Chapter_034
advertisement

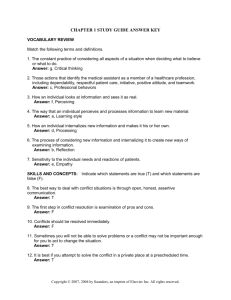
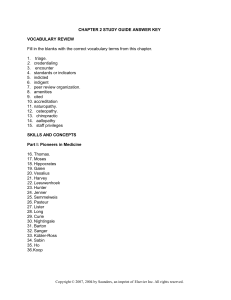
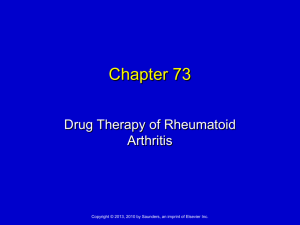
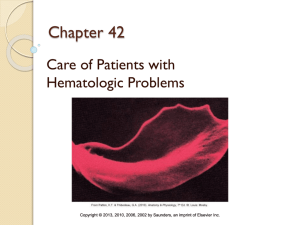
Chapter 34 Care of Critically Ill Patients with Respiratory Problems Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Chapter 34 Care of Critically Ill Patients with Respiratory Problems Learning Outcomes 1. Protect the patient receiving mechanical ventilation. 2. Ensure safe management of endotracheal tubes, tracheostomy tubes, and mechanical ventilators. 3. Identify hospitalized patients at risk for a pulmonary embolism. 4. Teach people at risk for pulmonary embolism techniques to reduce the risk. 5. Support the patient and family in coping with changes in breathing status and the need for mechanical ventilation. 6. Provide emotional support to patients experiencing acute respiratory difficulties. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Chapter 34 Care of Critically Ill Patients with Respiratory Problems Learning Outcomes (Continued) 7. Assess the respiratory status of any patient who develops sudden-onset respiratory difficulty or acute confusion. 8. Use laboratory data and clinical manifestations to evaluate the adequacy of oxygenation and ventilatory interventions. 9. Coordinate nursing care for the patient being mechanically ventilated. 10. Maintain a patent airway on anyone who has experienced chest trauma. 11. Describe a variety of conditions that result from chest trauma and their common treatments. 12. Describe critically ill patients and the related nursing interventions and rationales. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Chapter 34 Care of Critically Ill Patients with Respiratory Problems *Pulmonary embolism* Acute respiratory failure Acute respiratory distress syndrome The patient requiring intubation and ventilation Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Chapter 34 Care of Critically Ill Patients with Respiratory Problems (Continued) Chest Trauma Pulmonary contusion Rib fracture Flail chest Pneumothorax Tension pneumothorax Hemothorax Tracheobronchial trauma Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Pulmonary Embolism • Collection of particulate matter—solids, liquids, air—that enters venous circulation and lodges in pulmonary vessels • Usually occurs when blood clot from a VTE in leg or pelvic vein breaks off; travels through vena cava into right side of heart Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Pulmonary Embolus Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Risk Factors • • • • • • • Prolonged immobilization Central venous catheters Surgery Obesity Advancing age Conditions that increase blood clotting History of thromboembolism Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Health Promotion & Illness Prevention • • • • Smoking cessation Weight reduction Increased physical activity If traveling or sitting for long periods, get up frequently and drink plenty of fluids • Refrain from massaging Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Clinical Manifestations • Respiratory – Dyspnea, tachypnea, tachycardia, pleuritic chest pain, dry cough, hemoptysis • Cardiac – Distended neck veins, syncope, cyanosis, systemic hypotension, abnormal heart sounds, abnormal ECG, tachycardia • Low grade fever, petechiae, flu-like symptoms Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Laboratory Assessment • ABGs -> alkalosis then acidosis • PaO2 – FiO2 ratio falls • Imaging assessment – Chest x-ray – Computed tomography – Transesophageal Echocardiography Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Laboratory Assessment (cont) • D-dimer: A fragment produced during the degradation of a clot. The D here stands for domain. Dimer indicates two identical units, in this case two identical domains. D-dimer result from complete breakdown of the clot. Monoclonal antibody to the D-dimer fragment provide the basis for the main methods of detecting it. The presence of D-dimers in the blood is a reliable clue that clotting has begun. Sometimes used as a clinical marker for pulmonary embolism blood clot in the lung) or deep venous thrombosis (DVT) (blood clot in the leg) Sometimes written ddimer or D-Dimer http://www.medterms.com/script/main/art.asp?articlekey=2 4476) Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Nonsurgical Management • • • • • Oxygen therapy (nasal cannula, mask) Continuous patient monitoring Obtain adequate venous access Continuous monitoring of pulse oximetry Drug therapy – Anticoagulants – Fibrinolytics Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Interventions • Ensure appropriate antidotes are present on the nursing unit! • Assess for bleeding every 2 hr • Examine all stool, urine, drainage, vomitus for gross blood; test for occult blood • Monitor laboratory values Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Surgical Management • Embolectomy • Inferior vena cava filtration (example – Greenfield http://emedicine.medscape.com/article/419796-overview ) Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Community-Based