Kaplan-Meier Estimates of Cumulative Hazards for Hip Fracture
advertisement

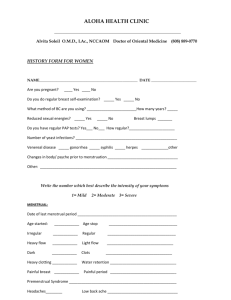
POSTMENOPAUSAL WOMEN’S HEALTH Barcey T. Levy, M.D., Ph.D. August 23, 2002 1 Objectives • Understand major health problems facing postmenopausal women • Understand the recent results of the Women’s Health Initiative and how they differ from the observational studies • Learn about therapies other than estrogen for postmenopausal women • Through the panel discussion, begin to appreciate women’s concerns regarding menopause and what they expect from their physician 2 Menopause • Cessation of menstrual periods due to declining estrogen and progesterone production by the ovaries • Refers to the final menstrual period – must be free of periods for one year to be called menopause 3 Stages of Menopause • Perimenopause – may have erratic cycles, hot flashes, and vaginal dryness; lasts from about 2 years prior to LMP to 2 years after the official “last” LMP. Average age 51 years • Menopause – refers to final last menstrual period • Postmenopausal – from “final” LMP on; women spend about 1/3 of their lives in postmenopausal period 4 Symptoms of Menopause • • • • Irregular menses Hot flashes Vaginal dryness Urinary incontinence 5 Irregular Menses • In some women, periods become lighter and less frequent • In others, bleeding may be heavier, with 2 or 3 periods a few weeks apart, and then several months before another period 6 Hot Flashes • Definition: sudden rush of heat to upper body, followed by sweating and chills • Cause: vasomotor instability triggered by hormonal changes • Affect 50 to 85% women at some point; 15% find them troubling • Treatment: estrogen quickly stops hot flashes • Home remedies: dress in light layers; small fan to cool the face; light bedclothes and cotton blanket; avoid alcohol and caffeine 7 Estrogen • Estrogen works best for hot flashes • All types and routes of administration equally effective • Markedly improves quality of life for younger postmenopausal women 8 Vaginal Dryness • Definition: reduced vaginal secretions and thinning of the mucous membranes lining the vagina dryness and itching and painful intercourse • Cause: declining estrogen levels • Treatment: estrogen; nonprescription lubricant such as Replens • Home remedies: regular sexual activity or nonperfumed oils such as vegetable oils or Vitamin E oil 9 Urinary Incontinence • Definition: involuntary loss of urine; main types stress or urge incontinence • Cause: declining estrogen levels thinning of urethra and bladder tissue; anatomical changes in pelvic organs such as cystocele, rectocele or uterine prolapse • Treatment: varies by cause; estrogen therapy may improve bladder control in some postmenopausal women • Home remedies: exercises to tone and strengthen muscles around the bladder (Kegel); avoid caffeine, alcohol and high dose Vitamin C; bladder retraining 10 Public Health Issues • • • • Heart disease Osteoporosis Cancer Dementia 11 Heart Disease in Women 32,100,000 women have heart disease 512,902 deaths/year among women Accounts for 1/2.4 deaths among women 12 Other Public Health Issues in Women Osteoporosis 28,000,000 low bone mass or osteoporosis Cancer (2001) new cases Lung 78,800 Colon 68,100 Breast 192,200 Dementia deaths 67,300 29,000 42,200 4,000,000 total (men and women) 13 Estrogen and Heart Disease • A healthy 60 year old female has about a 30% lifetime risk of dying of heart disease • Observational studies show a 35 to 50% lower risk of CAD in estrogen users • However, results of recent