Data - (S&I) Framework
 Framework")
Clinical Quality Framework
All Hands Meeting
February 11, 2016
11am-12:30pm ET
cqframework.info
Logistics
• As a reminder, please mute your phone when you are not talking to the group.
• When speaking, please say your name before making your comment.
• You can ask questions by unmuting or by using the “Chat” feature on the web meeting.
To find the “Chat” feature, look for the “Chat” bubble at the top of the meeting window.
From S&I Framework to Participants:
Could you please explain how the terminologies are used in this instance?
All Panelists
• Send your “chat” to All Panelists in order to ensure the comments are addressed publicly.
• This meeting is being recorded.
• Should you need to take another call, please leave the meeting and rejoin (i.e., please do not put the meeting line on hold).
Agenda
Topic
Welcome
DIGITizE/IOM Pilot on Genomics-Based
CDS
FHIR-Based CQF Harmonization
FHIR-Based CQF Connect-a-Thon – May
2016
CQL-based HQMF Readability Pilot
Managing Episode of Care for eCQM and
CDS – Seeking Input and Experience
Next Steps
Questions and Discussion
Presenter
Swapna Bhatia , Project Administrative Support
Sandy Aronson, DIGITizE Co-chair
Sarah Beachy , DIGITiZE Director
Bryn Rhodes, CQF Subject Matter Expert
Bryn Rhodes, CQF Subject Matter Expert
Bryn Rhodes, CQF Subject Matter Expert
Floyd Eisenberg , CQF Co-Coordinator
Ken Kawamoto , CQF Co-Coordinator
Ken Kawamoto , CQF Co-Coordinator
CQF Wiki: cqframework.info 3
Welcome
• Announcements, Meeting Schedules, Agendas, Minutes, Reference Materials,
Use Cases, Project Charter, and General Information are posted on cqframework.info
• Clinical Quality Framework (CQF) All Hands meetings are held bi-weekly on
Thursdays from 11am to 12:30pm ET
• https://siframework1.webex.com/siframework1/onstage/g.php?t=a&d=666535029
• Dial In: +1-650-479-3208
• Access code: 666 535 029
• CQF Data Model meetings are held weekly on Wednesdays from 1 to 2pm ET
• https://meetings.webex.com/collabs/#/meetings/detail?uuid=M8UL81KQZZKHCW46R28OYGI
NQM-8ENJ&rnd=47738.082690
•
Dial In: +1-770-657-9270
• Participant passcode: 217663
• CDS-on-FHIR/CQF Office Hours meetings are held weekly on Wednesdays from 11am to 12pm ET
• https://global.gotomeeting.com/meeting/join/554237525
• Dial In: +1-770-657-9270
• Participant passcode: 6870541
CQF Wiki: cqframework.info 4
Displaying and Integrating Genetic
Information Through the EHR Action
Collaborative
(DIGITizE AC)
Can We Deploy
Can We Deploy
Patients?
to Far More Patients?
How Quickly Can We Do So?
Can We Create
Inter-institutional Foundational
Health Information Technology
Power of Genetics
That will be helpful now but also stand the test of time?
Strategy
• Assemble Stakeholders
• Identify areas of agreement
• Transform into an inter-institutional project coordination group
Stackholders
• Government
• Providers
• Laboratories
• Vendors
• Patients Representatives
• Standards Organizations
Membership
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Sandy Aronson, Partners HealthCare
J.D. Nolen, Cerner
Mark Adams, Good Start Genetics
Gil Alterovitz, Harvard Medical School
Brian Anderson, athenahealth
Jane Atkinson, NIDCR
Larry Babb, Partners HealthCare
Dixie Baker, Martin, Blanck and Associates
Gillian Bell, Moffitt Cancer Center
Chris Chute, Johns Hopkins University
Chris Coffin, Invitae
Mauricio De Castro, U.S. Air Force
Carol Edgington, McKesson
Laurel Estabrooks, Soft Computer Corporation
Robert Freimuth, Mayo Clinic
Geoff Ginsburg, Duke University
Jennifer Hall, University of Minnesota
Stephanie Hallam, Good Start Genetics
Heather Halvorson, U.S. Air Force
Gillian Hooker, NextGxDx
Stan Huff, Intermountain Healthcare
Kristen Janes, Kaiser Permanente
Andrew Kasarskis, Mount Sinai School of Medicine
Anthony Kerlavage, NCI
Deborah Lange-Kuitse, McKesson
Debra Leonard, University of Vermont
Steve Lincoln, Invitae
Ira Lubin, CDC
Elaine Lyon, ARUP Laboratories
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
John Mattison, Kaiser Permanente
Larry Meyer, VA
Blackford Middleton, Vanderbilt University
Doug Moeller, McKesson
Scott Moss, Epic
James O'Leary, Genetic Alliance
Erin Payne, Northrop Grumman
Brian Pech, Kaiser Permanente
Teji Rakhra-Burris, Duke University
