Spatial Perception - McCausland Center
advertisement

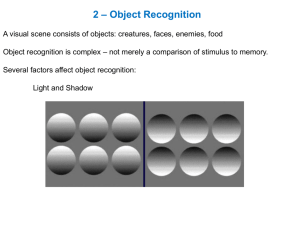
1 Perception • Chris Rorden • Lecture 8: Vision and perception • Low level visual deficits: • Visual field defects • Blindsight • Achromatopsia :: cortical colorblindness (V4) • Akinetopsia :: motion perception (MT/V5) • Agnosias :: apperceptive, associative, prosop- (FFA) • ‘How’ versus ‘what’ www.mricro.com 2 Vision Human vision: Lots of real-estate 3 Visual Pathway Each eye sees both left and right visual field. Ipsilateral information crosses over at optic chiasm. Some connections to superior colliculi. – Reflexive eye movments Others go to thalamus (lateral geniculate nuclei) and then cortex. 4 Visual Defects Field defects reveal anatomical injury A. Monocular blindness B. C. Bitemporal hemianopia D. Homonymous hemianopia E. Upper quadrantanopia F. Lower quadrantanopia G. Homonymous hemianopia 5 V1 Primary visual cortex (V1) lies in calcarine fissure. Complete damage leads to Homonymous hemianopia. Partial damage leads to scotomas 6 V1 – retinotopic mapping V1 is retinotopic: distorted spatial map of visual scene Fovea has massively over represented. 7 V1 damage and blindsight People with damage to V1 fail to report objects presented in their field defect. However, when forced to guess, they can accurately point to location of unseen visual stimulus! Can also accurately report direction of motion. Weiskrantz et al., 1974 8 Implications of Blindsight V1 is crucial for conscious awareness. What explains blindsight? Why do only 20% of V1 patients show blindsight? – Incomplete damage to V1? Islands of spared tissue (Gazzaniga, 1994). – Typically seen in people who had injury while young – neural plasticity? – Small number of indirect connections to later cortical visual centers? – Visual connections to colliculi? 9 The visual processing stream Three major streams of vision: 1. Subcortical 2. Dorsal 3. Ventral Different streams do different things… 10 Cortical visual processing Dorsal system is fast, but color blind. Helps with motor control (Where/How). Parietal MT V5 M-ganglion cells Magno LGN P-ganglion cells Parvo LGN V1 V1 V2 V3 V2 V4 Ventral system is slow, but detailed. Helps with object identification (What). IT cortex 11 Achromatopsia :: V4 Achromatopsia is usually caused by bilateral damage to V4 - lingual and fusiform gyri (occipitotemporal junction) and is characterized by an inability to identify or discriminate colour Still able to perceive form and motion 12 Akinetopsia (Motion Blindness) Zilles reported first case of akinetopsia. Pure cases are rare, as requires bilateral injury. – Case LM - akinetopsia 43 yr old. Sinus vein thrombosis V5 damaged bilaterally - V1 spared Could not see movement of objects but could see still objects. People would suddenly appear Diagnosed as agoraphobic Can see movements/reach for/catch very slow moving objects (< 10°/s) 13 V5 timecourse Beckers & Zeki (1995) examined brief V5 disruption using TMS. Motion perception disrupted most with V5 stimulation up to 30ms after visual stimulation onset V1 stimulation also partially disrupts motion perception, but later (60-70ms after VS onset). Takes 30-50ms for signals to go from V1 to V5 – Direct route to V5? – Reafference to V1? – May explain motion performance in blindsight? 14 Agnosias Three reasons why people might fail to recognize objects: – Perceptual Deficit: e.g. acuity, field cut, loss of color vision – Apperceptive agnosia: unable to perceive full shape of object despite intact low level processing. – Associative agnosia: ability to perceive shape, but unable to recognize it. 15 Apperceptive agnosia Intact low-level perception – acuity – brightness discrimination – color vision Unable to recognize objects Unable to extract global structure. 16 Associative agnosia Able to see whole form of shapes No problem copying figures However, unable to recognize the objects 17 Associative agnosia Theoretical explanations: – Disconnection between visual representation and language? – Damage to visual memory representation? – Slightly impaired perception? 