LIS Validation Tool Test Flow
advertisement

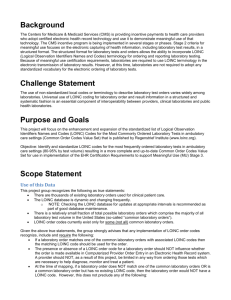
LRI Validation Suite Meeting October 11th, 2011 Agenda (Red=topics today) • Action Item List • Test data update – – – – Selection of core message set Review of lab results test category spreadsheet First set of test messages NIST data sets and management of test data • Review policy proposal for validating receiver processing of terminology • Identify/Create/Verify Value Sets – HL7 Tables, LOINC, UCUM, SNOMED CT • • • • Review ELINCS Test Plan and Test Tool (09/29/2011) Update on LIS Test Plan Template Update on EHR Test Plan Template Spreadsheet Analysis/Juror Document – – – – Overview and purpose of spreadsheet Mapping CLIA requirements to HL7 Elements Identifying Reportable Conditions to PH Lab Results IG Example Messages (IG Analysis Call) • Tooling Update • Planning Draft Test Messages • Completed/Located Draft Messages – – – – – – • Hematology Chemistry Microbiology (has been reviewed by Riki) Special Chemistry (Lipid Panel) Susceptibility Other (Surgical Pathology ) Work in Progress – Routine Urinalysis – Complete Urinalysis • Provides at least one message for each of the categories we identified • We will use these to finish test plan skeletons, to develop data management spreadsheet, create test case variations, etc. • Disclaimer: These messages are not verified to be correct and do not yet meet the technical/structural requirements specified in the IG. Draft Test Messages • Hematology – Hemoglobin 718-7 – use as example for minimally populated message • Started mapping to IG – – – – • • • • • • Potentially maximally populated message (with no repeats) Unknown patient OID version Non-OID version Chemistry Microbiology (has been reviewed by Riki) Special Chemistry (Lipid Panel) Susceptibility Other (Surgical Pathology) Work in Progress – Routine Urinalysis – Complete Urinalysis ELINCS I • Met with Walter Sujansky and team on 09/27/2011 • Generally speaking, in-line with validation suite approach • Automated LIS Validation and Inspection Testing for EHR (EHR Display and mostly CLIA) – Other data items not specified as CLIA requirements were not examined – I think we can relax our requirement that all required elements need to be inspected; some will be implied (a lot of MSH, set id, etc.—it is just part of the message processing) – Other items will need to be inspected (access to DB) – Did not test “RE” usage elements; did test for conditionals when feasible – LIS testing was context free testing • About 20 test messages covering the various scenarios (e.g., P, F, C). – Messages posted on Wiki – We can adopt these messages with modifications – Limited in scope (in terms of the breath of lab results) • Agreed that an “Expert Reviewer” is needed to access terminology equivalence – ELINCS was self testing tool (CCHIT did the certification) – We’ll follow same model (we’ll provide recommendations for “Expert Reviewers) ELINCS II • Since Labs and trading partners will have worked out mappings we can’t necessarily expect a particular mapping for our test cases (test data sheets) – This is OK; we can validate to make sure it is a valid LOINC and also provide a set of acceptable LOINCs – The tool can provide an “ERROR with exceptions”; meaning that the validation flagged it but it may be OK based on the inspection of an “Expert Reviewer” • Code is .net/C# (Desktop application) – We’ll leverage ideas, not code base • Configuration for certain data elements – Addressing, Patient IDs, local codes?, etc. – Dynamically create messages from message templates – Inline with the validation suite WG design LIS Validation Tool Test Flow Use Case Test Case Data Sheet Specific Lab Test • Provide LOINC Code • Allow for local code (from Order) Vendor LIS System Message LIS Test Tool select test case Validation Report LIS Test Harness Test Flow Testing the EHR – Model 1 Use Case 1. 2. 3. 4. LIS Test Harness Test Cases Specific Lab Test • Provide LOINC Code • Allow for local code (from Order) via configuration? Juror Document Test Data LN-1 Test Message Validation Lab Message Comm LN-1 On-site inspection Over-webex technology Printed Report (?) Screen-scraper – screen-capture (include clock) What are the requirements on the EHR with regards to LONIC? • Persist original LN code? • Display Lab Results (options) EHR ACK LN-1 Optional Techniques Tech 1 Database access Tech 2 View configuration files Tech 3 CDA/CDD Tech 4 HL7 message to public health Report *In all cases, some level of inspection test should be performed LIS Test Harness Test Flow Testing the EHR – Technical Option #2 Use Case LIS Test Harness Test Cases LN-1 Test Data Test Message Validation Report Should we expect the same LONIC code? Juror Document Lab Message Comm LN-1 EHR ACK LN-1 HL7 V2 HL7 V2 Validator Mapped LN-1 Text on display Report Comments from Vocabulary WG (C. Johns) I • LOINC codes often indicate a specific processing method for a particular lab test; the NLM has recommended use of LOINC codes that do not