Priyadarshini Ravindran, Allscripts
Mary Relling, St. Jude Children's Research Hospital
Wendy Rubinstein, NCBI
Hoda Sayed-Friel, Meditech
Megan Schmidt, Sunquest Information Systems
Jud Schneider, NextGxDx
Sam Shekar, Northrop Grumman
Brian Shirts, University of Washington
Brad Strock, Epic
Jeff Struewing, NHGRI
Charles Tuchinda, First Databank
Deepak Voora, Duke University
Michael Watson, ACMG
Scott Weiss, Partners HealthCare
Jon White, ONC
Bob Wildin, NHGRI
Ken Wiley, NHGRI
Marc Williams, Geisinger
Grant Wood, Intermountain Healthcare
Identify Areas of Agreement
Framework for Increasing Support for
Genetics in the EHR Ecosystem
PGx Use Case Patterns
Germline Use Case
Patterns
Somatic Use Case
Patterns
Objective
Learn how to work together while producing near term benefit for patients
Simple use cases are good for this
Don’t Boil the Ocean
Boil some initial cups while standing on firm ground
Framework for Increasing Support for
Genetics in the EHR Ecosystem
PGx Use Case Patterns
Germline Use Case
Patterns
Somatic Use Case
Patterns
Initial
PGx Use Case
Types
Initial
PGx Use Case
Types
Specific
Example
Specific
Example
Abacavir – HLA-B57:01
• Approximately 6% of European ancestry patients are hypersensitive to Abacavir
• Hypersensitivity can produce life threatening reaction
• Genetic test can predict hypersensitivity
Martin et al, 2012 CPIC Guidelines
Thiopurine - TPMT
• Metabolic effect
• Prescribing too high a dose places patient at risk for myelosuppression
• Test is required to accurately dose
Reilling et al, 2011 CPIC Guideline
Key Pharmacogenomic
Use Cases Types
# Use Case Types
1 Incorporating Genetic Results into EHR User Interfaces
2 Adding genetic tests in order sets
3 Clinical Decision Support (CDS) identifies when a test should be ordered (pre-test alert*)
4 CDS identifes when a drug order is inconsistent with a test result (post-order alert*)
* Note pre and post order status refers to the status of the test order as opposed to the drug order
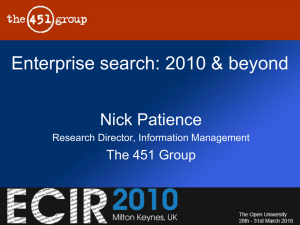
Project Coordination
Example of Cross Institutional Dependencies
• A use case calls for providers to implement a CDS rule that requires data from the EHR ecosystem
• To supply the required data EHR ecosystem vendors need to receive data from lab system vendors
• To instantiate the required data flows lab and EHR ecosystem vendors need better defined standards
• Standards organizations need feedback from lab and provider organizations to produce needed refinements
The Action Collaborative has the breadth of membership required to manage these types of issues
Interdependency
Providers
Data
Labs
Interdependency
EHR Vendors
LIS Vendors
Supporting
Vendors
Providers
Data
Interoperability and functionality
Labs
Interdependency
Cooperation /
Interfaces
EHR Vendors
LIS Vendors
Supporting
Vendors
Providers
Data
Interoperability and functionality
Labs
Interdependency
Cooperation /
Interfaces
Providers
Data
Interoperability and functionality
EHR Vendors
LIS Vendors
Supporting
Vendors
Standards and Ontologies
Standards &
Ontology
Organizations
Labs
Interdependency
Cooperation /
Interfaces
Providers
Data
Interoperability and functionality
EHR Vendors
LIS Vendors
Supporting
Vendors
Standards and Ontologies
Input
Standards &
Ontology
Organizations
Labs
Interdependency
Cooperation /
Interfaces
Providers
Data
Labs
EHR Vendors
Interoperability and functionality
Proof of what is possible/helpful
LIS Vendors
Supporting
Vendors
Standards and Ontologies
Input
Standards &
Ontology
Organizations
Gov
Agencies
Interdependency
Cooperation /
Interfaces
Funding / Reimbursement Environment that
Makes this Possible
Data
Labs Providers
EHR Vendors
Interoperability and functionality
Proof of what is possible/helpful
LIS Vendors
Supporting
Vendors
Standards and Ontologies
Input
Gov
Agencies
Standards &
Ontology
Organizations
The Good News
Cooperation /
Interfaces
EHR Vendors
LIS Vendors
Supporting
Vendors
Providers
Patients
Labs
Gov
Agencies
Standards &
Ontology
Organizations
Lucky Choice in Baseline Rules
• Not dependent on structured variant transfer
• Warn every time potentially desirable
• Existing standards work
Implementation Guide
• Rational
• LOINC Transfer Codes
• Suggested Rules
Where to Next
• Pilots!
