Informal service providers of health care_ Recognition & Legitimacy
advertisement

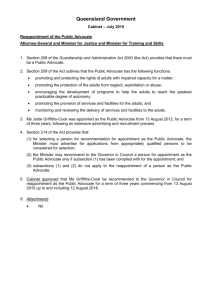
Informal Service Providers of Health Care Recognition & Legitimacy 21/03/14 Legal Framework Indira Unninayar, Advocate 21/03/14 Legal Framework Indira Unninayar, Advocate RURAL & URBAN POOR WHO ARE 80% POPULATION Facts Summary •Public healthcare infrastructure is 1/3rd to 1/6th of what is recommended •80% of healthcare is CURATIVE instead of being PREVENTIVE •Most healthcare is out of pocket; 2.2% / 60 lakh Indians are pushed below poverty line every year 21/03/14 Legal Framework Indira Unninayar, Advocate Expenditure on Healthcare 21/03/14 Legal Framework Indira Unninayar, Advocate Informal Healthcare Providers (Estimates) •For every 1,00,000 (1 lakh) : – There are ONLY 62.5 qualified doctors in India – Of which there are ONLY 5 in Rural India – And 197 in Urban India •For a total population of 1.21 billion: • Only 6,00,000 qualified doctors practice allopathy PLUS • 6,00,000 qualified doctors practice Ayurveda, Homeopathy, Unani, Sidha PLUS • 10-15 lakh Informal Providers practice healthcare • BUT Informal Providers are not ‘recognized’ and lack ‘legitimacy’ 21/03/14 Legal Framework Indira Unninayar, Advocate Necessary numbers • For every 1,000 population: – – – – – – India has .6 physicians + 1 nurses/midwives U.S. has 2.4 physicians + 9.8 nurses/midwives U.K. has 2.8 physicians + 9.8 nurses/midwives Brazil has 1.8 physicians + 6.4 nurses/midwives China has 1.8 physicians + 1.7 nurses/midwives Singapore has 1.9 physicians + 6.4 nurses/midwives • To achieve MDG Goals : • Need a minimum of 2.3 physicians, nurses, midwives • Less is a recipe for failure 21/03/14 Legal Framework Indira Unninayar, Advocate Situation Today Healthcare CRISIS in India Right to Health – a fundamental right, stands seriously violated for most Indians HEALTHCARE CRISIS IS ALSO A POVERTY ISSUE 21/03/14 Legal Framework Indira Unninayar, Advocate Question • Low utilization of Primary OPD Public Healthcare is because of long distances, inconvenient opening hours, lengthy waiting, staff absenteeism, poor availability of medicines, and poor quality of care •Informal Healthcare Providers are already filling several of these gaps •Q: Can the State formally utilize this readily available resource with Recognition & Legitimacy? 21/03/14 Legal Framework Indira Unninayar, Advocate Constitutional Mandates Above all laws 21/03/14 Legal Framework Indira Unninayar, Advocate Preamble •Relevant portions: – – – – SOCIALIST JUSTICE, social, economic EQUALITY of status and opportunity Dignity of the individual •Is the ‘basic structure’ of the Constitution •Aims - to end poverty, ignorance, disease and inequality of opportunity •Enables legislation or executive action – To remove inequalities – To protect interests of weaker/vulnerable sections of society 21/03/14 Legal Framework Indira Unninayar, Advocate Fundamental Rights (Part III) • Inalienable, guaranteed by State • Article 12 – Government, Parliament – Government, Legislature of each State – All local or other authorities in India or under the control of the GOI • Article 13 – All laws inconsistent with this part shall be void – The State shall not make any law which takes away or abridges the rights conferred by this part • Article 14 (against arbitrariness, discrimination) – The State shall not deny to any person equality before the law or the equal protection of the laws in India • Article 21 (right to health, medical services) – No person shall be deprived of his life or personal liberty except according to procedure established by law 21/03/14 Legal Framework Indira Unninayar, Advocate Fundamental Rights (Part III) - NOT TO BE USED - • Article 19(1)(g) - Protection of certain rights regarding freedom of speech, etc. (g) to practise any profession, or to carry on any occupation, trade or business • Article 19(6) – Nothing in sub-clause (g) shall affect the operation of any existing law in so far as it imposes, or prevent the State from making any law imposing, in the interests of the general public reasonable restrictions on the exercise of the rights conferred by the said sub-clause, and, in particular, nothing in the said sub-clause, shall affect the operation of any existing law in so far as it relates to or prevent the State from making any law relating to,(i)the professional or technical qualifications necessary for practising any profession or carrying on any occupation, trade or business, or (ii) the carrying on by the State, or by a corporation owned or controlled by the State, of any trade, business, industry or service, whether to the exclusion, complete or partial, of citizens or otherwise. 