Source - Gilberto De Nucci
advertisement

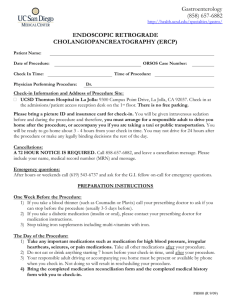
Dúvidas denucci@gilbertodenucci.com Arquivo Importância da Farmacologia na Terapêutica Site: www.gilbertodenucci.com Solicitar aulas para: guilherme@lexxa.com.br Importância de Reações Adversas a Medicamentos (RAM) • 2 milhões de RAM anualmente nos EUA • Cem mil mortes por ano • Quarta causa de morte nos EUA (na frente de doenças pulmonares, diabetes, AIDS, acidentes automobilísticos • RAM ambulatorial – incidência não estimada • RAM em clínicas para idosos – 350 mil por ano Custos associados a RAM • 136 bilhões de US$ anualmente • Maior do que custos com moléstias cardiovasculares ou tratamento de diabetes • RAM responsável por 20% de danos ou mortes por ano em pacientes hospitalizados • Custo hospitalar o dobro em relação a demais pacientes Por que há tantos RAM? • Dois terços de consultas médicas geram uma receita • 2.8 bilhões de receitas no ano 2000 (10 por habitante dos EUA) • RAM aumenta exponencialmente com 4 ou mais medicações Interações Medicamentosas • Representam 3-5% das internações de RAM que podem ser evitadas • Importante causa no número de atendimentos ambulatórios Por que há tantos RAM? • Dois terços de consultas médicas geram uma receita • 2.8 bilhões de receitas no ano 2000 (10 por habitante dos EUA) • RAM aumenta exponencialmente com 4 ou mais medicações Reported serious events vs outpatient prescriptions, 1998-2005. Serious Adverse Drug Events Reported to the Food and Drug Administration, 1998-2005 - ARCH INTERN MED/VOL 167 (NO. 16), SEP 10, 2007 Estados Unidos - Idosos Creatinine clearance and drug prescriptions for the elderly. A study of 419 patients older than 70 years admitted through the emergency department Viallon A, Guyomarch P, Marjollet O, Belin M, Robert F, Berger C, Guyomarch S, Bertrand JC. Service d'Urgence et de Reanimation, Hopital Bellevue, Saint-Etienne. alain.viallon@univ-st-etienne.fr INTRODUCTION: The incidence of drug-related adverse events increases with age. In approximately 20% of cases, these events necessitate hospitalization. By taking into account the physiological changes associated with aging when prescribing drugs, physicians can prevent some of these events. The objective of this study was to analyze the prescriptions written by general practitioners for elderly patients admitted to the emergency department in relation to the patient's creatinine clearance. PATIENTS AND METHODS: Of 968 consecutive patients older than 70 years, 419 underwent a plasma creatinine assay on admission and were included in this study. Creatinine clearance was calculated with Cockcroft's formula. The patients were classified into two groups according to creatinine clearance:<30 mL/min (group I) and >or=30 mL/min (group II). RESULTS: Creatinine clearance was<30 mL/min in 84 of the 419 patients (group I) and >or=30 mL/min in 335 (group II). Mean age was significantly higher in group I than in group II (87 +/- 6 vs 81 +/- 6 years, p<0.001), as was mean plasma creatinine concentration (113 +/- 23 vs 83 +/- 19 mmol/L, p<0.001), while mean weight was significantly lower (57 +/- 10 vs 69 +/- 13 kg, p<0.001. In group I, 82 drugs with precautions concerning renal function had been prescribed for 69 (82%) patients, and in group II, 331 such drugs for 174 Of the 82 drugs prescribed in group I that required precaution, 47 (57%) were contraindicated or prescribed at an inappropriate dose in view of the creatinine clearance. Irrespective of (52%) patients. pharmacokinetic parameters, the mean number of drugs taken per patient was 5 +/- 2 in group I and 6 +/-2 in group II. CONCLUSION: In prescribing drugs for elderly patients, especially those whose weight is low, careful attention should be paid to renal function. Am J Geriatr Pharmacother. 2010 Dec;8(6):562-70. Incident use and outcomes associated with potentially inappropriate medication use in older adults. Dedhiya SD, Hancock E, Craig BA, Doebbeling CC, Thomas J 3rd. Source School of Pharmacy and Pharmaceutical Sciences, Purdue University, West Lafayette, Indiana, USA. Abstract BACKGROUND: Most studies of potentially inappropriate medication (PIM) use among older adults have focused on prevalence rather than incidence. OBJECTIVES: The goals of this study were to determine the 1-year incidence of PIM use among elderly Indiana Medicaid residents of nursing homes and to examine associations between incident PIM use and hospitalization and mortality. METHODS: A retrospective analysis was conducted using Indiana Medicaid enrollment and administrative claims files. Individuals were included if they were Medicaid eligible and aged ≥65 years as of January 2003 and received nursing home services in each month of 2003 or until death in 2003. Individuals also had to receive nursing home services from October 2002 through December 2002 for inclusion in the sample. To focus analysis on incident PIM use, individuals who received any PIM prescription medication from October 2002 through December 2002 were excluded from the sample, as were those not prescribed any new medication in 2003. PIMs were identified using the 2003 Beers criteria. Associations between incident PIM use and hospitalization and mortality were assessed using logistic regression models after controlling for other risk factors. Potential selection bias was examined using bivariate probit models. RESULTS: The study sample consisted of 7594 individuals (mean age, 83.07 years). A majority of the sample was female (76.5%), white (89.7%), and widowed (58.8%). Most individuals received care in nursing homes located in urban areas (5306 [69.9%]) and in the central region of Indiana (2838 [37.4%]). One-year incidence of PIM use was 42.1%. Incident PIM users were more likely to be hospitalized (odds ratio [OR] = 1.27; 95% CI, 1.10-C1.46) and more likely to die (OR = 1.46; 95% CI, 1.31-C1.62) in the 12 months after first receiving a PIM than nonusers, even after adjusting for demographic and clinical risk factors. CONCLUSIONS: Incident PIM use was high among these elderly Indiana Medicaid residents of nursing homes. Individuals who began use of a PIM were at a higher risk of hospitalization and of dying. Comment. Advances in critical care medicine have led to a greater number of elderly ICU survivors. These survivors experience polypharmacy and numerous transitions in care during hospitalization and are at high risk of adverse drug effects after hospital discharge. In the present study, 85% of elderly ICU survivors were discharged from the hospital with 1 or more PIM. A unique aspect of our study, and a concerning finding, was that more than half of these patients were discharged with 1 or more AIM, medications deemed more harmful than beneficial to the patient. Similarly, Hajjar et al found that 44% of elderly veterans were prescribed at least 1 AIM at hospital discharge. Inappropriate prescribing in an older ED population • Fredric M. Hustey MD*, Nicole Wallis MD, Jonathan Miller MD Department of Emergency Medicine, Cleveland Clinic, Cleveland, OH 44195, USA Cleveland Clinic Lerner College of Medicine, Case Western Reserve University, Cleveland, OH 44195, USA Department of Emergency Medicine, MetroHealth Medica • American Journal of Emergency Medicine (2007) 25, 804–807 Inappropriate prescribing in an older ED population • The objective of this study was to determine the prevalence of potentially inappropriate medication (PIMs) use in older emergency department (ED) patients based on the updated 2002 Beers criteria. This was a retrospective analysis of 352 consecutive ED visits by patients aged 65 years and older. The mean number of medications taken was 8.4 per patient. In the study population, 111 (32%; 95% confidence interval [CI], 27-36) of 352 patients were taking at least 1 PIM at ED presentation. Inappropriate prescribing in an older ED population • Among 101 of 193 patients discharged home from the ED with a new prescription, 13 (13%; 95% CI, 6-19) were also given PIMs. Inappropriate prescribing in the elderly • Journal of Clinical Pharmacy and Therapeutics (2007) 32, 113–121 Inappropriate prescribing in the elderly • Prescription of potentially inappropriate medications to older people is highly prevalent in the United States and Europe, ranging from 12% in community-dwelling elderly to 40% in nursing home residents. Australas J Ageing. 