Beyond Resistance - Missouri Rehabilitation
advertisement

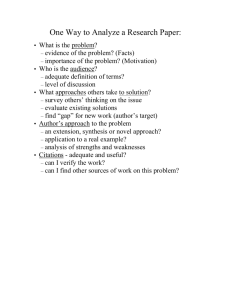
Missouri Rehabilitation Association Presents Beyond Resistance Generating Strengths, Hope, & Possibilities with Challenging People Bob Bertolino, Ph.D. Associate Professor, Maryville University-St. Louis Sr. Clinical Advisor, Youth In Need, Inc. Sr. Associate, International Center for Clinical Excellence Tidbits • • • • For copyright reasons and confidentiality some of PowerPoint slides may be absent from your handouts. To download a PDF of this presentation, please go to: www.bobbertolino.com. Please share the ideas from this presentation. You have permission to reproduce the handouts. I only ask that you maintain the integrity of the content. Contact: bertolinob@cs.com; 314.852.7274 bobbertolino.com Overview 1. Understanding Characteristics of Unresponsive Clients 2. Three Challenges with Unresponsive Clients: The Data 3. Personal Philosophy in the Service of Change 4. Evidence-Based Practice (EBP) 5. A Strengths-Based Approach: Principles and Strategies Characteristics of Unresponsive Clients Characteristics of Unresponsive Clients • What kind of clients are most challenging for you? • What specifically do these clients do that is frustrating or discouraging or difficult or __________ to mitigate? • What effect(s) do/does these behaviors have on you? • How about on your ability to help such clients? • How have you successfully mitigated past challenges with clients? Three Challenges with Unresponsive Clients: The Data Challenge #1 Psychotherapy works but primarily with a subset of clients. Despite a substantial increase in diagnostic categories and a proliferation of treatment approaches and specialized techniques, the effect size of psychotherapy has not improved since the first meta-analytic studies in 1977 (Bertolino, Bargmann, & Miller, 2012). Further, 30% to 50% of clients do not benefit from therapy (Lambert, 2010) with deterioration rates among adult clients between 5%-10% (Hansen, Lambert, & Forman, 2002; Lambert & Ogles, 2004) Bertolino, B., Bargmann, S., & Miller, S. D. (2013). Manual 1: What works in therapy: A primer. The ICCE manuals of feedback informed treatment. Chicago, IL: International Center for .Clinical Excellence. Hansen, N., Lambert, M. J., & Forman, E. M. (2002). The psychotherapy dose-response effect and its implication for treatment delivery services. Clinical Psychology: Science and Practice, 9(3), 329–343. Lambert, M. J. (2010). Prevention of treatment failure: The use of measuring, monitoring, and feedback in clinical practice. Washington, DC: American Psychological Association. Wampold, B. E. (2001). The great psychotherapy debate: Models, methods, and findings. New Jersey: Lawrence Erlbaum. Challenge #2 Clients who are not improving and/or deteriorating dropout of services at a higher rate. Dropout: the unilateral decision by clients to end therapy— averages are between 20% to 47% (Swift et al., 2012; Wierzbicki & Pekarik, 1993). In addition, it is estimated that the clients who do not benefit or deteriorate while in psychotherapy are responsible for 60-70% of the total expenditures in the health care system (Miller, 2010). Miller, S. D. (2010). Psychometrics of the ORS and SRS. Results from RCT’s and Meta-analyses of Routine Outcome Monitoring & Feedback. The Available Evidence. Chicago, IL. http://www.slideshare.net/scottdmiller/measures-and-feedback-january2011. Swift, J. K., Greenberg, R. P., Whipple, J. L., & Kominiak, N. (2012). Practice recommendations for reducing premature termination in therapy. Professional Psychology: Research and Practice, 43(4), 379-387. Wierzbicki, M., & Pekarik, G. (2002). A meta-analysis of psychotherapy dropout. Professional Psychology: Research and Practice, 24(2), 190-195. Challenge #3 There is substantial variation in outcomes between providers with similar training and experience. • Some therapists consistently have better outcomes, regardless of the diagnoses, age, developmental stage, medication status, or severity of their clients. (Wampold & Brown, 2005) • Clients of the most effective therapists improve at a rate at least 50% higher and drop out at a rate at least 50% lower than those of less effective therapists. (Wampold & Brown, 2005) • 97% of the difference in outcome between therapists is attributable to differences in their ability to form alliances with clients. (Anderson et al., 2009; Baldwin, Wampold, & Imel, 2007) Anderson, T. Ogles, B. M., Patterson, C. L., Lambert, M. J., & Vermeersch, D. A. (2009). Therapist effects: Facilitative interpersonal skills as a predictor of therapist effects. Journal of Clinical Psychology, 65(7), 755-768. Baldwin, S. A., Wampold, B. E., & Imel, Z. E. (2007). Untangling the alliance-outcome correlation: Exploring the relative importance of therapist and patient variability in the alliance. Journal of Consulting and Clinical Psychology, 75(6), 842–852. Wampold, B. E., & Brown, G. S. (2005). Estimating variability in outcomes attributable to therapists: A naturalistic study of outcomes in managed care. Journal of Consulting and Clinical Psychology, 73(5), 914–923. Personal Philosophy in the Service of Change PRACTICES “What we do” ↑ THEORY/MODELS “How we think” ↑ PERSONAL PHILOSOPHIES “Who we are” What is My Philosophy? 