Smoking and Tobacco - Part 1
advertisement

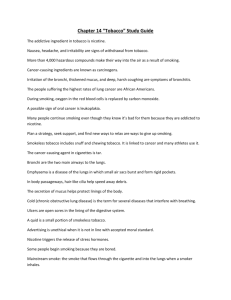
Smoking and Tobacco Part 1 Health Risks Epidemiology Pharmacology of nicotine dependence © 2010 University of Sydney Learning objectives To be able to: • Recognise population impact of tobacco use • Understand pharmacology of nicotine • Describe factors contributing to dependence on tobacco smoking • Describe benefits of smoking cessation What is a cigarette? • Cigarettes have long since been simple dried tobacco • ‘Tobacco’ in a cigarette is remanufactured leaf – Fillers and expanders are added – bits of plant stem and scraps and solidified tobacco dust – The leaf is designed with the cigarette paper to burn in a predictable and consistent fashion – This reduces cigarette-to-cigarette variations • There is an uncertain number of additives that have a variety of putative roles – Ease the otherwise irritating effect of smoke – Increase the speed of nicotine delivery • Highly addictive modern cigarette was developed and extensively taste/effect tested in the 1950s-1970s. Smoking in Australia Tobacco Smoking: Harms • Major preventable cause of premature morbidity and mortality in Australia and throughout the world • Major risk factor for a number of diseases and conditions, including: – – – – coronary heart disease stroke peripheral vascular disease and cancer1 • Types of cancer: – of the mouth, larynx, oesophagus, lung, stomach, pancreas, kidney, urinary bladder, uterine cervix and leukemia2 1AIHW (2008). Australia’s health 2008. JA, et al (2009) “The Pharmacology of Nicotine and Tobacco” in Principles of Addiction Medicine. 4th edition 2Dani Tobacco Smoking: Harms (cont) • Increases risk of developing: – Respiratory tract infections • Influenza, pneumococcal pneumonia, TB – Peptic ulcers – Cataracts, macular degeneration1 • Gender specific risks – In women: • Low levels of oestrogen, early menopause, osteoporosis • In pregnancy – risk of spontaneous abortion and perinatal mortality. Morbidity increased by one third and the risk of having a low birth weight infant is doubled. – In men: • Erectile dysfunction, primarily in people with underlying vascular disease and with coronary artery disease and hypertension.1 1Dani J et al (2009) Smoking: any health benefits? • Possibly reduces symptom severity in schizophrenia (self-medication hypothesis) – There is deficient endogenous central nicotinic neurotransmission in schizophrenia, which causes a disruption of sensory gating (a possible mechanism for delusions). – Exogenous nicotine partly compensates for this deficiency. – Schizophrenic patients smoke larger amounts of cigarettes per day and extract more nicotine from them – significant health risk. – Therapeutic use of safe forms of nicotine in schizophrenia has been proposed.1 • Reduces risk of Parkinson’s disease – Benefit correlates with the intensity and duration of smoking. – Does not appear to be due to publication bias. 2 • Does it reduce prevalence of Alzheimer’s disease? – After controlling for tobacco industry affiliation, smoking has been found to increase the risk of Alzheimer’s disease, RR -1.72.3 1Conway JL. (2009) Med Hypotheses. 73(2):259-62. M, et al (2009) Biochem Pharmacol. Oct 1;78(7):677-85. 3Cataldo et al (2009) J Alzheimers Dis. Oct 8. [Epub]. 2Quik Tobacco Smoking: Costs • In Australia, tobacco smoking was responsible for 7.8% of the total burden of disease in 2003 – Lung cancer, chronic obstructive pulmonary disease and ischemic heart disease account for more than 3/4 of this burden1 • Estimated tangible costs of tobacco use in 2004–05 were $10.8 billion (about 1.3% of gross domestic product)2 1Begg S, et al (2007). The burden of disease and injury in Australia 2003. DJ and Lapsley HM (2008). The costs of tobacco, alcohol and illicit drug abuse to Australian Society in 2004/05. 