2011 Sep;30(3):124-9. doi: 10.1111/j.1741-6612.2010.00458.x. Epub 2010 Aug 19. Medication-related problems in patients referred to aged care and memory clinics at a tertiary care hospital. Elliott RA, Woodward MC. Source Pharmacy Department, Austin Health, Heidelberg. rohan.elliott@austin.org.au Abstract AIM: To investigate the prevalence of medication-related problems (MRPs) in patients attending aged care and memory disorder clinics and explore the potential role of a clinical pharmacist to obtain medication histories and identify unresolved MRPs. METHODS: The clinical pharmacist interviewed patients and reviewed their medication regimens in the outpatient clinics. Clinical significance of pharmacist-identified MRPs was rated by an independent expert panel using validated criteria. RESULTS: Forty-six patients (mean age 82 years) were reviewed. They took a median of nine medications, of which three were not recorded in the medical record. One hundred and thirteen MRPs (median 2.0 per patient) were identified by the pharmacist. Independent review rated 35% of MRPs as high or extreme risk. Thirty-seven (33%) MRPs related to medications not recorded in the medical record. CONCLUSIONS: Medication-related problems were present for most patients. Involvement of a clinical pharmacist resulted in a more comprehensive medication history and identified unresolved MRPs. Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis Jérôme Tourret, Isabelle Tostivint,1 Sophie Tézenas Du Montcel,2 Svetlana Karie,1 Vincent Launay-Vacher,1 Cécile Vigneau,3 Christel Bessette,1 Gilbert Deray,1 and Corinne Isnard Bagnis1 Nephrology and 2Biostatistics Departments, Groupe Hospitalier Pitié-Salpêtrière, and 3Nephrology Department, Hôpital Tenon, Assistance Publique-Hôpitaux de Paris, and 4INSERM U722, Université Paris 7 Denis Diderot, Site Xavier Bichat, Paris, France Clinical Infectious Diseases 2007; 45:779–84 Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis • Background. Several studies have revealed the frequency of antiretroviral (ARV) drug prescription errors. We nalyzed highly active antiretroviral therapy (HAART) prescribing practices for human immunodeficiency virus (HIV)–infected patients undergoing hemodialysis in France. Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis • Methods. Prescribed ARV drug doses in our cohort (consisting of all HIV-infected patients who underwent hemodialysis from 1 January 2002 and were prospectively followed up until 1 January 2004) were compared with the recommended doses for patients undergoing hemodialysis. The log-rank test was used to compare the outcomes among different groups of treated patients. Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis • Results. One hundred seven of the 129 patients in our cohort received a total of 317 ARV drugs, 59% of which were improperly prescribed. Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis • The dosing was too low for 18% of the patients and too high for 39% of the patients. Twenty-eight patients (26%) did not receive any of their ARV drugs at the recommended dose. Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis • Among the patients who received HAART, those who were prescribed an insufficient dose of a PI were not statistically distinguishable from the others in terms of age, sex, ethnicity, diabetic comorbidity, HIVassociated nephropathy diagnosis, hepatitis B virus and/or hepatitis C virus coinfections, duration of dialysis, and duration of HIV infection. Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis No underprescribed PI Proportion of patients who survived 1.00 0.75 Underprescribed PI 0.50 0.25 0.00 0 No. Of patients at risk Underprescribed PI 30 No underprescribed PI 66 6 28 66 12 18 24 Time, months 24 23 63 62 23 60 Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis - HIV/AIDS • CID 2007:45 (15 September) Antiretroviral Drug Dosing Errors in HIV-Infected Patients Undergoing Hemodialysis • For dialyzable ARV drugs, the delay between ARV drug receipt by the patients and dialysis sessions was not respected in 9% of cases, and in 73% of cases, it was not known whether the patients took the ARV drugs before or after dialysis sessions. HIV Med. 2011 Sep;12(8):494-9. doi: 10.1111/j.1468-1293.2011.00915.x. Epub 2011 Mar 13. Evaluation of antiretroviral-related errors and interventions by the clinical pharmacist in hospitalized HIV-infected patients. Carcelero E, Tuset M, Martin M, De Lazzari E, Codina C, Miró J, Gatell J. Source Department of Pharmacy, Hospital Clinic, Barcelona, Spain. ecarcelero@yahoo.es Abstract OBJECTIVES: The aim of the study was to identify antiretroviral-related errors in the prescribing of medication to HIV-infected inpatients and to ascertain the degree of acceptance of the pharmacist's interventions. METHODS: An observational, prospective, 1-year study was conducted in a 750-bed tertiary-care teaching hospital by a pharmacist trained in HIV pharmacotherapy. Interactions with antiretrovirals were checked for contraindicated combinations. Inpatient antiretroviral prescriptions were compared with outpatient dispensing records for reconciliation. Renal and hepatic function was monitored to determine the need for dose adjustments. RESULTS: The prescriptions for 247 admissions (189 patients) were reviewed. Sixty antiretroviral-related problems were identified in 41 patients (21.7%). The most common problem was contraindicated combinations (n=20; 33.3%), followed by incorrect dose (n=10; 16.7%), dose omission (n=9; 15%), lack of dosage reduction in patients with renal or hepatic impairment (n=6; 10% and n=1; 1.7%, respectively), omission of an antiretroviral (n=6; 10%), addition of an alternative antiretroviral (n=5; 8.3%) and incorrect schedule according to outpatient treatment (n=3; 5%). Fifteen out of 20 errors were made during admission. A multivariate analysis showed that factors associated with an increased risk of antiretroviral-related problems included renal impairment [odds ratio (OR) 3.95; 95% confidence interval (CI) 1.39-11.23], treatment with atazanavir (OR 3.53; 95% CI 1.61-7.76) and admission to a unit other than an infectious diseases unit (OR 2.50; 95% CI 1.28-4.88). Use of a nonnucleoside reverse transcriptase inhibitor was a protective factor (OR 0.33; 95% CI 0.13-0.81). Ninety-two per cent of the pharmacist's interventions were accepted. CONCLUSION: Antiretroviral-related errors affected more than one-in-five patients. The most common causes of error were contraindicated or not recommended drug-drug combinations and dose-related errors. A clinical pharmacist trained in HIV pharmacotherapy could help to detect errors and reduce the duration of their effect. Pharmacoeconomics. 