specify a method (ie, are “methodless”) – Read: Our test cases/messages should focus on LOINC codes that are methodless; however a test case that specifies a LOINC code (that specifies a method) is OK • The Vocabulary Standards workgroup’s understanding is that EHR conformance testing is only to determine if the system can accommodate LOINC codes, not to determine that the system correctly applies LOINC codes to the lab tests – This was not our assumption; The MU term is “incorporate”. If the system doesn’t have to apply/incorporate the standard codes, what is the purpose of requiring standard codes? • Conformance testing should allow for both a LOINC code and a “local” (proprietary) code for a lab test – Agreed. Test tool will allow for this in configuration. Lab and EHR may have agreed upon codes that they use. If both LOINC and local codes are sent then mapping is straight-forward (bound in the message). – OK for inaction with real labs and pilot testing, but what about certification where the Lab is the test tool (no mapping agreements made). Does EHR have to do mappings from just a LOINC code? Comments from Vocabulary WG (C. Johns) II • Conformance testing should allow any LOINC code to be used for any lab test – ie, if a result message sent to an EHR uses an ESR LOINC code for a Retic Count lab test, the system is still in conformance because it was able to accommodate a LOINC code at all – Not sure what this means; but if a certain type of lab result is ordered don’t you expect to see a LOINC code that represents that lab results? • The LRI Validation Tool should be designed to allow any kind of character (alpha, numeric, or alpha-numeric) for the LOINC fields of the HL7 segments (e.g., OBX-3) – Does LOINC have a certain format? If so, then this format is the only code that should be accepted (For the OBX.3 triplet that contains the LOINC code). • If the LRI Validation Tool is designed to test for a valid LOINC code in the LOINC fields of the HL7 segments, the Tool should be able to check the entire LOINC database to determine if the LOINC code used is in the database, but the Tool should not determine if the correct LOINC code was applied for a specific test – Even if given a specific order/test case data sheet? Correct Reasonable/equivalent? – We did not plan on checking the LOINC database for context-provided test cases (for context-free testing this may be appropriate) Challenge of Testing Terminology I (Receiver System) • Problem Statement: – A specific terminology is specified for use in the IG (e.g., LOINC; OBX.3.1 (code), OBX.3.2 (text), and OBX.3.3 (LN-coding system) – The LIS Test Harness sends the EHR a test message containing a LOINC code • How do we test? • How do we test the universe of possible codes? • Considerations: – Meaningful Use Requirements (See next Slide) – EHR likely translate/map code to internal code and display local text representation on display – EHR could use standardized codes internally – Inspection Testing • Automated testing is limited Meaningful Use Requirements • • LOINC is a named standard for lab test results in the §170.306.g Reportable Lab Results Stage 1 ONC certification criterion. In the §170.302 (h) Incorporate laboratory test results criterion it states: – Receive results. Electronically receive clinical laboratory test results in a structured format and display such results in human readable format. – Display test report information. Electronically display all the information for a test report specified at 42 CFR 493.1291(c)(1) through (7). – Incorporate results. Electronically attribute, associate, or link a laboratory test result to a laboratory order or patient record. • The criteria use the following verbiage when referring to LOINC: – “§170.306 (g) Reportable lab results. Electronically record, modify, retrieve, and submit reportable clinical lab results in accordance with the standard (and applicable implementation specifications) specified in §170.205(c) and, at a minimum, the version of the standard specified in §170.207(c).” – §170.207(c) states: “Standard. Logical Observation Identifiers Names and Codes (LOINC®) version 2.27, when such codes were received within an electronic transaction from a laboratory (incorporated by reference in §170.299).” – In the ONC Final Rule Preamble for 170.304.i Exchange Clinical Information and Patient Summary Record ONC stated the following: • “For the purposes of electronically exchanging a patient summary record, we expect the patient summary record to include health information that is coded, where applicable, in accordance with adopted vocabulary standards. Therefore, unless otherwise required in the context of a meaningful use objective and measure, an eligible professional (or eligible hospital) would be permitted to map or crosswalk local/proprietary codes to the adopted vocabulary standards prior to transmitting a patient summary record.” – MU Stage-2 requirement not finalized Processing of Terminology • Receiver requirements for processing