2Collins Annual death and burden due to tobacco Note: DALY = ‘Disability-adjusted life year’ • Key measure of total burden of disease and injury. • Describes years of life lost due to premature death plus years of ‘healthy’ life lost due to disability. Begg S, et al (2007). The burden of disease and injury in Australia 2003. AIHW. Lung cancer mortality, Australia 1910–2004 • Age-standardised rates per 100,000 persons (World Standard Population) Source: Scollo, M and Winstanley, M [eds]. (2008) Tobacco in Australia: Facts and Issues. Third Edition. Cancer Council Victoria. Deaths due to smoking • Incidence is falling in men but remain relatively constant in women Source: NSW Health, Population Health Division. The health of the people of New South Wales - Report of the Chief Health Officer. © - Copyright - New South Wales Health Department for and on behalf of the Crown in right of the State of New South Wales Tobacco Control • The falls in COPD and lung cancer deaths in Australia are largely attributed to tobacco control. • Australia ranks with Sweden, Canada and the USA as having achieved the largest falls in daily smoking prevalence of any nation. Scollo, M and Winstanley, M (2008) Tobacco in Australia: Facts and Issues. 3rd Ed. Public Health Approaches to Tobacco Control • Restricting access by regulation of supply • Prohibition (selective or total) • Taxation to increase price • Demand reduction • e.g. reducing acceptability of smoking • Warning labels • Harm reduction • ?Snuff tobacco Some Australian achievements in Tobacco Control • Restrictions on advertising and promotion – TV/radio – Print – Elimination of sports and ‘cultural’ sponsorship • Public places and workplace legislation – Workplaces – Sporting stadiums – Pubs/clubs – Outdoor places (beaches and parks) Some Australian achievements in Tobacco Control (cont) • Innovative mass media and counter-advertising – e.g. successful bubblewrap/COPD campaign • Increased private smoke-free places – Smoke-free homes – Smoke-free cars • Graphic pack warnings • (Some) point-of-sale initiatives Tobacco Control in Australia: Major events and tobacco sales Major events in tobacco control and tobacco products dutied for sale per person 15 years and over, Australia, 1906 -2006, (grams) Source: Scollo, M and Winstanley, M (2008). Tobacco in Australia: Facts and Issues. 3rd Edition. Cancer Council Victoria. Current patterns • Overall smoking rate has been declining. • In the 1950s an estimated 70% of males and 30% of females smoked. • Currently 1 in 6 Australians aged 14 years and over smokes (16.6%). – Daily smoking rate is 18% in males and 15% in females AIHW (2008). 2007 NDS Household Survey Daily smoking rate Source: AIHW (2008). ‘Australia’s health 2008’, cat. no. AUS 99 Daily smoking 2007 by State/Territory 30 Males 25 Females 20 15 10 5 0 WA SA NSW ACT VIC Aust QLD TAS NT Data Source: AIHW (2008). 2007 NDS Household Survey: State and territory supplement. Youth Daily Smoking 2007 (ages 14-19) 25 Males 20 Females 15 10 5 0 SA WA VIC Aust NSW QLD ACT TAS NT Data Source: AIHW (2008). 2007 NDS Household Survey: State and territory supplement. Total community smoking burden • Daily smokers – Male – Female 1.54M 1.33M • Less than daily smokers – Male – Female 0.26M 0.21M – Ex-smokers – Never smokers 4.33M 9.55M AIHW (2008). 2007 NDS Household Survey: detailed findings. Specific populations • Smoking is more common in the following groups: – People from lower economic background • 26% with the lowest status reported regular smoking versus 14% with the highest status. – Living in remote areas • 25% of people living in remote areas compared with 18% for people in major cities. – Unemployed • 38% compared to 22% (employed) or 9% (students) – People from the Aboriginal and Torres Strait Islander background • 34% versus 19% (other Australians) AIHW (2008). 2007 NDS Household Survey: detailed findings. Smoking in Indigenous population • Rates are more than double those in general population1 – Males 51% – Females 47% – No change since 1994 • Causes 12% of the burden of injury and disease due to smoking in males and 7% in females1 – Population comparisons 9.5% & 6% respectively • Smoking during pregnancy is very common – up to 72%2 1Trewin D (2006) National Aboriginal and Torres Strait Islander Health Survey: Australia, 2004–05. 