clinical trials conflict with these findings 14 Nurses’ Health Study • Largest prospective cohort study in which HRT use and CAD examined (observational) • 70,543 women without prior CAD observed for up to 20 years • Outcome: CAD RR Current hormone use 0.60 Past hormone use 0.82 • Results were similar for both E users and E+P users 15 Nurses’ Health Study Risk of Death Among All Postmenopausal Hormone Users (Never = Referent) Grodstein, NEJM 1997 Hormone Use Cause of Death All Causes # of Cases adj RR (95% CI) CAD # of Cases adj RR (95% CI) All Cancer # of Cases adj RR Breast Cancer # of Cases adj RR Current Past 574 0.63 (0.56-0.70) 1012 1.03 (0.94-1.12) 43 0.47 (0.32-0.69) 129 0.99 (0.75-1.30) 353 0.71 (0.62-0.81) 529 1.04 (0.92-1.17) 85 0.76 (0.56-1.02) 94 0.83 (0.63-1.09) 16 Meta-analyses of Observational Studies CAD -- 10 Prevention All Studies Prospective Studies RR Current HRT vs. Non-users 0.53 0.60 17 HERS RCT of HRT for Secondary Prevention of CAD (Hulley, JAMA 1998) • 2763 women with CAD < 80 years, postmenopausal (mean age 66.7 years) • 0.625 mg conjugated estrogen + 2.5 mg MPA qd (n= 1380) or placebo (n= 1383) followed for 4.1 years • Outcome: non-fatal MI or CHD death 18 HERS Results • No difference in MI or CHD death between groups (RR=0.99) • 11% lower LDL + 10% higher HDL in the hormone group compared with placebo • Time trend with more CHD events in the hormone group in year 1 and fewer in years 4 and 5 • More in the HRT group had venous thromboembolic events (34 vs. 12, RH 2.89) and gallbladder disease (84 vs. 62, RH 1.38) • No difference in total mortality 19 HERS Conclusions • Treatment with HRT did not reduce the overall rate of CHD events in postmenopausal women • HRT not recommended for secondary prevention 20 Almost 50% of Undiagnosed Postmenopausal Women Have Low Bone Mass Distribution of T-scores in NORA* 7% < -2.5 -1.0 to -2.5 40% 53% • A longitudinal observational study of osteoporosis among previously undiagnosed postmenopausal women > -1.0 • More than 200,000 women from 4,236 primary care practices participated Data available from Merck & Co., Inc. West Point, PA. DA-FOS65(1). *The National Osteoporosis Risk Assessment (NORA) Study was supported by Merck & Co., Inc. Forearm Relative BMD (%) 100 Spine Hip and Heel 90 80 70 60 30 40 50 60 70 80 Age Faulkner, KG. J Clin Densitom. 1998;1:279-285. 90 Annual Fracture Incidence BMD and Fracture Risk Are Inversely Related Colles' Vertebrae 4000 Hip 3000 2000 1000 0 3539 85+ Age Cooper C. Baillieres Clin Rheumatol.1993;7:459-477. Risk Factors for Osteoporotic Fracture Not Modifiable Potentially Modifiable Personal history of fracture as an adult Current cigarette smoking History of fracture in first-degree relative Estrogen deficiency, including menopause onset <age 45 Caucasian race Alcoholism Low body weight (<127 lbs) Low calcium intake (lifelong) Advanced age Female sex Impaired eyesight despite adequate correction Recurrent falls Dementia Poor health/frailty Inadequate physical activity Poor health/frailty Gold color denotes risk factors that are key factors for risk of hip fracture, independent of bone density. National Osteoporosis Foundation, Physician’s Guide to Prevention and Treatment of Osteoporosis. Belle Mead, NJ: Excerpta Medica, Inc; 1998. Hip Fractures Can Lead to Disability, Loss of Independence, and Even Death • Hip fracture is associated with increased risk of: – Disability: 50% never fully recover1,2 – Long-term nursing home care required: 25%2 – Increased mortality within 1 year: up to 24%3 – Lifetime risk of death: comparable to that of breast cancer4 1. Consensus Development Conference. Am J Med. 1993;94:646-650. 