1. What are my core beliefs, ideas, or assumptions about the clients with whom I work? 2. How did I arrive at those beliefs? 3. What has most significantly influenced my beliefs, ideas, and assumptions as they relate to my clients? 4. How have my beliefs, ideas, and assumptions affected my work with clients? With colleagues/peers? With larger communities? What is My Philosophy (cont.)? 4. 5. 6. 7. How do I believe that change occurs? Do I believe that some degree of change is possible with every client? (If you answered “yes” then end here.)(If you answered “no,” proceed to the next question.) How do I work with clients whom I believe cannot (or do not want to or are resistant to) change? What do I do? If I do not believe that every client (and/or family) can experience some degree of change, what keeps me in doing this kind of work? The Costs of Negativity • A recent study shows that extensive discussions of problems and encouragement of ‘‘problem talk,’’ rehashing the details of problems, speculating about problems, and dwelling on negative affect in particular, leads to a significant increase in the stress hormone cortisol, which predicts increased depression and anxiety over time. • People who are in a more positive mood are better liked by others and more open to new ideas and experiences. Byrd-Craven, J., Geary, D. C., Rose, A. J., & Ponzi, D. (2008). Co-ruminating increase stress hormone levels in women. Hormones and Behavior, 53, 489–492. Fredrickson, B. (1998). What good are positive emotions? Review of General Psychology, 2, 300-319. Bertolino, B. (2015). The residential youth care worker in action: A collaborative, strengths-based approach. New York: Routledge. Evidence-Based Practice (EBP) Evidence-Based Practice (EBP) “The integration of the best available research with clinical expertise in the context of patient characteristics, culture, and preferences.” (p. 273) APA Presidential Task Force on Evidence-Based Practice. (2006). Evidence-based practice in psychology. American Psychologist, 61(4), 271–285. Clinical Expertise The APA Task Force on EBP “Clinical expertise… entails the monitoring of patient progress (and of changes in the patient’s circumstances—e.g., job loss, major illness) that may suggest the need to adjust treatment… If progress is not proceeding adequately, the psychologist alters or addresses problematic aspects of the treatment (e.g., problems in the therapeutic relationship or in the implementation of the goals of the treatment) as appropriate” (2006, pp. 280, 276-277). APA Presidential Task Force on Evidence-Based Practice. (2006). Evidence-based practice in psychology. American Psychologist, 61(4), 271–285. Lambert, M. J., Bergin, A. E., & Garfield, S. L. (2004). Introduction and overview. In M. J. Lambert (Ed.), Bergin & Garfield’s handbook of psychotherapy & behavior change (5th ed.)(pp. 3-15). New York: Wiley. Warren, J. S., Nelson, P. L., Mondragon, S. A., Baldwin, S. A., & Burlingame, G. A. (2010). Youth psychotherapy change trajectories and outcomes in usual care: Community mental health versus managed care settings. Journal of Consulting and Clinical Psychology, 78(2), 144-155. Patient (Client) Characteristics, Culture, and Preferences • • • • Client characteristics (i.e., age, gender, gender identity, ethnicity, race, social class, disability status, sexual orientation, developmental status, life stage, etc.). Strengths, resources, beliefs, and factors that can influence change. Understanding of the local knowledge and culture. Personal preferences, values, and preferences related to treatment (e.g., goals, beliefs, worldviews, treatment expectations). A Strengths-Based Approach: Principles and Strategies The Pathology Bias • Freud thought the best we could hope for in life was “ordinary misery.” • Behavioral health has historically focused on pathology. • Until recently, psychological publications and studies dealing with negative states outnumber those examining positive states by a ratio of 21 to 1. • A bias in behavioral health has been to get people back to zero; a result of which is the “empty person.” • We can help individuals to better leverage strengths and resources, a result of which is a reduction in negative symptoms and an increase in well-being. From Pathology to Strengths “What we have learned over 50 years is that the disease model does not move us closer to the prevention of these serious problems. Indeed the major strides in prevention have largely come from a perspective focused on systematically building competency, not correcting weakness. Prevention