2Ivers R. (2001) Indigenous Australians and Tobacco: a literature review. • Higher prevalence of smoking in remote Indigenous communities AIHW (2008). Indicators for chronic diseases and their determinants. Smoking and Mental Health • People with psychiatric disorders and substance use disorders have 2-4 times higher rates of smoking (range 41% and 67% respectively) than the general population. • 40-88% of patients with schizophrenia smoke. Kalman D et al(2005). American Journal on Addictions,14:106-123. Smoking and Mental Health (cont) • Among current smokers in general population: – ~ 41% report having a mental health diagnosis in the last month.2 – 60% report a past or current history (ever history) of a mental health diagnosis sometime in their lifetime.1 – the most common mental health diagnoses include:2 • • • • Alcohol abuse Major Depressive Disorder Anxiety disorders: simple phobias and social phobias Substance Abuse • Among those seeking help to stop smoking3: – 30% are likely to have a history of depression – 20% are likely to be using alcohol or other drugs 1Kalman D et al(2005). American Journal on Addictions,14:106-123. 2 Lasser K, et al. (2000) JAMA, 284:2606-2610. 3Zwar N, et al (2004). Smoking Cessation Guidelines for Australian General Practice. Pharmacology of nicotine and neurobiology of nicotine dependence Nicotine • Naturally occurring alkaloid – Serves as insecticide in many plants • Major CNS active compound in tobacco smoke • Nicotinic cholinergic receptor agonist • In humans acts mainly as a psychostimulant and mood modulator. Nicotinic Acetylcholine Receptors (nAChRs) • Ligand-gated ion channels (mostly Na+/K+ ) • Widespread in the CNS • Acetylcholine (Ach) is the endogenous ligand • The major role in mammalian CNS is to influence neurotransmitter release. Dani et al (2009) Principles of Addiction Medicine. 4th Ed. nAChR structure • Pentamer – 5 polypeptide subunits – 9 subtypes – Potential for 59 = 2 million different assemblies • Nicotine is a potent agonist at the nicotinic 42 receptor β2 α4 β2 α4 β2 • Nicotine dependence is modulated primarily through 42 nACh receptors – In 2-subunit knock-out mice nicotine does not produce reinforcing effect (less dopamine is released and mice do not self-administer nicotine).1 – Alterations in 4 structure change the receptor sensitivity to nicotine2 1Mineur 2Tapper YS and Picciotto MR (2008) Biochem Pharmacol, 75:323-333. AR, et al. (2004) Science, 306:1029-1032. nAChRs: functional states • Three states of the nAChR ion channels: – closed (at rest) – open (cations flow into the cell) – desensitised (closed and not responsive to agonists) Dani JA, et al (2009) Receptor activation • Ach (or nicotine) binds to the receptor and stabilises the open state of the ion channel for several milliseconds. • Cations (Na+ and K+) enter and depolarise the cell initiating cellular response • A variety of neurotransmitters are released in the CNS as presynaptic nAChRs are present on various types of neurons. • ACh is rapidly broken down by acetylcholine-esterase • Nicotine has much longer duration of effect than ACh • Receptor becomes de-sensitised and unresponsive for a period of time Dani JA, et al (2009) nAChRs with repeated smoking • Between cigarettes nAChRs are mainly desensitised (acute tolerance). • Next cigarette activates a small pool of receptors that are still responsive, producing pleasurable effects. • In chronic smokers (e.g. with daily smoking for 6 months or longer): – – – – Tolerance Withdrawal syndrome on cessation of smoking Long-term desensitisation of nAChRs Increase in receptor density (upregulation of nAChRs) as a compensatory response to desensitisation of the large proportion the total number of nAChRs receptors. Nicotine effects • Releases multiple neurotransmitters in the CNS, including: – ACh, dopamine, noradrenaline, GABA, serotonin and glutamate • Produces CNS stimulatory effects: – Increased arousal, decreased fatigue, decreased appetite – Improved attention, concentration and cognitive function – Euphoria and