2. Riggs BL, Melton LJ III. Bone. 1995;17:505S-511S. 3. Ray NF et al. J Bone Miner Res. 1997;12(1):24-35. 4. Cummings SR et al. Arch Intern Med. 1989;149:2445-2448. Prevention of Osteoporotic Fractures • Clinical trials show 5 to 7% greater spinal bone density after 2-3 years in women randomized to HRT compared with placebo • OS suggest 50% lower risk of hip and other fractures in HRT users compared with nonusers • In a meta-analysis of 22 small trials, women randomized to HRT had a 27% lower risk of osteoporotic fracture compared with placebo • HERS trial showed no benefit for fracture outcomes after 4 years • Approved by FDA for prevention, but not treatment of osteoporosis 25 Central DXA Measurement • Measures multiple skeletal sites – – – – Spine Proximal femur Forearm Total body • Office based • Considered the clinical standard Visualizing a Patient’s T-Score 2 1 Peak Bone Mass SD 0 –1 –2 –3 –4 H T-score = –3.0 –5 –6 20 30 40 50 60 70 80 90 Age (years) T-score = Number of standard deviations (SDs) by which the patient’s bone mass falls above or below the mean peak bone mass for normal young adult women H = T-score for patient, a 60-year-old woman; here, T = –3.0 Light line: Change in mean bone mass over time for women Heavy line: Mean peak bone mass for young normal adult women National Osteoporosis Foundation, Physician’s Guide to Prevention and Treatment of Osteoporosis. Belle Mead, NJ: Excerpta Medica, Inc.; 1998 Interpreting BMD Measurement Reports T-Score Is Key • The most clinically relevant value on the BMD report • Describes bone mass compared with the mean peak bone mass of healthy young adult women in terms of Standard Deviation (SD) • Can help confirm the diagnosis of low bone mass or osteoporosis • For every SD below the young adult normal, the risk of fracture doubles Interpreting BMD Measurement Reports Some BMD Reports Also Include a Z-score • Describes a patient’s bone mass compared with the age-matched and sex-matched mean in terms of SD • Should not be used in the diagnosis of osteoporosis; a patient may have values that compare favorably with age-matched controls, but still be at increased risk for fracture National Osteoporosis Foundation, Physician’s Guide to Prevention and Treatment of Osteoporosis. Belle Mead, NJ: Excerpta Medica, Inc.; 1998 Increased Fracture Risk at T-Score of -2.0 A T-score of -2.0 at the spine or hip represents: • 20% reduction in bone mass (compared with mean BMD of normal young adult women) • 380% increase in fracture at the spine • 480% increase in fracture at the hip Recommendations for Treatment Based on BMD Testing Results National Osteoporosis Foundation Guidelines for Women T-SCORE ACTION –2.0 or less Initiate therapy –1.5 or less (with at least 1 additional risk factor) Initiate therapy National Osteoporosis Foundation, Physician’s Guide to Prevention and Treatment of Osteoporosis. Belle Mead, NJ: Excerpta Medica, Inc.; 1998 Breast Cancer • Multiple OS have found an risk of breast cancer among long-term hormone users (30-60%) • No risk among women who took estrogen for less than 5 years • Until WHI, no RCTs had addressed the risk of breast cancer among estrogen users 32 Women’s Health Initiative University of Iowa 33 Components • Preventive Clinical Trial – Hormone Replacement Therapy – Diet Modification – Calcium+Vitamin D Supplementation • Observational Study 34 WHI Estrogen+Progestin Trial Background circa 1992 Suspected benefits of hormones: • risk of CHD • risk of fracture • risk of colorectal cancer Suspected risks of hormones: • Possible risk of breast cancer • risk of VTE/PE 35 WHI Estrogen+Progestin Trial Specific Aims • To test whether E+P reduces the incidence of CHD and other CVD • To test whether E+P reduces the incidence of all osteoporosis-related fractures and hip fractures separately • To assess whether E+P increases the risk of breast cancer 36 Women’s Health Initiative Trial of Estrogen + Progestin Methods 37 WHI Estrogen+Progestin Trial Recruitment • National and local area media awareness campaigns • Population-based direct mailings to ageeligible women • Augmented by local recruitment strategies • 3 screening visits 38 Women’s Health Initiative Clinical Centers Fred Huthcinson Cancer Research Center Univ. of Minnesota Med. Ctr. Medical College of Wisconsin Kaiser Foundation Research Institute Univ. of Wisconsin Wayne State Univ. SUNY Buffalo Univ. of Mass Med. Ctr. Albert Einstein Brigham & Women’s Hosp. Col. of Med. Univ. of Iowa Mem. Hosp. of Rhode Is. Univ. of Pittsburgh Rush-Presb. Northwestern SUNY, Stony Brook Univ. St. Luke’s Ohio State Univ. Univ. of Med. & Dent. Med. Ctr. of New Jersey Univ. of California, Davis Univ. of Nevada, Reno Kaiser Foundation Research Institute Leland Stanford Junior University Medlantic Res. Inst./Howard Univ. George Washington Univ. Univ. of Cincinnati Medical Center Univ. of California, Los Angeles Univ. of California, Irvine Harbor-UCLA Research & Education Inst. Univ. of Tennessee Univ. of California, San Diego Bowman Gray School of Medicine Univ. of North Carolina Emory Univ. Sch. of Medicine Univ. of Alabama Univ. of Arizona at Tucson Univ. of Texas Health Science Ctr., San Antonio Univ. of Florida Baylor College of Medicine Univ. of Miami Univ. of Hawaii 39 I:\DOCUMENT\GRAPHICS\FIGURES\WHIMAP.PPT WHI Hormone Program Study Population: Inclusion criteria • Age 50-79 at baseline • Post menopausal, defined as: – No bleeding for >6 months (>12 months for 50-54 years old) – Current / prior use of menopausal hormones – Post hysterectomy with symptoms • Likely to reside in the clinic area for 3 years • Willing to provide written informed consent 40 WHI Hormone Program Design YES Conjugated equine estrogen (CEE) 0.625 mg/d N= 10,739 Placebo Hysterectomy NO N= 16,608 CEE 0.625 mg/d + medroxyprogesterone acetate 2.5 mg/d Placebo 41 WHI Estrogen+Progestin Trial Blinding • Treatment assignments unknown to participants, clinic staff and clinic investigators. • Unblinding discouraged unless necessary for safety or clinical management of participants. • When necessary, an unblinding officer provided the clinic gynecologist with treatment assignment. • Unblinding officers and clinic gynecologists were not involved with study outcomes activities. 42 WHI Estrogen+Progestin Trial Reasons for Permanent Discontinuation of Study Medication • Development of breast cancer • Endometrial cancer, atypia or hyperplasia not responsive to treatment • Deep vein thrombosis or PE • Malignant melanoma • Meningioma • Triglyceride level greater than 1000 mg/dL • Prescription of estrogen, testosterone or SERM 43 WHI outcomes confirmed by hospital records • CHD – MI requiring hospitalization or silent or coronary death • Stroke • Pulmonary embolism/DVT • Cancer • Hip, vertebral, and other osteoporotic fractures 44 WHI Estrogen+Progestin Trial Global Index • Defined to summarize important aspects of health benefits vs. risks • Defined for each woman as the earliest occurrence of CHD, invasive breast cancer, stroke, PE, endometrial