researchers have discovered that there are human strengths that act as buffers against mental illness: courage, future-mindedness, optimism, interpersonal skill, faith, work ethic, hope, honesty, perseverance, the capacity for flow and insight, to name several… We need now to call for massive research on human strength and virtue. We need to ask practitioners to recognize that much of the best work they already do in the consulting room is to amplify strengths rather than repair the weaknesses of their clients.” (p. 6-7) Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction. American Psychologist, 55(1), 5–14. Strengths-Based Defined A strengths-based perspective emphasizes the abilities and resources people have within themselves and their support systems to more effectively cope with life challenges. When combined with new experiences, understandings and skills, those abilities and resources contribute to improved well-being, which is comprised of three areas of functioning: individual, interpersonal relationships, and social role. Strengths-based practitioners value relationships convey this through respectful, culturally-sensitive, collaborative, practices that support, encourage and empower. Routine and ongoing real-time feedback is used to maintain a responsive, consumer-driven climate to ensure the greatest benefit of services. Bertolino, B. (2014). Thriving on the front lines: Strengths-based youth care work. New York: Routledge. 1 Expectancy and Hope are Catalysts of Change Key Competency Demonstrate faith in the restorative effects of services • Evidence shows that client pretreatment expectations affect engagement, retention, and outcome. • Have faith in clients and the restorative effects of services. • Believe and demonstrate faith in the procedures/practices. • Show interest in the results of the procedure or orientation. • Ensure that the procedure or orientation is credible from the client’s frame of reference and is connected with or elicits previous successes. 2 Clients are the Most Significant Contributors to Service Success Key Competency Maximize client contributions to change • The client and factors in the client’s life account for more variance (8087%) in the outcome than any other factor. • Focus on client ratings of distress and change. • Recognize clients as competent and capable of change. • Identify and utilize client contributions including internal strengths (i.e., abilities, coping skills, resiliencies) and external resources (i.e., relationships, social support systems). The Variance in Treatment Outcome • Client/Extratherapeutic Factors = 80-87% • Treatment Effects = 13-20% • Therapist Effects = 4-9% • The Alliance = 5-8% • Expectancy, Placebo, and Allegiance = 4% • Model/Technique = 1% Bertolino, B., Bargmann, S., & Miller, S. D. (2013). Manual 1: What works in therapy: A primer. The ICCE manuals of feedback informed treatment. Chicago, IL: International Center for .Clinical Excellence. Wampold, B. E., & Brown, G. S. (2005). Estimating variability in outcomes attributable to therapists: A naturalistic study of outcomes in managed care. Journal of Consulting and Clinical Psychology, 73(5), 914-923. Client Contributions • Use assessments as opportunities to explore both risks and strengths. • Identify and assist with developing supportive social systems, resources, and networks. • Explore client stories by using questions that elicit past solutions and successes: • • • • • • • Utilization Exceptions Difference Influence (Problem or Person over) Coping Splitting Linking 2 Family 3 Friends/ Social Relationships 8 Other 1 Client 7 Work/ Employment 6 School/ Education 4 Community 5 Outside Helpers 3 The Therapeutic Relationship Makes Substantial and Consistent Contributions to Outcome Key Competency Engage clients through the working alliance • The quality of the client’s participation (engagement) in services the most important process determinant in outcome. • Clients who are more engaged and involved in services are likely to receive greater benefit. • The client’s rating of the alliance is more highly correlated with outcome than provider ratings. • Work with clients to establish goals and methods to achieve those goals. What is the Therapeutic Alliance? The therapeutic alliance refers to the quality and strength of the collaborative relationship between the client and therapist and is comprised of four empirically established components: 1) agreement on the goals, meaning or purpose of the treatment; Consumer Preferences Goals, Meaning or Purpose Means or Methods 2) agreement on the means and methods used; 3) the client’s view of the relationship (including the therapist being perceived as warm, empathic, and genuine); and, 4) accommodating the client’s preferences. Client’s View of the Therapeutic Relationship Possibility Language Dissolving Impossibility Talk 1. Reflect client statements in the past tense. From: “It’s always that