terminology: – The receiver shall persist (store) the original standardized code and the original standardized code text as received in exact representation. – The receiver may perform a translation/mapping to locally defined representations. Assessment of Terminology • Proposed procedure for assessing the receiver for incorporation of terminology: (for Lab Results name not results—results need to be exact) – Where applicable to meet CLIA requirements the receiver shall display on the EHR GUI the equivalent representation of the received coded lab results. The receiver shall display at least one of the following: • Original standardized code text • Original standardized code (will the actual code ever be displayed; is it adequate or good practice to display just the code?) • Local code text – The receiver shall be capable of demonstrating the persistent of the original standardized code and the original standardized code text. Acceptable methods for attestation: • Administrative access to database • Inspector approved method – If applicable the receiver shall be capable of demonstrating the linkage of the original standardized code the locally translated/mapped code. Acceptable methods for attestation: • Administrative access to database • Browse capabilities of configuration files • Inspector approved method Equivalent Representation • The exact original code • The exact original code text • For translated/mapped local code text an equivalent representation as determined by clinical terminology expert. The following rules and guidance are given to promote consistency in assessment: – Rule: A terminology shall never be made more specific in the translation/mapping. – Rule: A terminology shall never be made more specific in the display of standardized terminology. – Guidance: A limited number of synonyms are provided to assist the clinical terminology expert. Note: a predefined definitive set is not possible—there are too many possible equivalent local representations. – Guidance: The inspector must consider the context in which the code is used as this may impact the translation/mapping. Questions • What should be the assessment if a more detailed terminology term is received that is mapped to a less specific term? • This mapping will lead to a loss of information if the original code is not persisted. • Is it valid to display a representation that has less specificity? • Is it valid to display a representation that has less specificity as long as the original data is persisted in the system? • Is it acceptable for a loss of information to occur when data is rendered as a report or forwarded on to another system (e.g., public health)? That is, we sent a specific code and then a general code is forwarded on to public health. Is it acceptable for either the general or specific LOINC code to be forwarded? LOINC-RELMA List for Hemoglobin LOINC # 11559-2 19949-7 19951-3 19953-9 19955-4 2714-4 2715-1 2716-9 2717-7 30369-3 30370-1 34969-6 Component Ex. UCUM Units Ex. Units Order/Obs Oxyhemoglobin/Hemoglobin.total % Observation 1 Oxyhemoglobin/Hemoglobin.total % Class MFr % MFr % 2 Oxyhemoglobin/Hemoglobin.total MFr % % 2 Oxyhemoglobin/Hemoglobin.total MFr % PULM 2 Oxyhemoglobin/Hemoglobin.total MFr % PULM 2 Oxyhemoglobin/Hemoglobin.total MFr % % Observation 1 Oxyhemoglobin/Hemoglobin.total MFr % % Observation 1 Oxyhemoglobin/Hemoglobin.total MFr % % Observation 1 Oxyhemoglobin/Hemoglobin.total MFr % % Observation 1 Oxyhemoglobin/Hemoglobin.total MFr % % of tot Observation 1 Oxyhemoglobin/Hemoglobin.total MFr % % of tot Observation 1 Oxyhemoglobin/Hemoglobin.total MFr % % of tot Observation 1 No Method listed in RELMA for any of these tests Property Time Aspect System Scale Long Common Name Type Pt Bld Qn CHEM Fractional oxyhemoglobin in Blood 8H^max PULM BldA Qn Fractional oxyhemoglobin in 8 hour maximum Arterial blood 8H^min PULM BldA Qn Fractional oxyhemoglobin in 8 hour minimum Arterial blood Pt Bld.preductal Qn Fractional oxyhemoglobin in Blood Preductal % Pt Bld.postductal Qn Fractional oxyhemoglobin in Blood Postductal % Pt CHEM BldA Qn Fractional oxyhemoglobin in Arterial blood Pt CHEM BldC Qn Fractional oxyhemoglobin in Capillary blood Pt CHEM BldV Qn Fractional oxyhemoglobin in Venous blood Pt CHEM Plas Qn Fractional oxyhemoglobin in Plasma Pt CHEM BldCoV Qn Fractional oxyhemoglobin in Venous cord blood Pt CHEM BldCoA Qn Fractional oxyhemoglobin in Arterial cord blood Pt CHEM BldMV Qn Fractional oxyhemoglobin in Mixed venous blood Testing Options/Policy-OLD LOINC # Component Ex. Units Class Type 11559-2Oxyhemoglobin/Hemoglobin.total MFr % 1 19949-7Oxyhemoglobin/Hemoglobin.total MFr % 2 19951-3Oxyhemoglobin/Hemoglobin.total MFr % 2 Property Time Aspect System Long Common Name Scale Ex. UCUM Units Order/Obs Pt CHEM Bld Fractional oxyhemoglobin in Blood Qn % Observation 8H^max PULM BldA Qn Fractional oxyhemoglobin in 8 hour maximum Arterial blood % 8H^min PULM BldA Qn Fractional oxyhemoglobin in 8 hour minimum Arterial blood % OBR|1|111325^EHR^2.16.840.1.113883.19.3.2.3^ISO|1132896^Lab^2.16.840.1.113883.19.3.1.6^ISO|7187^Hemoglobin^LN|||20070701152505|||||||||100^Hippocrates^Harold||||||20070701162505||CH| F|NA&Not Applicable&LB OBX|1|NM|11559-2^Hemoglobin.Total^LN||^12.4|g/dL^grams per deciliter^UCUM|12.0 to 16.0||||F|||20070701152505|||||||||Effective Labs, Inc^^^^^DRSD&2.16.840.1.113883.19.1.11&ISO^XX^^^6543|3434 Test Loop^^Ann Arbor^MI^48103^^B • Depending on what the order is, what are possible test results? Are there more than one valid test result base on local conventions, etc.? • Potential Test Case Policy: In the data sheet (test case) we can allow any of these to be selected. This assumes that nothing else in the message needs to be changed. It would be an easy way to provide the capability to tests all of these LOINC codes with minimal effort. The Long Common Name is the differentiator. • One of the determining factors likely will be whether or not the same result value can be used for all of the various versions of Oxyhemoglobin/Hemoglobin.total. Issues/Comments: • Other data elements in the HL7 message might also need to be test-specific. For example, if data for the SPM-4: Specimen Type and SPM-8: Specimen Source are included in the message, then the same message probably could not be used for all of the versions of Oxyhemoglobin/Hemoglobin.total. OBX-7: Reference Range also might be a limiting factor if venous blood and arterial blood result values have normal ranges that don’t overlap. • The LOINC code is the anchor that discretely and accurately identifies the lab test that was ordered/performed. No matter what a hospital or physician chooses to call the test, the LOINC code is the one constant that tells everyone which it test was. For our purposes, we’ll need to be sure that all of the data for the data elements in the HL7 message are appropriate for the test indicated by the LOINC code. Note on the use of LOINC • The list of tests has been organized by order panel or, for micro related tests, by target organism for easier readability. • The LOINC terms included here are considered examples only – though they may be the more common LOINC terms, each laboratory needs to be sure to map their own tests to the most appropriate LOINC, even if it is NOT on this list. • This is NOT an exclusive list of LOINC terms – ANY valid LOINC should be accepted in data exchange projects based on this specification. Other Issues I • EHR – Implementation Choices for Terminology – Use standardize coding internally – Map to local codes – Need to account for options in test procedure • How to we test for complete coverage of recommended terminology? – Create all messages for all possible (recommended) terms (for important code system, e.g., LOINC)—This is the preferred approach – Alternative approach: Create a subset and inspect/verify tables for coverage and accuracy – The LAB is not restricted to sending the recommended list of LOINC codes and the EHR should not fail when it does not recognize a LOINC code. • How can this be tested; should it be tested? – We should test that the EHR recognizes an invalid LONIC code and rejects the message. • Given that LONIC changes often what mechanisms will a system use to identify invalid codes (based on a certain format?) • We could send messages where code and text don’t match as another negative test – Selection of approach may be made on a case-by-case analysis – It may be necessary to provide coverage for all recommended LOINC codes. However, for other terminology it may not be a priority (e.g., state) or may not be feasible (SNOWMED). Other Issues II • Use of UCUM. Can/should UCUM be mapped locally and displayed as local representation? • What terminology can be mapped? • Is it in scope to test the actual results of given in the lab results (abnormal values was mentioned) CLIA Requirements 42 CFR 493.1291(c) The test report must indicate the following: 1. 2. 3. 4. 5. 6. 7. For positive patient identification, either the patient's name and identification number, or a unique patient identifier and identification number The name and address of the laboratory location where the test was performed The test report date The test performed Specimen source, when appropriate The test result and, if applicable, the units of measurement or interpretation, or both Any information regarding the condition and disposition of specimens that do not meet the laboratory's criteria for acceptability CLIA Requirements Mapped to Data Elements 42 CFR 493.1291(c) The test report must indicate the following: 1. For positive patient identification, either the patient's name and identification number, or a unique patient identifier and identification number – – 2. PID-3 : Unique patient identification number PID-5 : Patient Name The name and address of the laboratory location where the test was performed - OBX-23/24/25: Lab Identification Fields 3. The test report date - OBX-19: Date/Time Analysis 4. The test performed - OBX-3: LOINC codes for Observation Identifier 5. Specimen source, when