2010;28(1):23-34. The cost and incidence of prescribing errors among privately insured HIV patients. Hellinger FJ, Encinosa WE. Center for Delivery, Organization, and Markets, Agency for Healthcare Research and Quality, Rockville, Maryland 20850, USA. BACKGROUND: With the rapid growth in the volume of HIV-related studies that address drug interactions, appropriate medication regimens, and when and how to alter drug regimens, it is challenging for physicians to stay informed. Physicians require knowledge about all drugs taken by HIV patients in order to assess accurately the benefits and risks of various drug combinations. OBJECTIVE: To examine the cost and frequency of antiretroviral prescribing errors among a sample of privately insured patients with HIV disease. METHODS: Data were obtained from the MarketScan Commercial Claims and Encounter Database created by the Medstat Group Inc. The MarketScan database contains claims data for inpatient care, outpatient care, physician services and prescription drugs in benefit plans sponsored by >50 large employers in the US. This study compared data from the 1999-2000 MarketScan database with those from the 2005 MarketScan database. The 2005 MarketScan database includes 12,226 HIV enrollees who received antiretroviral drugs. This study compared the claims experience of HIV patients who filled a prescription for a drug combination that is not recommended by the US Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents with the claims experience of patients who did not receive such a prescription. RESULTS: In the 1999-2000 database the most common inappropriate drug combination involved the coadministration of a protease inhibitor (PI) and the lipid-lowering drug simvastatin, and 1% of patients experienced this type of error. In the 2005 database, only 0.4% of patients (46 of 12,226) experienced an inappropriate combination of simvastatin and a PI while 5.3% of patients (644 of 12,226) received atazanavir and tenofovir without ritonavir (referred to herein as 'boosting errors'). Patients who experienced a boosting error incurred higher annual costs than patients who took ritonavir along with tenofovir and atazanavir ($US 20,927 vs $US 16,704). Because atazanavir was approved by the US FDA in June 2003, medication errors involving atazanavir were not relevant in 1999 and 2000. Overall, it was found that HIV patients were three times as likely to experience an inappropriate drug combination in 2005 than they were in either 1999 or 2000 (5.9% vs 1.9%), and that this increase is attributable to boosting errors. In addition, the prevalence rate of HIV in the 2005 MarketScan database was almost triple that in the 1999 MarketScan database (0.14% vs 0.05%). CONCLUSION: This study indicates that those who provide care to HIV patients must be vigilant in their efforts to provide patients with a drug therapy regimen that minimizes the chance of an adverse reaction and maximizes the potential to control viral replication. Prehosp Emerg Care. 2012 Jan;16(1):59-66. Epub 2011 Oct 14. Medication dosing errors in pediatric patients treated by emergency medical services. Hoyle JD, Davis AT, Putman KK, Trytko JA, Fales WD. Source Emergency Department, Helen DeVos Children's Hospital/Michigan State University College of Human Medicine, Grand Rapids, Michigan 49503, USA. jdhoyle@hotmail.com Abstract BAKGROUND: Medication dosing errors occur in up to 17.8% of hospitalized children. There are limited data to describe pediatric medication errors by emergency medical services (EMS) paramedics. It has been shown that paramedics have infrequent encounters with pediatric patients. OBJECTIVE: To characterize medication dosing errors in children treated by EMS. METHODS: We studied patients aged ≤11 years who were treated by paramedics from eight Michigan EMS agencies from January 2004 through March 2006. We defined a medication dosing error as ≥20% deviation from the weight-appropriate dose, as determined by the patient's reported weight in the prehospital medical record or by use of the Broselow-Luten tape (BLT). We studied errors in administering six EMS medications commonly given to children: albuterol, atropine, dextrose, diphenhydramine, epinephrine, and naloxone. RESULTS: There were 5,547 children aged ≤11 years who were treated during the study period, of whom 230 (4.1%) received drugs and had a documented weight. These patients received a total of 360 medication administrations. Multiple drug administrations occurred in 73 cases. Medication dosing errors occurred in 125 of the 360 drug administrations (34.7%; 95% confidence interval [CI] 30.0, 39.8). Relative drug dosage errors (with 95% CI) were as follows: albuterol 23.3% (18.4, 29.1), atropine 48.8% (34.3, 63.5), diphenhydramine 53.8% (29.1, 76.8), and epinephrine 60.9% (49.9, 73.9). The mean error (± standard deviation) for intravenous/intraosseous 1:1000 epinephrine overdoses was 808% ± 428%. The mean error (± standard deviation) for intravenous/intraosseous 1:1000 epinephrine underdoses was 35.5% ± 27.4%. CONCLUSIONS: Medications delivered in the prehospital care of children were frequently administered outside of the proper dose range when compared with patient weights recorded in the prehospital medical record. EMS systems should develop strategies to reduce pediatric medication dosing errors. Arch Dis Child. 2010 Feb;95(2):113-8. Epub 2010 Feb 4. The incidence and nature of prescribing and medication administration errors in paediatric inpatients. Ghaleb MA, Barber N, Franklin BD, Wong IC. Department of Practice and Policy, The School of Pharmacy, University of Hertfordshire, Hatfield AL10 9AB, UK; m.ghaleb@herts.ac.uk. Objectives To determine the incidence and nature of prescribing and medication administration errors in paediatric inpatients. Design Prospective review of drug charts to identify prescribing errors and prospective observation of nurses preparing and administering drugs to identify medication administration errors. In addition, incident reports were collected for each ward studied. Participants Paediatric patients admitted to hospitals and nurses administering medications to these patients. Setting 11 wards (prescribing errors) and 10 wards (medication administration errors) across five hospitals (one specialist children's teaching hospital, one nonteaching hospital and three teaching hospitals) in the London area (UK). Main outcome measures Number, types and incidence of prescribing and medication administration errors, using practitioner-based definitions. Results 391 prescribing errors were identified, giving an overall prescribing error rate of 13.2% of medication orders (95% CI 12.0 to 14.5). There was great variation in prescribing error rates between wards. Incomplete prescriptions were the most common type of prescribing error, and dosing errors the third most common. 429 medication administration errors were identified; giving an overall incidence of 19.1% (95% CI 17.5% to 20.7%) erroneous administrations. Errors in drug preparation were the most common, followed by incorrect rates of intravenous administration. Conclusions Prescribing and medication administration errors are not uncommon in paediatrics, partly as a result of the extra challenges in prescribing and administering medication to this patient group. The causes and extent of these errors need to be explored locally and improvement strategies pursued. . Intravenous Acetaminophen in the United States: Iatrogenic Dosing Errors. Pediatrics. 