cancer, colorectal cancer, hip fracture or death from other causes 45 Women’s Health Initiative Trial of Estrogen + Progestin Results 46 Profile of the Women’s Health Initiative Randomized Trial of Estrogen Plus Progestin in Women With an Intact Uterus Initiated screening (N = 373,092) Provided consent and reported no hysterectomy (N = 18,845) Randomized (N = 16,608) Estrogen +Progestin (N = 8,506) Status on 4/30/02 Alive/outcomes data submitted in last 18 months (n = 7,968) Unknown vital status (n = 307) Deceased (n = 231) Placebo (N = 8,102) Status on 4/30/02 Alive/outcomes data submitted in last 18 months (n = 7,608) Unknown vital status (n = 276) Deceased (n = 218) 47 Cumulative Drop-out and Drop-in Rates by Randomization Assignment and Follow-up Time 40 35 Percent 30 25 Drop-out Estrogen+Progestin Drop-out Placebo 20 Drop-in Estrogen+Progestin Drop-in Placebo 15 10 5 0 Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7 48 Kaplan-Meier Estimates of Cumulative Hazards for CHD The number of women at risk are presented below the horizontal axis for each treatment arm. 0.05 CHD 0.03 0.04 HR 1.29 nCI (1.02, 1.63) aCI (0.85, 1.97) 0.0 0.01 0.02 E+P Placebo Time (years) 1 2 3 4 5 6 7 E+P 8506 0 8353 8248 8133 7004 4251 2085 814 Placebo 8102 7999 7899 7789 6639 3948 1756 523 49 Kaplan-Meier Estimates of Cumulative Hazards for Stroke The number of women at risk are presented below the horizontal axis for each treatment arm. 0.05 Stroke 0.03 0.04 HR 1.41 nCI (1.07, 1.85) aCI (0.86, 2.31) 0.0 0.01 0.02 E+P Placebo Time (years) 1 2 3 4 5 6 7 E+P 8506 0 8375 8277 8155 7032 4272 2088 814 Placebo 8102 8005 7912 7804 6659 3960 1760 524 50 Kaplan-Meier Estimates of Cumulative Hazards for PE The number of women at risk are presented below the horizontal axis for each treatment arm. 0.05 PE 0.03 0.04 HR 2.13 nCI (1.39, 3.25) aCI (0.99, 4.56) 0.0 0.01 0.02 E+P Placebo Time (years) 1 2 3 4 5 6 7 E+P 8506 0 8364 8280 8174 7054 4295 2108 820 Placebo 8102 8013 7924 7825 6679 3973 1770 52651 Kaplan-Meier Estimates of Cumulative Hazards for Breast Cancer The number of women at risk are presented below the horizontal axis for each treatment arm. 0.05 Invasive Breast Cancer 0.03 0.04 HR 1.26 nCI (1.00, 1.59) aCI (0.83, 1.92) 0.0 0.01 0.02 E+P Placebo Time (years) 1 2 3 4 5 6 7 E+P 8506 0 8378 8277 8150 7000 4234 2064 801 Placebo 8102 8001 7891 7772 6619 3922 1740 52352 Kaplan-Meier Estimates of Cumulative Hazards for Colorectal Cancer The number of women at risk are presented below the horizontal axis for each treatment arm. 0.05 Colorectal Cancer 0.03 0.04 HR 0.63 nCI (0.43, 0.92) aCI (0.32, 1.24) 0.0 0.01 0.02 E+P Placebo Time (years) 1 2 3 4 5 6 7 E+P 8506 0 8379 8297 8194 7073 4305 2111 825 Placebo 8102 8003 7916 7814 6660 3958 1756 52253 Kaplan-Meier Estimates of Cumulative Hazards for Hip Fracture The number of women at risk are presented below the horizontal axis for each treatment arm. 0.05 Hip Fracture 0.03 0.04 HR 0.66 nCI (0.45, 0.98) aCI (0.33, 1.33) 0.0 0.01 0.02 E+P Placebo Time (years) 1 2 3 4 5 6 7 E+P 8506 0 8382 8299 8190 7073 4305 2116 826 Placebo 8102 8009 7915 7807 6659 3958 1763 525 54 Kaplan-Meier Estimates of Cumulative Hazards for Death The number of women at risk are presented below the horizontal axis for each treatment arm. 0.15 Death 0.10 HR 0.98 nCI (0.82, 1.18) aCI (0.70, 1.37) 0.0 0.05 E+P Placebo Time (years) 1 2 3 4 5 6 7 E+P 8506 0 8388 8313 8214 7095 4320 2121 828 Placebo 8102 8018 7936 7840 6697 3985 1777 53055 1.29 1.26 1.41 2.11 0.63 0.67 56 Breast Cancer Outcome (Annualized