way.” To: “It’s been that way.” 2. Move from global (“everybody,” nobody,” “always,” “never”) to partial (“recently,” “somewhat more,” “a lot”). From: “I’m always in trouble.” To: “You’ve been in trouble a lot.” 3. Move from truth/reality to perception (“It seems to you,” “You’ve gotten the idea”). From: “Things will never get better.” To: “It really seems to you that it will never get better.” Possibility Language Future Talk: Acknowledgment and a Vision for the Future 1. Assume the possibility of future change and/or solutions by using words such as “yet” and “so far.” From: “It’s always going to be this way.” To: “So far you haven’t found any evidence that things will be different than the way they are now.” 2. Recast the problem statement into a statement about a preferred future or goal. From: “I’ll never be able to have the life I really want.” To: “So you’d like to be able to move toward the life you really want.” 3. Presuppose that changes and progress toward goals will occur by using words such as “when” and “will.” From: “No one wants to be around me.” To: “So when you begin to notice that there are people who enjoy your company and want to be around you what will be different for you?” Possibility Language Giving Permission • Give permission “to,” “not to have to,” and both From: “I shouldn’t be angry.” To: “It’s okay to be angry.” From: “People keep saying that it really should make me angry.” To: “It’s okay to not be angry about it.” From: “Sometimes I’m angry and sometimes I’m not. I must be crazy!” To: “It’s okay to be angry and you don’t have to be angry and you’re not crazy.” Say it in Another Way • “He doesn’t want to change.” • “She is manipulative.” • “He’s oppositional.” • “She’s resistant.” • “He’s got an anger management issues.” • “She’s too dependent.” • “He has poor judgment.” • “She’s out of control.” Using Action-Talk • Non-Action Talk • Cab driver talk • Opinions, evaluations, assessments, judgments • Politician talk • Vague, general, not specific as to person, place, time, thing, or action • “Someday” talk • Vague as to time or frequency Using Action-Talk (cont.) • Action-Talk/Videotalk • Move from vague, non-sensory-based descriptions to clear, observable, behaviors • Using Action-Talk to Clarify Meanings • Action complaints – specifics about what one doesn’t like or one wants to have change • Action requests – specifics about what one would like to have happen • Action appreciation – specifics about what has liked about something and would like more of • Specific to person, place, time, thing, action, or result • Who is to do what by when? • Who did what, when? 3-Point Strategy 1. Problem Description: What needs to change? • Scaling questions 2. Vision of the Future: How will we know that change has been achieved? • Miracle question, crystal ball, time machine, etc. • General future-oriented questions • Scaling questions (revisited) 3. Movement: How will we know that progress is being made? • Scaling questions (revisited) Session Rating Scale (SRS) • • • • • • • • • A 40 point measure with 4 subscales Two versions that can be scored: SRS & CSRS Complete near the end of session (last 5-10 minutes) Overall scores below 36 or any subscale below 8 should be discussed with clients Lower scores at the beginning of services can mean very different things Lower scores as services progress are 4x likely to contribute to dropout Takes less than 1 minute to administer Paper/pencil and electronic scoring systems Can plot personal data on Excel spreadsheet 4 Culture Influences and Shapes All Aspects of Clients’ Lives Key Competency Convey respect for clients and their cultures • Provide services with respect to client culture and preferences. • Maintain self-awareness of one’s heritage, background, and experiences and their influence on attitude, values, and biases. • Emphasize a multi-level understanding, encompassing the client, family, community, helping systems, etc. • Recognize limits of multicultural competency and expertise; consult others who share cultural similarities and expertise with clients being served. • Acknowledge clients as teachers and experts on their own lives. 3 • • • • • Culture Influences and Shapes All Aspects of Clients’ Lives (cont.) Create culturally meaningful experiences and activities. Use person-first language. Individualize services (avoid “one-size-fits-all” approaches). Create plans of action that are culturally sensitive. Exercise care in matching methods (i.e., techniques, interventions) with clients. • Use culturally sensitive methods of research and evaluation. • Conduct ongoing cultural self-assessments. 