repolarization wave vector is travelling towards or away from a detecting ( positive or active) electrode. Normal ECG The configuration and nomenclature of the of a normal ECG waves is as follows: 1.P wave: The P wave represents depolarization of the atria. The normal atrial depolarization wave vector is oriented downward and toward the subject’s left, reflecting the spread of depolarization from the sinus node to the right and then the left atrial myocardium. Since this vector points toward the positive pole of lead II and toward the negative pole of lead aVR, the normal P wave will be positive in lead II and negative in lead aVR. P wave amplitude rarely exceeds two and a half small squares (0.25 mV). The duration of the P wave is less than0.12 second, it correlates with conduction time through the atria; for example, if conduction velocity through the atria decreases, or atrial enlarged, the P wave will spread out. Atrial repolarization (Ta) is not seen on a normal ECG, because it is "buried" in the QRS complex. The wave of atrial repolarization (Ta), but it coincides with ventricular depolarization and is hidden by the much more prominent QRS complex). Figure5: P wave represents depolarization of the atria. Because the sinus node is located in the right atrium, the right atrium begins to depolarize before the left atrium and finishes earlier as well. Therefore, the first part of the P wave predominantly represents right atrial depolarization, and the second part left atrial depolarization. Figure6: right and left atrial component of P wave 3 2. PR interval. The PR interval is the time from initial depolarization of the atria to initial depolarization of the ventricles. Thus, the PR interval includes the P wave and the PR segment, an isoelectric (flat) portion of the ECG that corresponds to AV node conduction. Because the PR interval includes the PR segment, it also correlates with conduction time through the AV node. Normally, the PR interval duration is 0.12-0.20 second, which is the cumulative time from first depolarization of the atria to first depolarization of the ventricles. Increases in conduction velocity through the AV node decrease the PR interval (e.g., due to sympathetic stimulation), and decreases in conduction velocity through the AV node increase the PR interval (e.g., due to parasympathetic stimulation). Figure7: The PR interval 3. QRS complex. The QRS complex consists of three waves: Q, R, and S. Collectively, these waves represent depolarization of the ventricles. Capital letters (Q, R, S) denote largeamplitude deflections (≥5 mm or 0.5 mV), whereas lowercase letters (q, r, s) signify low-amplitude deflections (≤5 mm or 0.5 mV). Q, q, S, and s waves are negative excursions from the isoelectric baseline, whereas R and r waves are positive deflections. Q and q waves are initial negative deflections, and S and s waves are negative deflections that follow a positive deflection (R or r wave). The duration of the QRS complex reflects the time required for ventricular depolarization. The first step in depolarization of the ventricles is depolarization of the interventricular septum from the left to the right and anteriorly producing a current flow toward right, Then the simultaneous depolarization of the right and left ventricles; produce current points leftward and posteriorly due to large mass of left ventricl. Therefore, a right precordial lead (V1)will record a small positive deflection (septal r wave)followed by a larger negative deflection (S wave). While a left precordial lead, e.g., V6, will record a small negative deflection (septal q wave)followed by a relatively tall positive deflection (R wave). Figure 8: ventricular depolarization 4 Intermediate leads show a relative increase in R-wave amplitude (normal Rwave progression)and a decrease in S-wave amplitude progressing across the chest from the right to left. The precordial lead where the R and S waves are of approximately equal amplitude is referred to as the transition zone (usually V3 or V4). QRS complex duration range from 0.08 - 0.1 second, if the QRS duration is is more than 0.1 second, consider an intraventricular or interventricular conduction such as incomplete LBBB, incomplete RBBB, or WPW syndrome .The R-wave height should not exceed 25mm in leads V5 and V6, or 20mm in leads I and aVL. Q waves Normally present in aVR; occasionally in V1 or in aVL its <0.04 second duration. The amplitude of Q wave is ≤3 mm deep (does not usually exceed 25% of the following R wave). Note that the total duration of the QRS complex is similar to that of the P wave. This fact may seem surprising since the ventricles are so much larger than the atria; however, the ventricles depolarize just as quickly as the atria, because conduction velocity in the His-Purkinje system is much faster than in the atrial conducting system. ST segment The point Where the QRS complex ends is called the J point. At that time, all of the ventricular cells are depolarized and no voltage differences exist on the heart. For that reason, the voltage in the ECG returns to zero for a moment before the onset of the T wave. The J point is more commonly called the ST segment (the flat region between the end of the QRS and the start of the T wave). In a normal ECG, the ST segment should always be at the same level as the baseline, zero volts. Figure9: ST segment T wave The T wave represents repolarization of the ventricles. The entire outer surface of the ventricles, especially near the apex of the heart repolarized first and the endocardial areas repolarize last. This sequence of repolarization is postulated to be caused by the high blood pressure inside the ventricles during contraction, which greatly reduces coronary blood flow to the endocardium, thereby slowing repolarization in the endocardial areas. Because the outer apical surfaces of the ventricles repolarize before the inner surfaces, the positive end of the overall ventricular vector during repolarization is toward the apex of the heart similar to that of depolarization. However, the vector of wave of ventricular repolarization receding backward in opposite to that of depolarization vector that precede forward . Thus, the same electrodes that recorded a positive deflection during depolarization (appearing as a tall R wave) will also generally record a positive deflection during repolarization (appearing as a positive T wave). It is therefore 5 typical and normal to find positive T waves in the same leads that have tall R waves. T wave amplitude rarely exceeds 10 mm. Tall T waves may be seen in acute myocardial ischaemia and are a feature of hyperkalaemia. Figure10: T wave ( repolarization of the ventricles). 5.QT interval. The QT interval includes the QRS complex, the ST segment, and the T wave, and represents first ventricular depolarization to last ventricular repolarization. It is measured from the onset of the QRS complex to the end of the T wave. The QT interval must be corrected to allow comparison of this interval at differing heart rates. Bazett's formula defines a corrected QT interval The ST segment is an isoelectric portion of the QT interval that correlates with the plateau of the ventricular action potential. Accurate assessment of the repolarization interval is important inasmuch as patients with prolonged repolarization, either congenital or acquired, may be at risk for a torsades de pointes ventricular tachycardia. A short QT interval may be due to early repolarisation, digitalis effect and may associated with some genetic disorders . Figure11: The QT interval 6