Percentages) by Prior Postmenopausal Hormone Use Estrogen+Progestin Placebo Hazard Ratio 95% Nominal CI Years of Prior Use Never used 114 (0.35%) 102 (0.33%) 1.06 (0.81,1.38) <5 32 (0.39%) 15 (0.20%) 2.13 (1.15,3.94) 5 - <10 11 (0.49%) 2 (0.11%) 4.61 (1.01,21.02) 5 (0.40%) 1.81 (0.60,5.43) >10 9 (0.69%) Test for trend, p=0.03 57 Sensitivity Analysis of Selected Outcomes to Actual Use* Hazard Ratio * 95% Nominal CI CHD 1.51 (1.13,2.01) Stroke 1.67 (1.17,2.40) VTE 3.29 (2.25,4.82) Invasive breast cancer 1.49 (1.10,2.02) Censored 6 months after becoming non-adherent (using <80%, or stopping pills) 58 Attributable Risk Summary • Excess risk per 10,000 person-years on E+P – 7 more women with CHD – 8 more women with stroke – 8 more women with PE – 8 more women with breast cancer • Risk reduction per 10,000 person-years on E+P – 6 fewer colorectal cancer – 5 fewer hip fractures • Summary: 19 additional monitored events per 10,000 person years on E+P 59 WHI Estrogen+Progestin Trial Summary • Treatment with estrogen plus progestin for up to 5 years is not beneficial overall. • There is early harm for CHD, continuing harm for stroke and VTE, and increasing harm for breast cancer. • This risk-benefit profile is not consistent with a viable intervention for primary prevention of chronic diseases in postmenopausal women. 60 WHI Estrogen+Progestin Trial Summary • This trial did not address the use of estrogen plus progestin for short-term relief of menopausal symptoms. 61 WHI Estrogen+Progestin Trial Limitations • Still undetermined is: – Effects of other doses, formulations or routes of administration – Effects of progestin separate from estrogen – Longer term assessment of risks and benefits • Rates of discontinuation in the active treatment arm may have diluted the observed risks and benefits. • Early stopping limits precision of the results. 62 WHI Estrogen+Progestin Trial Implications • Estrogen plus progestin should not be initiated or continued for the primary prevention of CHD. • The risks for CHD, stroke, PE and breast cancer must be weighed against the benefit for fracture in selecting from the available agents to prevent osteoporosis. 63 64 Why the Differences Between Observational Studies and RCTs for CAD? • OS may produce the wrong answer if there are unmeasured differences between hormone users and nonusers • Women who take HRT are generally healthier and wealthier than nonusers • Adherence has been shown to be a strong marker for low risk of coronary events, even when adherence is to a placebo • Issue of 1º versus 2º prevention of CAD • Randomization helps eliminate these and other potential biases 65 Clinical Issues – Prevention of: • • • • Hot flashes Heart disease Osteoporosis Breast cancer 66 Hot flashes • Estrogen works! • Short term use (< 2 years minimal absolute risk) 67 Other Post-menopausal Prevention Choices Heart disease Osteoporotic fx Vertebral Non-vertebral Breast cancer DVT Rate of hot flashes Vaginal bleeding Alendronate Raloxifene No effect No effect 0.45 0.50 No effect No effect No effect None 0.50 0.9* 0.24 3.1 30% (worsen) Rare * not statistically significant 68 Heart Disease Prevention In NHS cohort, 82% of CAD cases could be eliminated if the population adhered to basic behavioral guidelines… – Exercise – Healthy diet – Normal weight – No smoking – Moderate alcohol consumption 69 Osteoporosis Prevention • • • • Weight bearing exercise 1500 mg calcium daily + 400 IU Vit D At least normal body weight No smoking 70 Summary: Healthy lifestyle choices may be the best medicine 71