2012 Jan 23 Dart RC, Rumack BH. Source aRocky Mountain Poison and Drug Center, Denver Health, Denver, Colorado; Abstract An intravenous formulation of acetaminophen was introduced to the United States in 2011. Experience from Europe indicates that serious dosing errors are likely to occur. Most events have involved a 10-fold dosing error in small children caused by calculating the dosage in milligrams, but then administering the solution in milliliters. The solution is 10 mg/mL; therefore, a 10-fold overdose occurs. Evaluation of overdose with the intravenous formulation is similar to oral overdose. A serum acetaminophen concentration should be drawn 4 hours after the infusion was started or as soon thereafter as possible. If the serum acetaminophen concentration plots above the treatment line on the Rumack-Matthew nomogram, treatment with acetylcysteine should be initiated. Health care providers are encouraged to contact their regional poison center (1-800-222-1222 begin_of_the_skype_highlighting 1-800-222-1222 end_of_the_skype_highlighting) so that dosing errors will be reported, and the experience with this new product can be accumulated. Pharm World Sci. 2010 Feb;32(1):59-65. Epub 2009 Oct 17. Detection of prescription errors by a unit-based clinical pharmacist in a nephrology ward. Vessal G. Department of Clinical Pharmacy, Faculty of Pharmacy, Shiraz University of Medical Sciences, Shiraz, Iran. OBJECTIVE: To determine the impact of a clinical pharmacist on detection and prevention of prescription errors at the nephrology ward of a referral hospital. SETTING: Nephrology ward of a major referral hospital in Southern Iran. METHOD: During a 4-month period, a clinical pharmacist was assigned to review medication order sheets and drug orders three times a week at the nephrology ward. Besides chart review, the clinical pharmacist participated in medical rounds once a week. The occurrence of prescribing errors, and related harm was determined on hospitalized patients in this ward during the 4 month period. When an error was detected, intervention was made after agreement of the attending physician. MAIN OUTCOME MEASURES: Number and types of prescribing errors, level of harm, and number of interventions were determined. RESULTS: Seventy six patient charts were reviewed during the 4-month period. A total of 818 medications were ordered in these patients. Eighty six prescribing errors were detected in 46 hospital admissions. The mean age of the patients was 47.7 +/- 17.2. Fifty five percent were male while 45% were female. Different types of prescribing errors and their frequencies were as follows: wrong frequency (37.2%), wrong drug selection (19.8%), overdose (12.8%), failure to discontinue (10.5%), failure to order (7 %), under- dose (3.5%), wrong time (3.5%), monitoring (3.5%), wrong route (1.2%), and drug interaction (1.2 %). The attending physician agreed to 96.5% of the prescription errors detected, and interventions were made. Although 89.5% of the detected errors caused no harm, 4(4.7%) of the errors increased the need for monitoring, 2 (2.3%) increased length of stay, and 2 (2.3%) led to permanent patient harm. CONCLUSION: presence of a clinical pharmacist at the nephrology ward helps in early detection of prescription errors, and therefore potential prevention of negative consequences due to drug administration. Ann Transplant. 2009 Oct-Dec;14(4):58-60. Dose switch to another dosage form of Neoral increase the risk of medication error? Fahimi F, Baniasadi S, Najafi Zadeh K. Clinical Pharmacy Department, Pharmacy School, Shahid Beheshti University, M.C., Tehran, Iran. BACKGROUND: One of the most significant ways to avoid medication errors is to study the errors that have occurred in other institutions and to use the information to prevent similar accidents at other practice sites. CASE REPORT: We report a cyclosporine overdose that was caused, in part, by misinterpretation of the medication order of a transplanted patient. In transplantation regimen, a 15 mg BID dose of cyclosporine was supposed to be given as part of the immunosuppressive therapy. Unfortunately the patient received a total of 1500 mg but survived the overdose. CONCLUSIONS: This case should be considered in the development of strategies to prevent unfavorable outcomes resulting from such errors. Revista da Sociedade Brasileira de Medicina Tropical 44(2):252-253, mar-abr, 2011 Superdosagem da vacina 17DD contra febre amarela, em uma região do sul do Brasil Overdose of yellow fever vaccine in the Southern region of Brazil Marcelo Carneiro1,2, Beanir da Silva Lara3, Betina Schimidt4 e Lediana Gais4,5 Entre março e abril de 2009, ou seja, entre a 9ª e 17ª semana epidemiológica, na vigência do surto de FA silvestre, notificou-se a ocorrência da aplicação inadvertida de 10 vezes a dose padronizada da vacina 17DD contra FA, da Bio-Manguinhos, devido a troca de diluente, na região de Santa Cruz do Sul, RS. O lote da vacina foi 089VFB020Z e o do diluente foi 083DFA020Z. J Med Assoc Thai. 2011 Feb;94 Suppl 1:S258-63. Inadvertent intrathecal vincristine administration: report of a fatal case despite cerebrospinal fluid lavage and a review of the literature. Pongudom S, Chinthammitr Y. Source Department of Medicine, Udonthani Hospital, Udonthani, Thailand. jangth172@yahoo.com Abstract Accidental intrathecal vincristine administration results in progressive ascending radiculomyeloencephalopathy usually leading to fatal outcome. No specific therapy for intrathecal vincristine toxicity has been reported. We report a 63-year-old man with diffuse large B-cell lymphoma at the right testis who inadvertently received intrathecal vincristine. Direct CSF aspiration and irrigation was done 30 minutes after the incident. Ventriculostomy and lumbar drain was placed. Intrathecal irrigation was started at 6.5 hours using FFP-containing lactate solution and continued for 11 days. In addition, antineurotoxic and neuroprotective agents were given. His neurological symptom deteriorated slowly and he died on day 12. Among 16 reported cases undergoing lumbar drainage and/or irrigation, 56.3% can survive 30 days or more and 37.5% had survive more than 6 months. Immediate CSF drainage and early irrigation is related to good outcome (prolonged survival with no encephalopathy). In our case, his poor outcome might be due to the delayed starting of irrigation. In conclusion, the appropriate and effective management of this complication is unknown. However, emergency cerebrospinal fluid drainage and irrigation remains the principal of management. J Cataract Refract Surg. 2011 Jun;37(6):1168-9. Macular infarction after inadvertent intracameral cefuroxime. Qureshi F, Clark D. Source From the Aintree University Hospital, Liverpool, United Kingdom. Abstract We present the case of a 70-year-old patient who had uneventful cataract surgery. Because of a procedural mishap, the patient received an excess dose of intracameral cefuroxime of approximately 62.5 mg. Two weeks postoperatively, evidence of macular infarction with cystoid macular edema was seen on fundus fluorescein angiography. The patient was treated with 4.0 mg of intravitreal triamcinolone, but the visual acuity failed to improve; the final pinhole acuity was 3/60. Based on the postoperative progress, we speculate that a delayed mechanism of vascular toxicity is implicated. The importance of systematic procedures to reduce the risk for mistakes is emphasized, especially for a procedure such as cataract surgery where efficiency is increasingly important. FINANCIAL DISCLOSURE: Neither author has a financial or proprietary interest