increased sense of wellbeing • Decreases anxiety (particularly in stressful situations) and reduces muscle tension – important effects that are perceived as beneficial by smokers Reinforcement • Reinforcing effect is mediated mostly via activation of the dopaminergic neurones and release of dopamine in the mesolimbic reward pathway – Ventral Tegmental Area - Nucleus Accumbens - Prefrontal Cortex • These areas have high concentrations of nAChRs, both presynaptic and postsynaptic. Other effects • Sympathetic stimulation – Increased heart rate and blood pressure • Some unpleasant effects occur at initiation of smoking, but tolerance to these effects quickly develops if smoking is continued – nausea, headache, dizziness Nicotine pharmacokinetics: Absorption • Inhaled nicotine is quickly absorbed from the large surface area of the alveoli into the pulmonary veins • Rapidly enters the arterial system – Time to arterial peak is less than 10 seconds • Easily crosses blood-brain barrier and begins to reach nAchRs in ~20 seconds • Crosses the placenta freely • Appears in breast milk in concentrations ~x2 those found in blood Dani JA, et al (2009) Nicotine metabolism • Extensively metabolised in the liver • CYP2A6 is the major enzyme involved • Major metabolite: cotinine – ~ 80% of nicotine converted to cotinine – long half-life: 20 hours – appears in urine • Induction of CYP2A6 enzyme may enhance clearance and contribute to metabolic tolerance • Metabolism of nicotine is faster during pregnancy and in women on estrogen containing contraceptive pill or hormone replacement therapy (estrogen is the CYP2A6 inducer). Dani JA, et al (2009) Nicotine plasma concentration • Each cigarette delivers 1.2-2.9mg of nicotine • A typical pack-a-day smoker absorbs 20-40mg of nicotine each day • Half-life is ~ 2hours • During a typical day, nicotine accumulates over 6-8 hours (3-4 half-lives) • The increment is 5-30ng/ml after each cigarette (depending on how the cigarette is smoked) • More frequent smoking reduces fluctuations in nicotine plasma concentration • The plateau (10-50ng/ml) is usually reached in the early afternoon Dani JA, et al (2009) Nicotine plasma concentrations Smoking 3 cigs/hour Russel MA and Feyerabend C (1978) Cigarette smoking: a dependence on high-nicotine boli. Drug Metabolism Review. 8(1):29-57. © 1978. Reprinted by permission of Taylor & Francis. How smokers titrate their dose of nicotine • Smokers control nicotine intake to achieve desired effect by altering: – the puff volume – the number of puffs they take from a cigarette – the depth of inhalation • Initial puffs are rapid and deep to achieve rapid nicotine delivery • Smokers tend to take smaller puffs towards the end of a cigarette (when desired nicotine has been delivered) to titrate the dose Nicotine withdrawal • Nicotine plasma concentration significantly drops overnight, which leads to withdrawal symptoms in the morning in chronic smokers. • Withdrawal onset is usually within a few hours after last cigarette • Nicotine withdrawal syndrome includes: – Mood changes • dysphoria, depressive mood – – – – – Irritability, frustration or anger Anxiety, restlessness Difficulty concentrating, impaired attention Hunger, increased appetite or weight gain Craving Nicotine withdrawal (cont) • First morning cigarette produces the most pleasurable effect – After an overnight abstinence more receptors become available for activation – It also relieves withdrawal symptoms • The earlier the smoker begins to smoke after waking in the morning the more severe the dependence • If abstinence continues, withdrawal symptoms peak at 24-48 hours and gradually subside over several weeks. • Some symptoms persist for months – mild depression, dysphoria and anhedonia Dani JA, et al (2009) Cycles of pleasure and withdrawal Nicotine used for pleasure, enhanced performance, mood regulation Tolerance and physical dependence1,2 • Initial activation causes pleasure response but… • Dopamine falls quickly over the next 2 hours • As levels fall the smoker feels displeasure or withdrawal • The next cigarette reduces the cravings and other withdrawal symptoms and produces some positive effects • This reinforces the compulsion to smoke • Environmental cues are also important in producing addiction Nicotine used to self-medicate withdrawal symptoms1 Abstinence produces withdrawal symptoms and cravings1 1Jarvis MJ. (2004) BMJ, 328:277-279. VI (1997) Nature, 390:401-404. 