• More Use Cases
– Internal: FH
– CSER Led: Lynch Syndrome
• Things the community feels we can help with
FHIR-Based CQF Harmonization
• First-class resources have been defined
– Still have some polishing/documentation to do
• FHIR-Infrastructure Alignment is complete
– ModuleMetadata type is committed
– FHIR-I is submitting proposals for alignment of conformance resources
• Incorporating CDS/eCQM Ballot Comments is in progress
– Reconciled spreadsheets are on Google docs
– Anyone that can/wants to help is welcome to join the CQF calls where we will be coordinating the effort and reviewing progress
FHIR-Based CQF Connect-a-Thon May 2016
• Proposal has been submitted
• Scenarios from the January Connect-a-Thon were brought forward
• Additional Scenarios:
– Knowledge Management Repository service and client
– Measure Evaluation results
– SOA Integration Scenario
• Intended to model a complete clinical quality spike
– Includes artifact distribution, ingestion, and evaluation for decision support and quality measurement
• Event Publish/Subscribe Service (EPS)
• Unified Communication Service (UCS)
CQL-Based HQMF Readability Pilot
• Objective – Supplement the CQL-Based HQMF
IG with additional material to inform knowledge artifact development with CQL
• Areas of Focus
– Display of CQL Population Criteria within the
HQMF
– Usability/Readability of the resulting HQMF
– Consistent authoring of CQL
– Accessible Documentation for CQL-Based Artifacts
32
Areas of Active Discussion
• Reordering criteria expressions
– top-down vs bottom up
• Utilizing HTML Functionality
– Linking, expand/collapse, fly-out options
• UX Review/508 Review
• Criteria Sections
• CQL Style Guide
• CQL Documentation Availability
• Common Library Usage
33
Reordering and Indenting of Criteria
• CQL expressions have been typically developed “bottom-up”
– Starting from the data elements and value sets
– Construct intermediate expressions to represent conceptual components of the criteria
– Combine these intermediates to produce the overall criteria
• This approach makes sense from an authoring perspective, but can be confusing to someone coming at the measure from the criteria sections
• Reorder the expressions “top-down”
– Starting from the top-level population criteria expressions
– Display the component expressions involved as they are encountered, and indented below the referencing expression
34
Utilization of HTML
• UX/Usability Review/508 Review
• Several options here
– Add hyper-links to the expressions to allow to be easily navigated
• Doesn’t work very well with native HTML functionality, the navigation is abrupt and often unclear what’s happening
– Add expand/collapse functionality to help organize the criteria expressions
• The solution is functional, but it doesn’t really add much because it just hides the criteria. For very large measures, this may be useful, but in general, probably not
– Add fly-outs to enable discovery without having to navigate
• This could be done in pure HTML with the “alt-text”, but it would rely on browserspecific behavior, and could potentially introduce some 508 compliance issues
• Adding java-script would enable some much more sophisticated functionality
• Specific coloring for valueset references
• Hyperlinks for valueset references to the data elements section
35
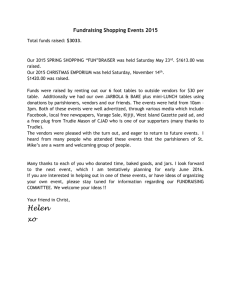
Criteria Sections
• Follow HQMF Guidance in ensuring all relevant criteria are displayed for a measure, even if the criteria is empty
Measure
Score
Initial
Population
Denominator Denominator
Exclusion
Denominator
Exception
Numerator Numerator
Exclusion
Measure
Population
Measure Population
Exclusion
Proportion
Ratio Required
Continuous
Variable
Required
Cohort
Required Required
Required
N/A
Required N/A
Optional
Optional
N/A
N/A
Optional
N/A
N/A
N/A
Required
N/A
Optional
Required
N/A
Optional
N/A
N/A
N/A
N/A N/A
Required Optional
N/A
N/A
N/A
36
CQL Style Guide
• Work with Measure Authors to define a CQL Style
Guide
• Specify conventions for
– White-space usage
– Naming
– Casing of identifiers
– Indenting style
– Expression organization (e.g. when is a block “too big”)
• Identify and establish guidance for common patterns
• Potentially develop tooling to support automatic formatting (a la GoFormat)
37
CQL Documentation Availability
• Increase accessibility of relevant CQL documentation from the measure itself
– Could use hyper-links to an online CQL Reference
– Could embed documentation for CQL operations used within the measure
• As flyouts or a “documentation” section at the end of the measure
38
Common Library Usage/Documentation
• Work with artifact developers to establish common libraries
• As with any knowledge asset reuse effort, this would require
– Governance
• How are the assets developed, tested, approved, published, and maintained?