in any material or method mentioned. J Patient Saf. 2009 Mar;5(1):16-22. Incidence of adverse drug events and medication errors in intensive care units: a prospective multicenter study. Benkirane RR, R-Abouqal R, Haimeur CC, S Ech Cherif El Kettani SS, Azzouzi AA, M'daghri Alaoui AA, Thimou AA, Nejmi MM, Maazouzi WW, Madani NN, R-Edwards I, Soulaymani RR. Moroccan Pharmacovigilance Centre, Rabat, Marocco BACKGROUND: In recent years, medication error has received considerable attention because it causes substantial mortality, morbidity, and additional health care costs. Collecting information in this field depends on the willingness of health professionals to report their errors. Another important point is to identify patients at high risk for an adverse drug event (ADE) to oversee the quality of the entire drug distribution chain, including prescription, drug choice, dispensing, and preparation to the administration of drugs. OBJECTIVE: To assess the prevalence rate of ADEs. To ascertain those related to medication errors to develop prevention strategies. DESIGN: Prospective cohort study. SETTING: Multicenter study, 7 intensive care unit in academic and military hospital of Rabat. PERIOD: Three months. PATIENTS: Adult and pediatric patients in medical/surgical intensive care units. COLLECTION DATA: One coordinator for each participating ward collaborates with a pharmacist investigator from Moroccan pharmacovigilance center in the detection of ADEs. MEASUREMENTS AND MAIN RESULTS: Of the 696 patients studied, the investigators identified 108 incidents (15.5 %) (95% confidence interval, 14.1-16.9). The reviewers concluded that 56 (70%) of 80 ADEs were nonpreventable, which, by definition, are considered as ADRs. Among the 52 medication errors, 28 (53.8%) led to potential ADEs and 24 (46.2%) led to actual preventable ADEs. There were 7.7 medication errors for 1000 patient-days. We noted that the preventable ADEs occurred in the prescribing (71.1%), administration (21.2%), transcription (5.7%), and dispensing stages. Errors of wrong or improper drug use accounted for the majority of potential and actual preventable ADEs (23%), followed by improper dose (21.1%), wrong duration of treatment (19.2%),wrong rate of administration(13.5), errors due to drug omission (9.6%), wrong administration technique (5.8%), wrong dosage form (3.8%), and wrong administration timing (1.9%). CONCLUSIONS: This study argues the need for pharmacovigilance to extend its scope to medication errors to improve the safety of drugs. Our results underlined that medication errors are likely to be more serious than ADRs. Our approach based on the collaboration between the pharmacovigilance center and clinicians can be a powerful tool for incorporating error reporting into the culture of medicine. J Am Geriatr Soc. 2011 Nov;59(11):2139-44. doi: 10.1111/j.1532-5415.2011.03567.x. Epub 2011 Aug 30. Inappropriate medication use in older adults undergoing surgery: a national study. Finlayson E, Maselli J, Steinman MA, Rothberg MB, Lindenauer PK, Auerbach AD. Source Department of Surgery, University of California, San Francisco, CA, USA. emily.finlayson@ucsfmedctr.org Abstract OBJECTIVES: To determine the prevalence and factors associated with use of potentially inappropriate medications (PIMs) in older adults undergoing surgery. DESIGN: Retrospective cohort study. SETTING: Three hundred seventy-nine acute care hospitals participating in the nationally representative Perspective database (2006-2008). PARTICIPANTS: Individuals aged 65 and older undergoing major inpatient gastrointestinal, gynecological, urological, and orthopedic surgery (N=272,351). MEASUREMENTS: Medications were classified as PIMs using previously published criteria defining 33 medications deemed potentially inappropriate in people aged 65 and older. Information about participant and provider characteristics and administration of PIMs was obtained from hospital discharge file data. Logistic regression techniques were used to examine factors associated with use of PIMs in the perioperative period. RESULTS: One-quarter of participants received at least one PIM during their surgical admission. Meperidine was the most frequently prescribed PIM (37,855, 14% of participants). In adjusted analysis, PIM use was less likely as age advanced (adjusted odds ratio (AOR)=0.98 per year of age, 95% confidence interval (CI)=0.97-0.98) and in men (AOR=0.83, 95% CI=0.81-0.85). PIMs were more likely to be prescribed to participants cared for by orthopedic surgeons than for those cared for by general surgeons (AOR=1.22, 95% CI=1.08-1.40). Participants undergoing surgery in the West (AOR=1.79, 95% CI=1.02-3.16) and South (AOR=2.24, 95% CI=1.38-3.64) were more likely to receive a PIM than those in the Northeast. CONCLUSION: Receipt of PIMs in older adults undergoing surgery is common and varies widely between providers and geographic regions and according to participant characteristics. Interventions aimed at reducing the use of PIMs in the perioperative period should be considered in quality improvement efforts. Continuação BMJ. 2011 Sep 22;343:d5543. doi: 10.1136/bmj.d5543. Multimodal system designed to reduce errors in recording and administration of drugs in anaesthesia: prospective randomised clinical evaluation. Merry AF, Webster CS, Hannam J, Mitchell SJ, Henderson R, Reid P, Edwards KE, Jardim A, Pak N, Cooper J, Hopley L, Frampton C, Short TG. MAIN OUTCOME MEASURES: Primary: composite of errors in the recording and administration of intravenous drugs detected by direct observation and by detailed reconciliation of the contents of used drug vials against recorded administrations; and lapses in responding to an intermittent visual stimulus (vigilance latency task). Secondary: outcomes in patients; analyses of anaesthetists' tasks and assessments of workload; evaluation of the legibility of anaesthetic records; evaluation of compliance with the procedural rules of the new system; and questionnaire based ratings of the respective systems by participants. RESULTS: The overall mean rate of drug errors per 100 administrations was 9.1 (95% confidence interval 6.9 to 11.4) with the new system (one in 11 administrations) and 11.6 (9.3 to 13.9) with conventional methods (one in nine administrations) (P = 0.045 for difference). Most were recording errors, and, though fewer drug administration errors occurred with the new system, the comparison with conventional methods did not reach significance. Rates of errors in drug administration were lower when anaesthetists consistently applied two key principles of the new system (scanning the drug barcode before administering each drug and keeping the voice prompt active) than when they did not: mean 6.0 (3.1 to 8.8) errors per 100 administrations v 9.7 (8.4 to 11.1) respectively (P = 0.004). Lapses in the vigilance latency task occurred in 12% (58/471) of cases with the new system and 9% (40/473) with conventional methods (P = 0.052). The records generated by the new system were more legible, and anaesthetists preferred the new system, particularly in relation to long, complex, and emergency cases. There were no differences between new and conventional systems in respect of outcomes in patients or anaesthetists' workload. CONCLUSIONS: The new system was associated with a reduction in errors in the recording and administration of drugs in anaesthesia, attributable mainly to a reduction in recording errors. Automatic compilation of the anaesthetic record increased legibility but also increased lapses in a