5 Effective Services Promote Growth, Development, and Well-Being Key Competency Utilize strategies that empower clients and improve their lives • Early response to services is strong indicator of eventual outcome. • The longer clients go without experiencing positive change the greater the likelihood they will have a negative or null outcome and/or drop out. • View problems as challenges instead of fixed pathology. • Maintain a future focus. • Use language as a vehicle for change. • Explore exceptions—how change is already happening. • Focus on small changes. • Focus on maximizing the impact of each interaction. • Monitor change from the outset through feedback. Strategies to Neutralize Resistance and Facilitate Change • Relationship to problems: Learn how clients situate themselves in relation to concerns and problems. Listen for “I,” “Me,” “Myself,” or “We” statements as opposed “You,” “He,” “She,” “Him,” “Her,” “They,” “Them” statements (Note: Be aware of cultural differences in language) • Explore coping style • Explore preparation for change • Search for exceptions Strategies to Neutralize Resistance and Facilitate Change (cont.) • Externalize the problem • Identify and alter repetitive patterns (depattern or repattern) • Life Witnesses as Supports • Find a vision for the future • Focus on language Well-Being Contributors Sales Life Circumstances 10% Set Point/Temperment 50% Intentional Activities 40% Lyubomirsky, S. (2007). The how of Intentional happiness: A scientific approach to getting the life you Life Circumstances Activities Set Point/Temperment want. New York: Penguin. Intentional Activities “Circumstances happen to people, and activities are ways that people act on their circumstance.” (Lyubomirsky et al., 2005, p. 118) • Intentional activities involve engaging in new actions, activities, and behaviors which form new habits, routines, and patterns. • These new routines—which are forms of “mental flossing— increase well-being. • The result is improved well-being, which is correlated with higher life satisfaction, better learning and retention, more creativity, and greater resiliency. Lyubomirsky, S., Sheldon, K. M., Schkade, D. (2005). Pursuing happiness: The architecture of sustainable change. Review of General Psychology, 9, 111-131. Considerations for Activities 1. Focus on fundamental skills such as listening, attending, and eliciting client feedback and respond to that feedback immediately as a means of strengthening the therapeutic relationship. 2. Collaborate with clients on determining which exercises provide the best fit. 3. Consider cultural and contextual factors with positive interventions. 4. Encourage clients to try agreed-upon exercises in a routine and ongoing manner, continue those exercises that have proven beneficial, and experiment with new ones as needed. 5. Package exercises to increase the likelihood of benefit. Five Pillars of Well-Being (PERMA) (Intentional Activities) 1. Positive Emotion: Happiness (and lastingly happier); Joy; Life Satisfaction 2. Engagement: “Being at one” with some absorbing activity (Flow) 3. Relationships: Building positive relationships and social connections 4. Meaning: Using what is best inside you to belong to and serve something bigger than you are (the “larger” world and society) 5. Accomplishments: Achievement, Competence, Mastery, Development of New Skills over life span Seligman, M. E. P. (2011). Flourish: A visionary new understanding of happiness and well-being. New York: The Free Press. Past, Present, and Future 1. Think of an event, situation, or experience from the past that you have good memories about. 2. Take a deep breath or two and immerse yourself as much as possible on the event. 3. Focus on your sensations. What you can see, hear, taste, smell, and/or feel in your body. Also notice your emotions. 4. Stay with and savor those pleasant sensations and emotions and develop them as much as you can. 5. Try to remain in the experience for 3-5 minutes. 6. Repeat the exercise by focusing on the present, and more recent or current experiences. Then do the same with future and “hoped-for” experiences. What Went Well? 1. For one week, identify and write down three good things that went well each day; 2. Write down what influenced those things; 3. At the end of the week reflect on the collection of good things and if comfortable, share your experience with another person. VIA Signature Strengths • • • • • • www.authentichappiness.org VIA Signature Strengths (cont.) 1. Wisdom and Knowledge: Cognitive strengths that entail the acquisition and use of knowledge 2. Courage: Emotional strengths that involve the exercise of will to accomplish goals in the face of opposition, external or internal 3. Humanity: Interpersonal strengths that involve “tending and befriending” others 4. Justice: Civic strengths that underlie healthy community life 5. Temperance: Strengths that protect against excess 6. Transcendence: Strengths that forge connections to the larger universe and thereby provide meaning Signature Strengths Exercise • Take one signature strength and for the following week use that strength in a new way, every day. Peterson, C. (2006). A primer in positive psychology. New York: Oxford University