Tenon's Capsule
advertisement

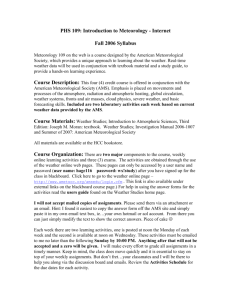
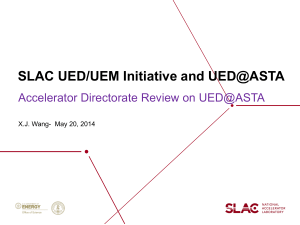
Dr S Wu. FACRRM, FRACGP Dr KC Tang. FRANZCO, Clinical lecturer School of Rural Health, University of Sydney Anterior Sub-Tenon’s Anaesthesia (ASTA) for Cataract Surgery Introduction Ocular regional blocks 1 = Anterior SubTenon’s Anaesthesia (ASTA) 2 = Steven’s subTenons Technique. 3 = Retrobulbar 4 = Peribulbar Tenon’s Capsule Like a glove for the whole eye Starts at the limbus and lid muscles Initially fused to conjunctiva Loose matrix Follows sclera around the globe Sleeves around rectus and oblique muscles Attaches to optic nerve sheaths Posterior instrumentation unnecessary for Sub-Tenon’s (ST) Block McNeela et al (2004) N=59 Successful ST blocks 6mm ultra-short cannula Kumar et al (2004) N=151 compared 3 sub-Tenon’s cannulae lengths: 25mm 18mm 12mm Sub-Tenon’s space accessed anteriorly!!! Short cannula achieved similar anaesthesia and akinesia Needle sub-Tenon’s injection Ripart et al (1996) N=151 Unlike cannula ST techniques 25G needle without dissection Medial canthus subTenon’s injection Mean depth 15-20mm 92% - total akinesia Dissection not necessary for sub-Tenon’s block Ripart (1998) CT images of fresh cadavers 9mls contrast given by MC sub-Tenon’s injection spread to: Episcleral space Optic nerve sheath Rectus muscle sheath Lid muscles- orbicularis occuli & levator palpabrae Subconjunctival space Short needle 25G 16mm Methods Case series 60 adult elective cataract patients All received ASTA by author Using 2 common local anaesthetics 30 – lignocaine 2% +hyalase 30 iu/ml 30 – bupivacaine 0.5% + lignocaine 2% + hyalase 30 iu/ml Approved by regional HERC ANZCTR Preparation Routine pre op care Supine, eye pillow ½ strength iodine Head stabilised by nurse Amethocaine 1% x1 drop Optional light sedation (midazolam) ASTA Technique Outline Lift upper lid, look down Pierce conjunctiva and Tenon’s capsule in upper outer quadrant 5-7mm from limbus Advance needle about 5mm supero-medially Following curve of sclera Visually check needle position by forming a small bleb of L.A. Inject L.A. VERY SLOWLY, guided by patient comfort Vol. 6-10mls, diff in each patient, guided by 3 signs of filling up the ST space as described by Ripart : Mod. proptosis + lid fullness + mod. chemosis At the end of ASTA injection, complete lid drop evident Excess chemosis Mostly resolves with gentle massage Akinesia Scored 10min post ASTA, using Aggregated Motility Score (AMS) Validated scale used by Kumar, MaNeela, Brahma etc Lid + Globe mvt in 4 directions: up, down, medial, lateral 0 = no mvt 1 = twitch <1mm 2 = partial mvt 3 = full mvt Total akinesia = 0, adequate akinesia < =4, max mvt = 15 Pain Rated as it occurred during operation Numeric Verbal Rating Scale 0 = no pain 1-3 = mild 4-6 = moderate 7-9 = severe 10 = worst Results Mean age 74, equal gender. All successfully completed surgery without supplemental anaesthesia No major anaesthetic complications No surgical complications due to ASTA Main complication = Sub conjunctival haemorrhage in 5% pts. 48% on warfarin or antiplatelet Rx Akinesia 10min post ASTA 18 •95% - AMS ≤4/15 16 •100% - lid paralysis : levator palpabrae and orbicularis occuli 14 12 10 Lignocaine Lignocaine/Bupivicaine 8 6 4 2 0 AMS 0 AMS 1 AMS 2 AMS 3 AMS 4 AMS 5 AMS 7 Pain during operation •58/60 pain free 35 30 •2 patients- Transient mild pain 1-2/10 25 20 Lignocaine 15 Lignocaine/bupivacaine 10 •End of procedure •No supplementation required 5 0 Pain 0 Pain 1 Pain 2 Discussion ASTA comparable to other sub-Tenons blocks Akinesia 95% AMS ≤ 4 Learning curve McNeela et al (2004) 98% AMS<4 Kumar 3 cannulae (2004) 92-100% AMS<4 Koh et al, Concord Hosp, 2005, Steven’s sub-Tenon’s block Akinesia - 88% AMS≤4 Anaesthesia – 7% needed topical amethocaine supp. ASTA - Comprehensive all-in-one block Relatively large volume Av = 9mls (similar to Ripart) One injection delivers LA to: Lid muscles, no need VII inj. Sub-conjunctival space Muscle sheaths Episcleral space Retrobulbar space Implications for Safety ASTA Anterior Visually guided Short needle Less invasive – no dissection Improve Aesthetics & healing Reduce infection Avoids vulnerable anatomy Optic and other nerves CSF Blood vessels Retina / macula Should be safer Potential Advantages Globe perforation Anterior Peripheral retina Visible Haemorrhage - anterior Seen Compressed No need to stop Warfarin or antiplatelets ?Safer in axial length ≥ 26mm Equipment is cheap & readily available – beneficial for developing nations Easily topped up anytime ?Role in patients with difficult access Previous surgery Adhesions Scleral buckles Conclusion Small study ASTA Simple Effective Safe Phaecoemulsification cataract surgery Further research to elucidate its wider application “Simplicity is achieving maximal effect with minimal means” Dr Kawana Contact: drwu@bigpond.com Zen Garden Master.