vigilance latency task and decreased time spent watching monitors. Trial registration Australian New Zealand Clinical Trials Registry No 12608000068369. Int J Clin Pharmacol Ther. 2011 Aug;49(8):500-9. Pharmaco-epidemiologic study of the prescription of contraindicated drugs in a primary care setting of a university: a retrospective review of drug prescription. Dhabali AA, Awang R, Zyoud SH. Source WHO Collaborating Centre for Drug Information, National Poison Centre, Universiti Sains Malaysia (USM), Penang, Malaysia. dahbali@yahoo.com Abstract BACKGROUND: The prescription of contraindicated drugs is a preventable medication error, which can cause morbidity and mortality. Recent data on the factors associated with drug contraindications (DCIs) is limited world-wide, especially in Malaysia. AIMS: The objectives of this study are 1) to quantify the prevalence of DCIs in a primary care setting at a Malaysian University; 2) to identify patient characteristics associated with increased DCI episodes, and 3) to identify associated factors for these DCIs. METHODS: We retrospectively collected data from 1 academic year using computerized databases at the Universiti Sains Malaysia (USM) from patients of USM's primary care. Descriptive and comparative statistics were used to characterize DCIs. RESULTS: There were 1,317 DCIs during the study period. These were observed in a cohort of 923 patients, out of a total of 17,288 patients, representing 5,339 DCIs per 100,000 patients, or 5.3% of all patients over a 1-year period. Of the 923 exposed patients, 745 (80.7%) were exposed to 1 DCI event, 92 (10%) to 2 DCI events, 35 (3.8%) to 3 DCI events, 18 (2%) to 4 DCI events, and 33 patients (3.6%) were exposed to 5 or more DCI events. The average age of the exposed patients was 30.7 ± 15 y, and 51.5% were male. Multivariate logistic regression analysis revealed that being male (OR = 1.3; 95% CI = 1.1 - 1.5; p < 0.001), being a member of the staff (OR = 3; 95% CI = 2.5 - 3.7; p < 0.001), having 4 or more prescribers (OR = 2.8; 95% CI = 2.2 - 3.6; p < 0.001), and having 4 or more longterm therapeutic groups (OR = 2.3; 95%CI = 1.7 - 3.1; p < 0.001), were significantly associated with increased chance of exposure to DCIs. DISCUSSION AND CONCLUSIONS: This is the first study in Malaysia that presents data on the prevalence of DCIs. The prescription of contraindicated drugs was found to be frequent in this primary care setting. Exposure to DCI events was associated with specific socio-demographic and health status factors. Further research is needed to evaluate the relationship between health outcomes and the exposure to DCIs. Spine (Phila Pa 1976). 2008 Jan 1;33(1):104-7. Towards the reduction of medication errors in orthopedics and spinal surgery: outcomes using a pharmacist-led approach. Weiner BK, Venarske J, Yu M, Mathis K. Source Division of Spinal Surgery, Department of Orthopaedic Surgery, The Methodist Hospital, Houston, TX 77030, USA. bkweiner@tmh.tmc.edu Abstract STUDY DESIGN: Evaluation of medication ordering errors discovered on an orthopedic/spinal in-patient hospital unit and efforts initiated to reduce them. OBJECTIVE.: In this study the authors aimed to assess the frequency of medication ordering errors and to examine the impact of local measures set forth to reduce their occurrence. SUMMARY OF BACKGROUND DATA: Since the release of the 2000 Institute of Health report: "To Err is Human"; in-hospital medical errors have been recognized as being unacceptably high; the consequence being preventable death rates estimated near 125,000 patients per year. The most common of errors are those involving medications. METHODS: The study consisted of 2 parts. In part 1, the charts from 82 consecutive patients admitted to the Orthopedic/Spine Surgical Unit were assessed to determine the frequency, type, and potential severity of medication ordering errors. Several programs to reduce such errors were subsequently instituted and included: improved chart surveillance by pharmacists, a newly developed medication/history form given to and reviewed with patients before surgery, in-service education of preoperative nursing staff, patient database form changes, and requests for patients to bring their medications on admission. Part 2, including 87 patients, assessed the impact of these measures. RESULTS: In part 1, medication errors were detected in 62% of orders overall. Of these, 43% were found to be of moderate or high potential for harm. After the institution of the above measures (part 2), overall errors were reduced by 31%; moderate/high risk potential harm was reduced by 64%; and errors of omission were detected twice as often. CONCLUSION: Medication errors in ordering are common in orthopedics. We found in part 1 that a chart review and patient interview by the pharmacy team can detect and correct these before reaching the patient. Furthermore, we found in part 2 that the risk could be further reduced by the implementation of pharmacist-led: patient education, education of preoperative nursing personnel, improvement of forms used for data collection, and having the patients bring all of their medications on admission. Medication dosing errors in hospitalized patients with renal impairment: a study in Palestine • Background and Aim Reduced renal function requires dose adjustment for certain drugs to avoid toxicity. The aim of this study was to determine whether appropriate dosage adjustments were made for drugs that are nephrotoxic, excreted, or metabolized (TEM medications) by the kidney in patients with renal impairment. Results A total of 78 patients had calculated creatinine clearance 59 ml/min. Those patients were prescribed a total of 1001 lines of prescription medication. Dosage adjustment was necessary for 193 TEM medications. Analysis of TEM medications with guidelines for adjustment indicated that 73.58% (142) were found to be inappropriate and 26.42% (51) were found to be appropriate. • Pharmacoepidemiology and drug safety 2007; 16: 908–912 Medication dosing errors in hospitalized patients with renal impairment: a study in Palestine • Conclusion In our study, a wide range of dosing errors was common among patients with renal impairment that was common during hospitalization. Continued medical education in the field of clinical pharmacokinetics is important for physicians. Incorrect use of orlistat and sibutramine in clinical practice • To investigate how the antiobesity drugs orlistat and sibutramin are prescribed in relation to the approved indications and the Swedish subsidiary rules. Eur J Clin Pharmacol (2007) 63:205–209 Incorrect use of orlistat and sibutramine in clinical practice • Methods - Anonymous survey to prescribers of a random sample of 2000 out of 20,000 prescription of orlistat and sibutramin. Incorrect use of orlistat and sibutramine in clinical practice • Results - The response rate was around 65%. About half of the patients were not treated in accordance with the approved indications and a fourth of the patients prescribed sibutramin had one or several contraindications to the drug. The subsidiary rules were not followed in the majority of cases. Incorrect use of orlistat and sibutramine in clinical practice • Conclusion - Deviation from the approved indications and subsidiary criteria of orlistat and sibutramin is a question of waste of medical and economic resources. Prescribing of sibutramin to patients with contraindications is a serious health hazard. J Am Geriatr Soc. 2011 Aug;59(8):1412-20. doi: 10.1111/j.1532-5415.2011.03522.x. Epub 