– Visibility
• How do artifact developers find relevant assets?
– Guidance
• How do artifact developers know how to use the assets?
• Documentation accessibility from the resulting artifacts
39
Next Steps
• Develop more complex/representative measures
– Complex Logic
– Multiple Populations
– Composite Measures
– Stratification
– Risk Adjustment
• Gather feedback from different venues
40
Defining Episode of Care
• Definition: A series of temporally contiguous healthcare services related to the treatment of a given spell of illness or provided in response to a specific request by the patient or other relevant entity.
1
1 National Quality Forum (NQF). Measurement Framework: Evaluating Efficiency Across
Patient-Focused Episodes of Care. Washington, DC: NQF; 2009.
41
Defining Episode of Care 2
2 National Quality Forum (NQF). Evaluating Episode Groupers: A Report from the
National Quality Forum. Washington, DC: NQF; 2014. (p. 8)
42
Episode of Care – Claims-based 3
3 National Quality Forum (NQF). Evaluating Episode Groupers: A Report from the
National Quality Forum. Washington, DC: NQF; 2014. (p. 10)
43
Seeking Field Experience with Clinical Data
• Determining the “start” and “end” of clinical encounters within an episode – Examples:
– Within a hospital facility:
• ED —› Observation Status —› Inpatient
• Outpatient Surgery —› Observation —› Admission
• Admission —› ICU —› Step-down Unit —› MedSurg
– Cross settings of care – Examples:
• Ambulatory office —› Physical Therapy —› ED —› Ambulatory office
• Tracking care for a specific health concern over time and location
– Admission – Discharge times
– Arrival – Departure times
44
Episode of Care: Observation Use Case
• Observation care is a well-defined set of specific, clinically appropriate services, which include ongoing short term treatment, assessment, and reassessment before a decision can be made regarding whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital. Observation services are commonly ordered for patients who present to the emergency department and who then require a significant period of treatment or monitoring in order to make a decision concerning their admission or discharge.
Medicare Benefit Policy Manual. (Chapter 6, Section 20.6) https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c06.pdf
45
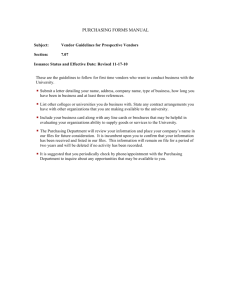
Episode of Care: Observation Use Case
• Seeking input on how EHRs handle transition from
Emergency Department to Observation Status to
Admission within a single episode of care
• Purpose – to evaluate the single episode from facility arrival time to treatment to facility departure time
Emergency
Department
Single Episode of Care – 1
Facility
Observation
Status
Hospital
Admission
46
Episode of Care: Observation Use Case
• Method to Determine the Following Times
ED
• Arrival Time
• Departure Time
Observation
• Arrival Time
• Departure Time
Hospital
Admission
• Arrival Time
• Departure Time
• Admission Time
• Discharge Time
• Admission Time
• Discharge Time
• Admission Time
• Discharge Time
47
Next Steps
• Engage in workgroups ( www.cqframework.info
)
• Pilots
– Co-Coordinator, Ken Kawamoto
• Standards Development
– Subject Matter Expert, Bryn Rhodes
• Join us for the upcoming Clinical Quality Framework All Hands meeting:
• 2/25
CQF Wiki: cqframework.info 48
Questions and Discussion
cqframework.info
Name E-Mail
Ken Kawamoto, Co-Coordinator kensaku.kawamoto@utah.edu
Floyd Eisenberg, Co-Coordinator floyd.eisenberg@esacinc.com
Swapna Bhatia, Initiative Support swapna.bhatia@esacinc.com
CQF Wiki: cqframework.info 49