Med-Peds Case Files - American Academy of Pediatrics
advertisement

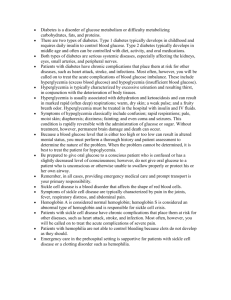
Med-Peds Case Files Last updated: December 2009 Introduction • ‘Med-Peds Case Files’ are a compilation of cases that are interesting to both internal medicine and pediatric physicians. • The purpose of the Case Files is: a) b) c) To provide a national venue for Med-Peds physicians to share interesting Med-Peds cases. To develop a public online library of Med-Peds cases for educational and promotional purposes. To provide Med-Peds physicians an opportunity to develop case preparation and presentation skills. • The Case Files will be freely available online under the AAP Med-Peds Section website starting in Fall 2009 http://www.aap.org/sections/med-peds/default.cfm Case Submissions • Resident, fellow, or attending physicians are eligible to submit a case. • Medical students may submit a case with a resident or faculty advisor. • Individuals may be personally invited for case submission. • Cases must be submitted in a structured power point format (see specifications). • Only peer-reviewed cases will be published online. • Cases may include an adult problem in a pediatric patient or progression of a childhood illness into adulthood. • Cases will be accepted on an annual basis. Slide Specifications • Introduction slide (chief complaint and/or one line intro, your name and affliated institution) • Case presentation (H&P with pertinent positives/negatives) • Labs and radiologic studies (include units and reference ranges for uncommon labs) • Management/treatment (include diagnosis/conclusion) • Learning objectives slide (take-home points for the case) • Case discussion (if possible, compare disease presentation and/or treatment in adults vs children) • References slide • Slides for question and answer to reinforce your learning objectives. Minimum of one, maximum of four questions. Do not use questions from published board review material (ie PREP, MKSAP, MedStudy) Slide Specifications • • • • • • • Maximum number of slides is 30 Use Calibri font with size no smaller than 20 Use white background with black text Use Power Point version 2003 or older Use images, pictures, tables, and/or figures when possible Use slide format with AAP logo See Case example • Focus more on the case discussion. Use bullets to highlight key points. • Note: H&P in the case example is very short. You may elaborate more if needed. Also, depending on whether you want to make the case a mystery, you may decide to put your learning objective slide later in the presentation (ie, before case discussion vs before case presentation) Questions? • For questions about case submissions, please contact Jacqueline Meeks at Jacqueline.P.Meeks@uth.tmc.edu Case example Chief Complaint: Altered mental status Jacqueline Meeks, M.D. University of Texas at Houston Health Science Center Case Presentation • 8 yo morbidly obese previously healthy AAF • Three days prior to presentation she took high dose prednisone for an asthma exacerbation. • She then developed symptoms of polyuria, polydipsia. • On presentation she was obtunded with hypovolemic shock. • Family history was significant for DM • BMI >95th percentile (85.7 kg) • Velvety hyperpigmentation over the posterior aspect on her neck was seen on exam Labs • • • • • • • • • • • Initial serum glucose 2343 mg/dL HgA1C 12.5% (CMBG 368 mg/dL) Minimal serum ketones Anion gap 24 Serum Osmolarity 393 mOsm/dL Lactic acid 6.8 Islet cell Antibody neg GAD-65 Antibody neg LDL 179, HDL 33, TG 293 Total Cholesterol 271 Microalbuminuria (high) Hospital Course • Patient was treated with IV fluids and insulin • Patient was diagnosed with type 2 diabetes Learning Objectives • Review diabetic ketoacidosis and hyperosmolar hyperglycemia • Review diagnostic criteria and screening guidelines for type 2 diabetes in children • Know that acanthosis nigricans is a marker for insulin resistance Case discussion • Acute life-threatening consequences of uncontrolled diabetes are hyperglycemia with ketoacidosis or the nonketotic hyperosmolar syndrome. Pediatric patients with nonketotic hyperosmolar hyperglycemia have a high mortality rate with risks for multiple complications. • The increasing prevalence of type 2 diabetes in children raises concerns for diabetic complication in young adults. • Diabetic education and screening can help prevent life threatening complications of undiagnosed, uncontrolled diabetes. Diabetes Diagnostic Criteria • Fasting (> 8 hrs) blood glucose >= 126 mg/dL* • Symptoms of hyperglycemia and a casual plasma glucose >= 200mg/dL. Casual meaning without regard to last meal. Classic symptoms of hyperglycemia including polyuria, polydipsia, and unexplained weight loss. • Two hour plasma glucose >= 200mg/dL during OGTT as described by WHO using a glucose load of 75 gm anhydrous glucose dissoled in water* * In the absence of unequivocal hyperglycemia, testing should be repeated on a different day. Impaired Fasting Glucose • Normal: Fasting plasma glucose (FPG) < 100 mg/dL • Impaired fasting glucose (IFG) or “prediabetes”: FPG >= 100 mg/dL and < 126 mg/dL or 2 hour values in the oral glucose tolerance test of >= 140 mg/dL and < 200mg/dL. • Two hour values in the OGTT < 140 mg/dL is normal and >= 200mg/dL is diabetes Acanthosis Nigricans Case discussion Diabetic ketoacidosis and hyperosmolar hyperglycemia represent a spectrum of uncontrolled diabetes. Diabetic Ketoacidosis Hyperosmolar Hyperglycemia Serum glucose >250 >600 Serum ketones Moderate /high Absent/Low Anion gap >12 Variable Serum osmolarity Variable >320 Mental status Mild – alert Severe - coma Stupor/coma Mortality <5% ~15% Type 2 DM Screening ADA/AAP recommends checking fasting serum glucose at age 10 or earlier with puberty, every 2 years who meet criteria: • BMI > 85th percentile for age and sex • Any two of the following risk factors: • Type 2 DM in 1st or 2nd degree relative • African, Asian/Pacific Islander, Hispanic or Native American Heritage • Signs or conditions associated with insulin resistance (i.e. acanthosis nigricans, PCOS, HTN, dyslipidemia) References: • Stoner G: Hyperosmolar Hyperglycemic State AFP 71(9):1723-29 2005 May 1 • Trachtenbarg D: Diabetic Ketoacidosis AFP 71(9):1705-14 2005 May 1 • Behrman RE, et al: Nelson textbook of Pediatrics • ADA Diabetes Care Journal • www.ndep.nih.gov • www.cdc.gov • www.obesity.org Question • You are evaluating a 14 year-old boy who has a BMI of 40kg/m2. His mother and 25 year-old sister have type 2 diabetes. A fasting blood glucose concentration for the boy is 110 mg/dL. Question • Of the following, the MOST appropriate next step to screen for diabetes is to A. measure glycosylated hemoglobin B. measure serum insulin and C-peptide level C. perform a 2 hour oral glucose tolerance test D. measure blood glucose 1 hour after a high carbohydrate breakfast E. repeat a fasting blood glucose Answer - C • The boy in the vignette is at high risk for type 2 diabetes because of elevated BMI and strong family history. His elevated fasting glucose is worrisome for impaired fasting glucose but not diagnostic for diabetes. A 2 hour glucose tolerance test should be performed to determine whether he meets criteria for diabetes. • Glycosylated hemoglobin, insulin/C-peptide levels are not diagnostic for diabetes. • A high carbohydrate diet is poorly defined • A repeat fasting glucose is likely to give an indeterminate value.