2011 Aug 8. Potential underuse, overuse, and inappropriate use of antidepressants in older veteran nursing home residents. Hanlon JT, Wang X, Castle NG, Stone RA, Handler SM, Semla TP, Pugh MJ, Berlowitz DR, Dysken MW. Source Geriatric Research, Education and Clinical Center, and Center for Health Equity Research and Promotion, Veterans Affairs Pittsburgh Health System, Pittsburgh, Pennsylvania, USA. jth14@pitt.edu Abstract OBJECTIVES: To examine prevalence and resident- and site-level factors associated with potential underuse, overuse, and inappropriate use of antidepressants in older Veterans Affairs (VA) Community Living Center (CLC) residents. DESIGN: Longitudinal study. SETTING: One hundred thirty-three VA CLCs. PARTICIPANTS: Three thousand six hundred ninety-two veterans aged 65 and older admitted between January 1, 2004, and June 3, 2005, with long stays (≥ 90 days). MEASUREMENTS: Prevalence of potential underuse, inappropriate use, and overuse of antidepressants in residents with and without depression (as documented according to International Classification of Diseases, Ninth Revision, Clinical Modification, codes or Depression Rating Scale). RESULTS: Selective serotonin reuptake inhibitors were the most commonly prescribed antidepressant. Of the 877 residents with depression, 25.4% did not receive an antidepressant, suggesting potential underuse. Of residents with depression who received antidepressants, 57.5% had potential inappropriate use due primarily to problems seen with drug-drug and drug-disease interactions. Of the 2,815 residents who did not have depression, 1,190 (42.3%) were prescribed one or more antidepressants; only 48 (4.0%) of these had a Food and Drug Administration-approved labeled indication, suggesting potential overuse. Overall, only 17.6% of antidepressant use was appropriate (324/1,844). The only consistent resident factor associated with potential underuse and overuse use was taking an antipsychotic without evidence of schizophrenia (underuse: adjusted relative risk ratio (ARRR)=0.56, 95% confidence interval (CI)=0.33-0.94; overuse: adjusted odds ratio=1.52, 95% CI=1.21-1.91). Having moderate to severe pain (ARRR=1.54, 95% CI=1.08-2.20) and the prescribing of an anxiolytic or hypnotic (ARRR=1.33, 95% CI=1.02-1.74) increased the risk of potential inappropriate antidepressant use. CONCLUSION: Potential problems with the use of antidepressants were frequently observed in older U.S. veteran CLC residents. Future studies are needed to examine the true risks and benefits of antidepressant use in CLC and non-VA nursing homes. SSRIs Associated With Increased Fall Risk In Nursing Home Patients With Dementia. HealthDay (1/19, Preidt) reports, "Antidepressants called selective serotonin reuptake inhibitors (SSRIs) are associated with an increased risk of falls in nursing home residents with dementia," according to a study published Jan. 19 in the British Journal of Clinical Pharmacology. In 248 patients with dementia who were in nursing homes, "researchers found that the risk of having an injury-causing fall was three times higher for residents taking SSRIs than for those who didn't take the antidepressants." BBC News (1/19) also covers the story. BMC Infect Dis. 2011 Jul 5;11:187. Unnecessary use of fluoroquinolone antibiotics in hospitalized patients. Werner NL, Hecker MT, Sethi AK, Donskey CJ. Source School of Medicine, Case Western Reserve University, 10,000 Euclid Avenue, Cleveland, Ohio, USA. Abstract BACKGROUND: Fluoroquinolones are among the most commonly prescribed antimicrobials and are an important risk factor for colonization and infection with fluoroquinolone-resistant gram-negative bacilli and for Clostridium difficile infection (CDI). In this study, our aim was to determine current patterns of inappropriate fluoroquinolone prescribing among hospitalized patients, and to test the hypothesis that longer than necessary treatment durations account for a significant proportion of unnecessary fluoroquinolone use. METHODS: We conducted a 6-week prospective, observational study to determine the frequency of, reasons for, and adverse effects associated with unnecessary fluoroquinolone use in a tertiary-care academic medical center. For randomly-selected adult inpatients receiving fluoroquinolones, therapy was determined to be necessary or unnecessary based on published guidelines or standard principles of infectious diseases. Adverse effects were determined based on chart review 6 weeks after completion of therapy. RESULTS: Of 1,773 days of fluoroquinolone therapy, 690 (39%) were deemed unnecessary. The most common reasons for unnecessary therapy included administration of antimicrobials for non-infectious or non-bacterial syndromes (292 days-of-therapy) and administration of antimicrobials for longer than necessary durations (234 days-of-therapy). The most common syndrome associated with unnecessary therapy was urinary tract infection or asymptomatic bacteriuria (30% of all unnecessary days-of-therapy). Twenty-seven percent (60/227) of regimens were associated with adverse effects possibly attributable to therapy, including gastrointestinal adverse effects (14% of regimens), colonization by resistant pathogens (8% of regimens), and CDI (4% of regimens). CONCLUSIONS: In our institution, 39% of all days of fluoroquinolone therapy were unnecessary. Interventions that focus on improving adherence with current guidelines for duration of antimicrobial therapy and for management of urinary syndromes could significantly reduce overuse of fluoroquinolones. Swiss Med Wkly. 2009 Jul 25;139(29-30):430-5. Economic burden of unjustified medications at hospital discharge. Perren A, Donghi D, Marone C, Cerutti B. Intensive Care Unit, Ospedale Regionale Bellinzona e Valli, Bellinzona, Switzerland. QUESTION UNDER STUDY: Medication errors are a major concern for health care since they may cause or lead to inappropriate medication use or patient harm. However, little is known regarding the economic burden of unjustified medications. METHODS: Hospital discharge records of 577 patients were prospectively screened for the presence of unjustified medications. From this sample population, 318 (55%) were eligible and their data were used to assess the monthly costs of unjustified discharge medications, their relationship to the total and each individual's drug expenditure, and the relative cost weights of relevant unjustified drug classes. RESULTS: The results found that 619 out of 3691 prescriptions (16.8%) were unjustified. The mean (median; 95% CI) monthly costs of unjustified discharge medications were 32 euro (27 euro; 29 euro to 35 euro). The percentage of unnecessary treatments was inversely linked to the amount of total individual drug expenditure. For this collective, monthly extra costs due to unjustified medications were 18585 euro, and the relative cost weights of the relevant drug classes were 45.8% for gastrointestinal agents (33.8% for proton pump inhibitors), 17.7% for cardiovascular drugs, and 17.2% for psychiatric drugs. CONCLUSIONS: There is a considerable financial burden imposed by unjustified medications at hospital discharge. Discharge medications not motivated by appropriate diagnoses should be questioned. This study should be repeated in other institutions and in a larger population. Am J Manag Care. 2010 Sep;16(9):e228-34. Magnitude and economic effect of overuse of antisecretory therapy in the ambulatory care setting. Heidelbaugh JJ, Goldberg KL, Inadomi JM. Source Department of Family Medicine, University of