2Pidoplichko Standard Elements of Dependence • Context • Ritual behaviours • Sensory stimulation • Reinforcing (nicotine) stimulus Context • Some places, times and situations are closely associated with smoking and enhance craving: – Morning coffee with breakfast – Coffee shop – Tea breaks • Some places and situations are now negatively associated and cravings can be less severe: – – – – – Places of worship Sporting stadiums In aircraft Smoke-free homes Around children Ritual behaviours • Going to a place where smoking is possible • Accessing the cigarette – e.g. opening handbag • Getting match or lighter • Lighting cigarette Sensory stimuli • Touch/feel of cigarette • Light from flame • Smell of smoke • Direct airway stimulation from smoke – Anaesthetising the airway reduces reported smoking satisfaction • These all travel to brain at nerve speed preceding the arrival of nicotine Addictive qualities • Fast absorption of nicotine and short time needed to reach receptor targets (and hence to exert pleasurable effects) are important factors in development of addiction • When linked with context/ritual/sensory stimuli they produce a strong reinforcing effect • In animals, random boluses of IV nicotine without the context associations cannot establish addiction and self-administration of nicotine does not occur. Individual variability • Smokers with low level of dependence or non-dependent: – Smoke small number of cigarettes per day – First cigarette delayed – Frequent periods off smoking – cold turkey each time – Minimal withdrawal symptoms • Majority of regular smokers have moderate-to-severe dependence and find it difficult to stop or cut down Genetics • Heritability ~50% (range 28-84%)1 • Effect of gene polymorphisms – People with defective alleles of CYP2A6 gene have slow metabolism of nicotine and lower rates of smoking and tobacco dependence.1 – People with CHRNA4 gene polymorphism (gene coding for α4 subunit of the nicotinic Ach receptor) have higher rates of tobacco dependence.2 1Schnoll et al. (2007) Curr Psychiatry Rep, 9:349-357. et al. (2007) Arch Gen Psychiatry, 64(9):1078-1086. 2Hutchison Health Benefits of smoking cessation If smoking continues • Risk of further illness is greatly increased1 – Second heart attacks are more common amongst cardiac patients if they continue to smoke. – Increased risk of a second cancer in people with successfully treated cancers who continue to smoke – Diabetics who smoke increase their risk of cardiovascular disease, peripheral vascular disease, progression of neuropathy and nephropathy. – There is a clear relationship between continued smoking and progression of COPD. 1Zwar N, et al (2004). Smoking Cessation Guidelines for Australian General Practice. Recent smokers - attempts to quit/cut down1 • Most smokers regret having started smoking and have made at least one attempt to quit. • A third of recent smokers reported decrease in the number of cigarettes smoked in the previous year.1 1AIHW (2008). 2007 NDS Household Survey Motivating Factors • Major motivating factors – health or fitness and cost AIHW (2008). 