Press. Seligman, M. E. P., Steen, T. A., Park, N., & Peterson, C. (2005). Positive psychology progress: Empirical validation of Interventions. American Psychologist, 60(5), 410-421. Character Strengths and Posttraumatic Growth • Character Strengths found to predict Posttraumatic Growth: • • • • • • Bravery Gratitude Hope Kindness Religiousness Character Strengths found to be important mediators of success in situations characterized by significant cognitive, emotional, and physical challenges: • • • • • • Courage Honesty Leadership Optimism Self-regulation Teamwork Mathews, M. D. (2008). Positive psychology: Adaptation, leadership, and performance in exceptional circumstances. In P. A. Hancock & J. L. Szalma (Eds.), Performance under stress (pp. 163-180). Aldershot, England: Ashgate. Character Strengths and Common Concerns Presenting Problem Potential Character Strength Utilized Effective prevention of depression relapse Perspective, Curiosity, Judgment, Spirituality Residual depressive symptoms Curiosity, Perseverance Anxiety Self-Regulation, Bravery, Fairness, Curiosity Body-image issues Gratitude, Kindness Drug Use Self-Regulation, Bravery Trauma Perseverance, Bravery, Hope Improved attention and working memory Self-Regulation, Love of Learning Reduced anxiety; adaptive learning dealing with threat Self-Regulation, Curiosity, Perspective Improved romantic relationships Love, Kindness, Social Intelligence Decreased negative self-focused attention Zest, Humor Decreased negative affect Zest, Hope Rashid, T. (2009). Positive interventions in clinical practice. Journal of Clinical Psychology: In Session, 65(5), 461-466. Finding Life Purpose or Direction Four signals or life energies: 1. 2. 3. 4. Blissed Blessed Pissed Dissed Adapted from the work of Bill O’Hanlon 61 Blissed Steve Jobs “You’ve got to find what you love. And that is true for your work as it is for your lovers. Your work is going to fill a large part of your life, and the only way to be satisfied is to do what you believe is great work. And the only way to do great work is to love what you do. If you haven’t found it yet, keep looking. Don’t settle. As with all matters of the heart, you’ll know it when you find it.” Your time is limited, so don’t waste it living someone’s life. Don’t be trapped by dogma–which is living with the results of other people’s thinking. Don’t let the noise of others’ opinions drown out your own inner voice. And most important, have the courage to follow your heart and intuition. They somehow already know what you truly want to become. Everything else is secondary.” Blessed • Identify people who believed in you, encouraged you or told you you were good at something or could do something. • Consider talents, developed or natural, that you have. • Reflect on incidents of good luck (being in the right place at the right time-and taking advantage of that luck). Pissed (Righteous Indignation) The Key: Transform the “negative” energy of anger and hurts into positive energy • What would you talk about if given an hour of prime time television to influence the nation or the world? • What pisses you off that you would like to correct in the world or other people? • What can’t you sit still for? Dissed (Wounded) The Key: Transform the “negative” energy of anger and hurts into positive energy • • Ann Rice’s daughter who died of leukemia at 5. Rice wrote a novel that featured a 5-year-old who could never die. (Interview with a Vampire) U2 singer Bono’s mother died when he was 14. He has written a series of songs to help transform his hurt. In reference to the most recent one, “Iris,” Bono has said that although the song came from wound it represents his mom’s positive energy. The Outcome Rating Scale (ORS) • A 40 point measure with 4 subscales • Two versions that can be scored: ORS & CORS • Higher score indicate lower levels of distress; lower scores indicate higher levels of distress • Clinical Cutoffs: 25 (> Age 19); 28 (Ages 13-19); 32 (≤ Age 12) • Reliable Change Index (RCI): 5 • Complete at the beginning of session • Takes less than 1 minute to administer • Paper/pencil and electronic scoring systems • Can plot personal data on Excel spreadsheet ORS – Individual + + + + + + + - Self-esteem Self-perception Sense of Self Internal Strengths Healthy activities and behaviors Coping Skills Safety Anxiety Depression Substance Abuse Somatic problems (i.e., sleep, headaches, etc.) ORS – Interpersonal + + + + + + + - Close Relationships Romantic Relationships Family Close Friends Stable Living Environment Conflict Resolution Safety Violence Mystification Disconnection ORS – Social Role + + + + + + + - Other Friends and Supports Community Connections (to individuals, groups, and the community at-large) Education (School, GED, Job Skills Programs) Employment Volunteering Feeling Valued and Empowered as a Member of a Community (there can be more than one) Safety Feeling Isolated (disconnection) Lack of Acceptance Lack of Opportunity