Care • Home care management • Teaching for self-management • Health care resources Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Acute Respiratory Failure • ABG value of PaO2 <60 mm Hg, SaO2; <90%; or PaCO2 >50 mm Hg with pH <7.30 • 3 types of ARF- see next slides • Patient is always hypoxemic regardless of the underlying problem Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Ventilatory Failure • Physical problem of lungs or chest wall • Defect in respiratory control center in brain • Poor function of respiratory muscles, especially diaphragm • Extrapulmonary causes • Intrapulmonary causes Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Oxygenation Failure • Insufficient oxygenation of pulmonary blood at alveolar level • Ventilation normal, lung perfusion decreased Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Combined Ventilatory/Oxygenation Failure • Often occurs in patients with abnormal lungs (e.g., chronic bronchitis, emphysema, asthma attack) • Diseased bronchioles and alveoli cause oxygenation failure; work of breathing increases; respiratory muscles unable to function effectively and therefore causes ventilator failure Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Dyspnea Interventions • Oxygen therapy • Position of comfort • Relaxation, diversion, guided imagery • Energy-conserving measures • Drugs Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Acute Respiratory Distress Syndrome (ARDS) • Persisting hypoxia • Decreased pulmonary compliance • Dyspnea • Noncardiac-associated bilateral pulmonary edema • Dense pulmonary infiltrates seen on x-ray Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Causes of Lung Injury in ARDS • Systemic inflammatory response is common pathway • Alveolar-capillary membrane injured – Intrinsic causes—sepsis, shock – Extrinsic causes—aspiration, inhalation injury Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Diagnostic Assessment • Lower PaO2 value on ABG – refractory hypoxemia -Increasing supplemental oxygen does not cause an increase in PaO2 levels • “Whited-out” (ground glass) appearance to chest x-ray • Sputum culture Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Interventions • ET intubation and conventional mechanical ventilation • Drug – corticosteroids – when to initiate and how much to give is controversial • Fluid therapy – controversial – how much is too much Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Interventions (cont) • Nutrition therapy • Case management – Phase 1 to Phase 4 Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Endotracheal Tube A, Endotracheal tubes. B, Correct placement of an oral endotracheal tube. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Verifying Tube Placement • End-tidal carbon dioxide levels • Chest x-ray • Assess for breath sounds bilaterally, symmetrical chest movement, air emerging from ET tube Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Stabilizing the Tube Do not tape the tube too tightly to the nose or skin breakdown will occur on the naris. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Endotracheal Tubes: Nursing Care • Assess tube placement, minimal cuff leak, breath sounds, chest wall movement • Prevent movement of tube by patient • Check pilot balloon • Soft wrist restraints – last resort and all laws apply • Mechanical sedation Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Mechanical Ventilation • Purpose is to support and maintain gas exchange • Ventilation does not cure diseased lungs • Variety of ventilators used Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Nursing Management • Always assess patient first, ventilator second • Monitor patient response • Manage ventilator system • Prevent complications! Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Complications • Cardiac: – Hypotension 2⁰ positive pressure that increases chest pressure thereby inhibiting venous blood return to the heart – Fluid retention 2⁰ decreased cardiac output – Valsalva maneuver - avoid Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Complications (cont’d) • GI – stress ulcers • Nutritional – malnutrition – effects muscles – diaphragm and intercostals • Infections—ventilator-associated pneumonia (VAP) • Muscle deconditioning Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Weaning • Process of going from ventilator dependence to spontaneous breathing Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Extubation • • • • • • Hyperoxygenate patient Thoroughly suction ET and oral cavity Rapidly deflate ET cuff Remove tube at peak inspiration Instruct patient to cough Monitor patient every 5 min; assess ventilatory pattern for respiratory distress Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Chest Trauma • About 25% of traumatic deaths result from chest injuries – Pulmonary contusion – Rib fracture – Flail chest – Pneumothorax – Tension pneumothorax – Hemothorax – Tracheobronchial trauma Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Pulmonary Contusion • Potentially lethal injury • May be asymptomatic