2007 NDS Household Survey. Smoking reduction: Ineffective Strategies • 1) Smoking cigarettes with reduced tar and nicotine delivery • 2) Reducing number of cigarettes smoked in a day (as a life-time strategy) • Neither strategy significantly reduces exposure to smoke • Smokers compensate for reduced delivery of nicotine:1 – By taking more frequent and deeper breaths – Increasing smoke intake by blocking the ventilation holes of the filter with their fingers or their lips 1Dani JA, et al (2009) Reduced Tar Cigarettes: Effect on the hazard ratio for lung cancer Source: Harris et al (2004) BMJ, 328:1-8 © BMJ. Reproduced with permission from BMJ Publishing Group. Smoking Fewer Cigarettes Copenhagen Studies • N=19,732 (from 3 studies) – Examined between 1967 and 1988 – Reexaminations at 5 to 10 year intervals – Mean follow-up of 15.5 years • Three groups – Continued smokers of >15 cigs/day – Reducers of >50% – Quitters • Reducers vs. continuing smokers – – – – CV disease Resp. disease Tobacco cancers All-cause mortality HR = 1.01 (0.76-1.35) HR = 1.20 (0.70- 2.07) HR = 0.91 (0.63-1.31) HR = 1.02 (0.89-1.17) Godtfredsen et al (2002) Am J Epidemiol, 156:994-1001. Quitters 0.88 0.77 0.36 0.65 Smoking cessation • Benefits are seen quickly – 5 Days • Sense of taste and smell improve – 6 Weeks • Safer surgery with fewer wound infections • Improved control of asthma – 3 Months • Cilia begin to recover and lung function improves – 1 year • Risk of coronary heart disease is halved compared to continuing smokers Zwar N, et al (2004). Smoking Cessation Guidelines for Australian General Practice. Benefits timeline (cont.) • 10 years: – Risk of lung cancer is less than half that of a continuing smoker and continues to decline • 10-15 years: – Risk of coronary heart disease the same as a non-smoker – All-causes of mortality decline to the same level as people who have never smoked. • In addition: – Women who quit before or in the early months of pregnancy have the same risk of having a low birth-weight baby as women who have never smoked. – Quitting slows the rate of loss of lung capacity in chronic airways disease – Improved appearance of skin and fitness – Saves money - based on one $10 pack of cigarettes per day: 1 year the cost is $3,650, over 5 years: $18,250. Zwar N, et al (2004). Conclusions (1) • Smoking is the leading cause of preventable illness and premature death. • The majority of smokers consider the health risks of smoking. • Nicotine is the main addictive substance in tobacco smoke. • Nicotine is rapidly delivered to the target receptors in the brain. • Nicotine activates ACh receptors in the CNS stimulating release of an array of neurotransmitters including dopamine. • It produces mostly stimulant effects but also relieves anxiety and muscle tension. Conclusions (2) • Cigarette smoking is highly addictive when linked with environmental cues. • Abstinence from smoking results in a withdrawal syndrome in dependent smokers. • Most smokers have tried to quit or alter their pattern of smoking in a way that they believe is healthy. • Benefits of smoking cessation are evident as early as several days of stopping. • After 10-15 years the risk of morbidity and mortality is the same as in people who never smoked. Case Study • John, aged 39 presents with his third chest infection in 12 months. He reports that despite two attempts to quit, he is still smoking a pack a day. He is not motivated to quit because ‘it‘s just too hard to do it right now’. He is under stress at work and needs his cigarettes. He now requests a prescription for antibiotics. • How important is it for John to stop smoking? • What would you say to John about benefits of smoking cessation? • How soon after quitting could he expect to see health risks reduce to non-smoker levels? • What are the major motivating factors for quitting? Case Study Answers • If John continues smoking: – antibiotics prescribed for current chest infection will be less effective – he is likely to suffer from more chest infections and may develop COPD in future – increased risk for lung cancer, cancer of other organs, cardiovascular disease, stroke, peripheral vascular disease, peptic ulcer, cataracts etc • Benefits of quitting: – – seen as early as 5-6 weeks after quitting. immune function will improve and he will be less likely to suffer from chest infections. – Health risks return to non-smoker levels after 10-15 years of abstinence. • Major motivating factors for quitting are health or fitness and cost. Contributors Dr Olga Lopatko University of Sydney Clinical A/Professor Matthew Peters Concord Hospital & University of Sydney All images used with permission, where applicable