appropriate – SPM-4: Specimen Type 6. The test result and, if applicable, the units of measurement or interpretation, or both – – – – – 7. OBX-5: Observation Value OBX-6: Units OBX-7: Reference Range OBX-8: Abnormal Flag OBX-11: Observation Result Status Any information regarding the condition and disposition of specimens that do not meet the laboratory's criteria for acceptability – – SPM-21: Specimen Reject Reason SPM-22: Specimen Quality Required CLIA Report Elements – – – – – – – – – – – – – PID-3 : Unique patient identification number PID-5 : Patient Name OBX-3: LOINC codes for Observation Identifier OBX-5: Observation Value OBX-6: Units OBX-7: Reference Range OBX-8: Abnormal Flag OBX-11: Observation Result Status OBX-19: Date/Time Analysis OBX-23/24/25: Lab Identification Fields SPM-4: Specimen Type SPM-21: Specimen Reject Reason SPM-22: Specimen Quality Are all elements required to be displayed on screen (including the components and subcomponents of these fields)? Action Item List I • Select message to handle core lab results – Identify 20 or so common lab results (In progress) – Obtain/Adapt/Create test messages to cover the core set of lab results (In progress) • Identify/List all pertinent data elements (In progress) – Create spreadsheet of all data elements with usage of R, RE, and C (rows) – Columns will identify: • Juror Document (How to assess the element) • Identify the elements required for CLIA testing • Identify static, configurable, or indifference data elements • Identify/create/verify value sets (In progress) – Create Spreadsheet; convert to NIST XML tool format – Incorporate the value sets in PHINVADS – Develop download mechanisms and transformation of values to support the NIST tooling format Action Item List II • Review LRI implementation Guide and create a list of all conformance requirements (Not Started) – Create matrix based on data elements – Link all conformance requirements to data elements when possible – Create “higher” level list of conformance requirements • Determine the policy for assessing receiver side terminology (Done: need to write policy statement) – Inspection test requirements and procedure – Automated test requirements and procedure • Complete development of LIS Test Plan Skeleton • Complete development of EHR Test Plan Skeleton Action Item List III • Identify and document the test dimensions (Not Started) – – – – – Coverage of Lab Results Scenarios (e.g., Preliminary, Final, Corrected) Reporting formats Negative testing Minimally and maximally populated • Contact CLIA and CAP inspectors to get their lab inspection process (Need contacts) • Determine a process for verifying test cases (Not Started) • Implement process for verifying test cases (Not Started) • Research ELINCS Test Tool (DONE) – Determine what we can leverage – Process flow, source code, test messages Action Item List IV • Identify all the public health reportable lab results (In progress) • Identify the data elements that differ from the public health IG and the S & I LRI IG (Not Started) • Determine a policy for validating LRI messages using EHR PH lab results messages (Not Started) • Develop spreadsheets for managing test cases/data (In progress) – Adapt tooling to process and incorporate data – Phase 1 nearly complete – Phase 2 will include the multiple dimensions (Data, Profile, Juror) • Create the HL7 standard message profiles (Starting soon) – MWB (then produce XML message template) – Need to make updates to the message profile based on changes made in version 2.7 and 2.7.1 – Write XSLT to modify XML message profile Action Item List V • Identify the CLIA conformance requirements and compare to the requirements in the implementation guide (In progress) – Mark in spreadsheet – (DONE) – Make sure conformance requirements and IG match – Write conformance requirements in IG where necessary to match CLIA requirements • Prototype tool (In progress) – – – – Requirements and design (In progress) Development (In progress) Incorporate test cases (Not Started) Testing (Not Started) Validation Methodology HL7 V2.5.1 Message Profile (LRI IG assertions) Test Case Specific Assertions (Validation Context Files) Vocabulary (Stored in PHINVADS than translated to V2.8 Table Library Format) Validation Engine and Juror Document Generator Tooling Update • LRI Implementation Guide is in ballot process – Open for comments until October 17th, 2011 • We will begin developing the HL7 standard conformance profile – MWB – Need to make updates to the conformance profile based on changes made in version 2.7 and 2.7.1 • Data Management of test cases/data will be with spreadsheet – Spreadsheet is processed to build messages and to create validation context files – Validation context files encapsulates test case related assessment – Leverage/adapt existing NIST Test messages to S&I Framework LRI IG • Early version of prototype tool developed – Limited functionality – Handles message validation based on message profiles and validation context files – Message Editing