at first, later develop respiratory failure • Bloody sputum, decreased breath sounds, crackles, wheezes • Treatment—maintenance of ventilation and oxygenation Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Rib Fracture • Chest usually not splinted by tape or other materials • Main focus—decrease pain so adequate ventilation is maintained Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Flail Chest • Paradoxical chest movement—“sucking inward” of loose chest area during inspiration, “puffing out” of same area during expiration • Treatment: humidified oxygen, pain management and promotion of lung expansion Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Flail chest. Normal respiration: A, Inspiration; B, Expiration. Paradoxic motion: C, Inspiration—area of the lung underlying unstable chest wall sucks in on inspiration; D, Expiration—unstable area balloons out. Note movement of mediastinum toward opposite lung during inspiration. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Pneumothorax • Air in the pleural space around the lungs • Severity depends on the amount of the lung collapsed • Treatment: chest tube to allow the air to escape and allow the lung to re-inflate Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Tension Pneumothorax (cont’d) • Category of Pneumothorax • Air leak in the lung or chest wall that can’t exit on expiration • If it gets bad enough, there is tracheal movement away from the midline toward the unaffected side. • Treatment Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Tension Pneumothorax Left: Pneumothorax. Right: Tension pneumothorax on the left with mediastinal shift to the right. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Hemothorax Left: Hemothorax. The amount of blood that can accumulate in the thoracic cavity (leading to hypovolemia) is a much more severe condition than the amount of lung compressed by this blood loss. Right: Right hemothorax. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Tracheobronchial Trauma • Caused by blunt trauma, rapid deceleration • Tracheal lacerations • Upper airway obstruction • Cricothyroidotomy, tracheotomy Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. A 65-year-old woman is brought to the ED by her husband with new onset shortness of breath. She had an abdominal hysterectomy 5 days ago. Her husband states that she stayed in bed since she was discharged from her surgery 48 hours ago, because she feels very short of breath when she gets up. What risk factors are present for DVT? Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • Prolonged immobility; advancing age; recent surgery Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. (cont’d) During triage, the following vital signs and assessments are noted: Temp – 99.6° F BP – 80/44 mm Hg P – 126 (sinus tachycardia) R – 28 and labored O2 saturation – 84% (room air) Crackles bilaterally Petechiae across chest and in axillae Based on these findings, what do you suspect might be happening with the patient? Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • The patient may have a pulmonary embolism. She could also have pneumonia based on her recent surgery and immobility. Further assessment should be performed to ascertain the specifics of her symptoms. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. (cont’d) When the ED physician is notified of the patient’s manifestations, she is moved immediately to a treatment room. The physician writes the following orders: – O2 at 2 L per nasal cannula – Stat CBC, BMP, D-dimer, aPTT, INR – Stat CT of the chest – Start a saline lock Which order takes priority at this time? 1. Oxygen 2. Saline lock 3. Labs 4. CT Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • Based on the patient’s pulse oximetry reading, the priority order is the administration of oxygen. Next, the saline lock should be started. Once the vein is accessed, blood can also be obtained for the CBC, BMP, D-dimer, PTT, and INR. After the laboratory specimens are sent, the radiology department can be notified to perform the stat CT of the chest. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. (cont’d) While in the treatment room, the patient says she needs to use the bathroom. The nursing assistant is delegated this task. What is the best approach for the nursing assistant to take? A. A. Place the patient on a bedpan and stay with her until she is finished. B. B. Ambulate her into the hall bathroom on room air and stand outside the door until she is done. C. C. Ask the provider for an indwelling catheter because of her shortness of breath when she ambulates. D. D. Tell her to try to wait until the shortness of breath subsides. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • ANS: A • The nursing assistant should place the patient on a bedpan and stay with her. She is too short of breath to ambulate to the bathroom and she should remain on the oxygen at all times. The nursing assistant should not ask the provider about an indwelling catheter because this would only increase the possibility of a UTI. The patient should never be told to try to wait, because this could also increase the risk for UTI. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. (cont’d) Two hours later, the patient is admitted to the medical unit where she is started on a continuous IV heparin weightbased protocol. Which finding indicates that the heparin infusion is therapeutic? A. B. C. D. INR is less than 1 INR is between 2 and 3 aPTT is the same as the control aPTT is 1.5 to 2.5 times the control Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • ANS: D • When a patient is started on continuous heparin, the aPTT is drawn before therapy is started and then every 4 hours until a therapeutic range of 1.5 to 2.5 times the control is reached. Thereafter, the aPTT is checked daily. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. (cont’d) Three days later, the provider prepares to discharge the patient on warfarin (Coumadin). Which teaching points do you include about this therapy? (Select all that apply.) A. “Be sure to have follow-up INR laboratory tests done.” B. “Report any bruising or bleeding to your provider.” C. “Consume lots of foods that are rich in vitamin K, such as green leafy vegetables.” D. “Use a soft toothbrush to brush your teeth and an electric razor to shave your legs.” E. “A skin rash is expected while you are taking this drug.” Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • ANS: A, B, D • It will be important for the patient to have followup INR laboratory tests done, reporting any bruising or bleeding, and use a soft toothbrush and electric razor while on warfarin therapy. Vitamin K is the antidote for warfarin, so patients should not consume a great deal of foods that are high in this vitamin. A skin rash is a sign of an adverse drug reaction and should be reported to the provider immediately. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Question 1 Which patient is at greatest risk of developing acute respiratory distress syndrome (ARDS)? A. B. C. D. 24-year-old male admitted with blunt chest trauma and aspiration at the scene 56-year-old male with a history of alcohol abuse and chronic pancreatitis 72-year-old male post heart valve surgery receiving 1 unit of packed red blood cells 82-year-old female on antibiotics for pneumonia Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • Answer: A • Rationale: All patient scenarios create a risk for ARDS. However, the trauma patient with direct chest injury and known aspiration is at greatest risk. ARDS risk factors include direct lung injury (most commonly aspiration of gastric contents), systemic illnesses, and injuries. The most common risk factor for ARDS is sepsis. Other risk factors include bacteremia, trauma with or without pulmonary contusion, multiple fractures, burns, massive transfusion, near drowning, post-perfusion injury after cardiopulmonary bypass surgery, pancreatitis, and fat embolism. • (Source: Accessed August 2, 2011, from http://emedicine.medscape.com/article/165139overview#aw2aab6b2b3) Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Question 2 A patient is going home on warfarin (Coumadin) therapy to manage an acute pulmonary embolism. Which patient response indicates further discharge teaching is needed? A. B. C. D. “I should make a doctor’s appointment for weekly blood draws.” “I should take the medication at the same time every day.” “I should eat more green leafy vegetables like spinach.” “I should limit my alcohol consumption.” Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • Answer: C • Rationale: Patients who experience a venothromboembolism/pulmonary embolism are frequently discharged on anticoagulant therapy (e.g., warfarin [Coumadin]). The patient should be educated to understand the risks and monitoring of this drug to include weekly monitoring for therapeutic levels, consistency in dosing regimens, and foods to avoid (e.g., leafy green vegetables, green tea, alcohol, cranberry juice, etc.). • (Source: Accessed August 2, 2011, from http://circ.ahajournals.org/content/119/8/e220.full; http://www.mayoclinic.com/print/warfarin/AN00455/MET HOD=print) Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Question 3 A patient in acute respiratory failure is classified as having ventilatory failure. A potential cause of ventilatory failure is: A. B. C. D. Opioid analgesic overdose Pulmonary embolus Hypovolemic shock Pulmonary edema Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. • Answer: A • Rationale: Acute ventilatory failure is the type of problem in oxygen intake and carbon dioxide removal (ventilation) and blood delivery (perfusion) that causes a ventilation-perfusion (V/Q) mismatch in which perfusion is normal but ventilation is inadequate. It occurs when chest pressure does not change enough to permit air movement into and out of the lungs. As a result, too little oxygen reaches the alveoli and carbon dioxide is retained. Opioid analgesic overdose is a possible cause of ventilatory failure. The others listed are related to oxygenation failure. Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.