18 Anatomical considerations Apperceptive agnosia: – right inferior parietal lobe (Middle Cerebral Artery) Associative agnosia: – left occipitotemporal 19 Prosopagnosia Wigan (1844), Quaglino & Borelli (1867), Hughlings Jackson (1872), Charcot & Bernard (1883), Wilbrand (1892) Inability to visually recognize faces Even a spouse’s face does not seem familiar 20 Prosopagnosia - specificity Seems specific to faces. Patients can still recognize others by: – Silhouette – Voice – Clothing Note: not like amnesia 21 Prosopagnosia Is face processing special? Or, are faces simply the most difficult objects we discriminate? Most people withprosopagnosia have difficulty recognizing differences within categories: – types of car – porcelain fixtures – breed of dog Also, often suffer achromatopsia 22 Faces are difficult Most objects are identified by unique components However, faces have the same basic components:nose, eyes,ears, hair 23 Are faces special? Farah tried to find objects as difficult as faces: – Spectacle frames – Undergrads recognized 87% of faces, 67% of eyeglass frames (faces easier) – LH recognized only 64% of faces, and 63% of eyeglass frames 24 Are faces special? 25 Are faces special? 26 Are faces special? Farah examined inversion effect Sequential matching task Undergrads: – Upright: 94% correct – Inverted: 82% correct Prosopagnosic LH – Upright: 58% – Inverted: 72% 27 Double dissociations Assal, Faure & Anderes (1984) report zooagnosic farmer MX – Lost ability to recognise cows – Still recognises faces Bruyer et al (1983) report reverse – Fails to recognise faces – Intact perception of cows 28 Double Dissociation Faces RB MX RB MX Accuracy If faces are simply difficult, we should not find patients with spared face recognition who are impaired on other tasks. Cows 29 Prosopagnosia Selective to faces in a few patients Unable to recognize faces Able to discriminate equally difficult objects: – cows – office furniture – spectacle frames Why are ‘pure’ prosopagnosics so rare? – Lesions tend to be large? – Overlap in processing in most patients? Functional imaging can resolve this question 30 Anatomical considerations Fusiform gyrus. Usually bilateral, occasionally right hemisphere only (Landis et al. 1986) Near V4 (color vision) Functional imaging gives convergent evidence (Sergent & Signoret 1992) 31 Vision in split brain patients Commissurotomy is neurosurgical treatment for intractable epilepsy where the Corpus callosum is completely divided. Allows systematic investigation of hemispheric specialization and integration 32 Split brain patients By using rapid (tachistoscopic) stimuli we can avoid eye movements. Using chimeric faces, Sperry projected different images to each hemisphere. Most able to return to work within 2 years of surgery. Typically, appear healthy Language ‘man’ Left hand woman 33 Split brain patients Picture presented in RVF (i.e. to LH) – Patient could name or reach for the object correctly with right hand. Picture presented in LVF (i.e. to RH) – Patients could not name/describe the object – Subjects could reach for the correct – object with their left hand Likewise, unable to find a object felt with one hand by using the other hand. 34 Split brain patients Left hemisphere clearly specialized in language. Right hemisphere appears better at copying designs, reading facial expressions, fitting forms in molds Similar effects can be seen in healthy people, e.g. most think A and C look more similar than A and B 35 Cortical visual processing Dorsal system is fast, but color blind. Helps with motor control (Where/How). Parietal MT V5 M-ganglion cells Magno LGN P-ganglion cells Parvo LGN V1 V1 V2 V3 V2 V4 Ventral system is slow, but detailed. Helps with object identification (What). IT cortex 36 Visual Form Agnosia DF has ventral damage – Profound agnosia :: can not even tell orientation of object – Motor control accurate :: motor system functions accurately. Posting task Patient DF Perceptual matching Posting Controls 37 Ventral vs Dorsal damage (Goodale et al. [1994] Curr Biol. 4:604-610) When shown two shapes (left), DF was poor at saying if the shapes were same or different, RV was good at this task. chance 0% DF RV Control 25% DF RV Frequency When asked to grasp an object, DF grasped near the centre (like healthy people), RV was poor at this task. 100% 0% 0 15 0 15 0 15 30 Distance from centre (mm)