Michigan, Ann Arbor, MI, USA. jheidel@umich.edu Abstract OBJECTIVES: To determine the prevalence and economic effect of inappropriate proton pump inhibitor (PPI) use in an ambulatory care setting. STUDY DESIGN: Retrospective medical record review of random sample with subgroup analysis. METHODS: Patients were categorized according to appropriateness of pharmacotherapy based on documented upper gastrointestinal tract diagnoses, gastrointestinal or extraesophageal symptoms, or gastroprotection. Adverse events potentially associated with PPI use were identified. RESULTS: Of 946 patients in an ambulatory care setting, 35.4% were given PPI therapy for an appropriately documented upper gastrointestinal tract diagnosis, 10.1% received PPIs empirically for symptomatic treatment based on extraesophageal symptoms, 18.4% received PPIs for gastroprotection, and 36.1% had no documented appropriate indication for PPI therapy. In a subgroup analysis, 48.6% of patients across all 4 categories received PPIs without documentation of reevaluation of upper gastrointestinal tract symptoms, accounting for 1034 patient-years of PPI use. The total cost of inappropriate PPI use was $233,994 based on over-the-counter PPI costs and $1,566,252 based on average wholesale price costs. Potentially related adverse events in this cohort included Clostridium difficile–associated diarrhea (6 cases) and community-acquired pneumonia (1 case), but no cases of hip fracture or vitamin B12 deficiency were identified. CONCLUSIONS: Proton pump inhibitors are often overused in the ambulatory care setting without documented valid indications. Inappropriate use of PPIs is associated with substantial cost expenditure and with the potential for adverse events. PBMs said to be pushing for "personalized" approach to prescribing medication. BusinessWeek (2010-1/22, Carey) reports that with "as much as $145 billion" being spent on medications that didn't help individual patients in 2008, the idea of targeting drugs only towards specific patients has still not been effectively implemented. However, "the promise of personalized drug treatments appears more realistic," thanks to pharmacy benefit managers (PBMs) such as Medco and CVS Caremark (CVS), which are testing patients for "genetic variations that explain why they respond differently to drugs." The article supposes that drugmakers who continue to seek the mass appeal of "blockbuster" drugs may soon encounter resistance from the FDA, which "may balk at approving drugs that can't be directed to the right patients.“ Patients Not Taking Prescribed Medicines Cost US Healthcare System $290B Yearly. The AP (1/4, Johnson) reports, "Patients not taking medicine as prescribed cost the US healthcare system roughly $290 billion a year in extra treatment and related costs, research shows. One study estimated those patients pay about $2,000 a year in extra out-of-pocket medical costs." Notably, "nearly three in four Americans don't take their prescription medicine as directed. Even among those with serious chronic health conditions such as diabetes, about one in three don't." Unfortunately, "for patients with chronic health conditions -- nearly half the US population -- not taking medications as prescribed can bring serious consequences," even premature death. Clin Drug Investig. 2011;31(5):309-16. doi: 10.2165/11586200-000000000-00000. Potential drug-drug interactions associated with prolonged stays in the intensive care unit: a retrospective cohort study. Moura C, Prado N, Acurcio F. Source Multidisciplinary Institute of Health, Federal University of Bahia, Vitria da Conquista, Brazil. csmoura@ufba.br Abstract BACKGROUND AND OBJECTIVES: Drug-drug interactions (DDIs) are one cause of adverse drug events and can cause harm to hospitalized patients. Little has been done to study the relationship between potential DDIs and an increased length of stay (LOS) in the intensive care unit (ICU). The aim of this study was to determine the frequency of potential DDIs during ICU stays and to determine whether the frequency of these adverse events was associated with ICU LOS. METHODS: This retrospective cohort study was conducted from January to December 2007 in the ICU of the General Hospital of Vitória da Conquista, Brazil. The study population comprised all patients aged >18 years admitted to the hospital's ICU. Demographic and prescription data were collected from medical files. All prescriptions administered during the period were examined. Potential DDIs were identified and classified according to the book Drug Interaction Facts. The median LOS was determined by the Kaplan-Meier method and Cox proportional hazards models were fitted to analyse the relationship between potential DDIs and the LOS. RESULTS: The study population comprised 236 adults, 158 (67%) of them men, between the ages of 18 and 96 years, with a mean ± SD age of 50 ± 20 years. The median LOS among patients with at least one DDI was 12 days compared with 5 days among those with no DDIs (p < 0.01). Multiple Cox proportional regression analyses showed that a prolonged ICU stay was positively associated with DDIs (hazard ratio [HR] 0.54; 95% CI 0.37, 0.80; p < 0.01), where an HR <1 indicates a variable that increases the risk of prolonged stay (i.e. an adverse outcome). This association was true even after controlling for the cost of hospitalization, the number of procedures and the number of prescribed drugs. CONCLUSION: In this study, DDIs were found to be associated with a longer ICU stay. Given that LOS is an important indicator of the quality of health care delivered and that DDIs are considered avoidable, specific measures are necessary to increase the recognition of DDIs. E-prescriptions and dispensing programmes associated with a DDI knowledge base can help health professionals identify hazardous drug combinations. Int J Clin Pharm. 2011 Apr;33(2):260-3. Epub 2011 Mar 15. Analysis of the quality of prescriptions at a cardiovascular ward in Brazil: a pilot study. Siqueira JS, Antoniolli AR, Silvestre CC, Oliveira-Filho AD, Silva WB, Lyra DP Jr. Source Laboratory of Teaching and Research in Social Pharmacy, Federal University of Sergipe, (DFS/UFS), LEPFS-UFS, São Cristóvão, Aracaju, Sergipe, 49000-000, Brazil. Abstract AIM OF STUDY: To analyze the quality of prescriptions in a hospital in Brazil. METHODS: A cross-sectional pilot study of the quality of prescriptions of adult patients admitted at the cardiovascular ward. Data were collected with the help of a structured form developed by the researchers based on related literature, with items about medications and completeness of prescriptions. The form was divided into four categories of prescription quality indicators: prescription type, legibility and readability of handwriting, and completeness. MAIN OUTCOME MEASURES 100 patients participated in the study, with ages between 20 and 94 years (mean of 67.12 ± 16.6 years), We analyzed 5,030 on 496 prescriptions for 100 patients. Of 11% the handwriting was considered to be less legible and 17% considered illegible. In terms of readability, a high incidence of medications were prescribed by their brand names (89%), and 13,707 abbreviations (mean of 27.6 per prescription) were used mainly to refer to the route of administration (31%), concentration (27%), and indications for use (20%). In relation to completeness, 471 (95%) prescriptions were considered incomplete, mainly medication data. CONCLUSION: The quality indicators used in this study revealed a high rate of prescription problems and errors.