21/03/14 Legal Framework Indira Unninayar, Advocate Fundamental Rights (Part III) • Article 15 - Prohibition of discrimination on grounds of religion, race, caste, sex or place of birth (5) Nothing in this article or in 19(1)(g) shall prevent the State from making any special provision, by law, for the advancement of any socially and educationally backward classes of citizens or for SC or ST, in so far as such special provisions related to admission to educational institutions including private educational institutions whether aided or unaided by the State • Article 23 Prohibition of traffic in human beings and forced labour – (2) Nothing in this article shall prevent the State from imposing compulsory service for public purposes, and in imposing such service the State shall not make any discrimination on grounds only of religion, race, caste or class or any of them. 21/03/14 Legal Framework Indira Unninayar, Advocate Enforcement/Realization of Fundamental Rights (Part III) • Article 32 – Supreme Court • Article 226 – High Courts Anyone can move the courts 21/03/14 Legal Framework Indira Unninayar, Advocate Directive Principles of State Policy (Part IV) - OBLIGATION ON STATE • Article 37 – Though the provisions are not enforceable by any court, but the principles therein laid down are nevertheless fundamental in the governance of the country and it shall be the duty of the State to apply these principles in making laws. • Article 38 – (1) State shall strive to promote the welfare of the people by securing and protecting as effectively as it may a social order in which justice, social, economic and political, shall inform all the institutions of national life (2) The State shall, in particular, strive to minimize inequalities in status, facilities and opportunities, not only amongst individuals, but also amongst groups of people residing in different areas or engaged in different vocations • Article 39 – Certain principles of policy to be followed by the State – The State shall, in particular, direct its policy towards securing(e) that the health and strength of workers, men and women, and the tender age of children are not abused and that citizens are not forced by economic necessity to enter avocations unsuited to their age or strength (f) that children are given opportunities and facilities to develop in a healthy manner and in conditions of freedom and dignity and that childhood and youth are protected against exploitation and against moral and material abandonment (b) that the ownership and control of material resources of the community are so distributed as to best serve the common good (c) that the operation of the economic system does not result in the concentration of wealth and means of production to the common detriment 21/03/14 Legal Framework Indira Unninayar, Advocate Directive Principles of State Policy (Part IV) • Article 41 – Right to work, to education and to public assistance in certain cases – The State shall, within the limits of its economic capacity and development, make effective provision for securing the right to work, to education and to public assistance in cases of unemployment, old age, sickness and disablement, and in other cases of undeserved want • Article 42 – The State shall make provision for securing just and humane conditions of work and for maternity relief • Article 47 – Duty of the State to raise the level of nutrition and the standard of living to improve public health - The State shall regard the raising of the level of nutrition and the standard of living of its people and the improvement of public health as among its primary duties and, in particular, the State shall endeavour to bring about prohibition of the consumption except for medicinal purposes of intoxicating drinks and of drugs which are injurious to health. • 51. The State shall endeavour to— (c) foster respect for international law and treaty obligations in the dealings of organized peoples with one another; and 21/03/14 Legal Framework Indira Unninayar, Advocate Fundamental Duties (Part IVA) • Article 51A - It shall be the duty of every citizen of India— • (h) to develop the scientific temper, humanism and the spirit of inquiry and reform; • (i) to safeguard public property and to abjure violence; • (j) to strive towards excellence in all spheres of individual and collective activity so that the nation constantly rises to higher levels of endeavour and achievement; 21/03/14 Legal Framework Indira Unninayar, Advocate Jurisdiction I (Union) 64. Institutions declared by law to be of national importance (63 – BHU, AMU & DU) 65. Union agencies and institutions for(a)professional, vocational or technical training… (b) promotion of special studies or research 66. Co-ordination and determination of standards in institutions for higher education or research and scientific and technical institutions 21/03/14 II (State) 6. Public health and sanitation, hospitals and dispensaries 64. Offences against laws with respect to any of the matters in this list III (Concurrent) 19. Drugs and poisons, subject to … 20 Economic and social planning 20A Population control and family planning 25. Education, including technical education, medical education and universities subject to List I (63-66) 26. Legal, medical and other professions 29. Prevention of extension of one State to another, of infectious or contagious diseases or pests affecting men, animals or plants. 30. Vital statistics including registration of births and deaths Legal Framework Indira Unninayar, Advocate Health – WHO definition • ‘Health’ is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity • INVOKE INTERNATIONAL CONVENTIONS • COURTS ARE QUITE IGNORANT ABOUT GROUND REALITIES • USE THEIR OWN JUDGMENTS 21/03/14 Legal Framework Indira Unninayar, Advocate International Commitments • Universal Declaration of Human Rights, 1948 – Right to inherent dignity, human rights – Right to health and medical care (Art 25) • International Covenant on Economic Social & Cultural Rights (ICESR), 1976 – Enjoyment of the highest attainable standard of physical and mental health (Art 12) – The creation of conditions which would assure to all medical service and medical attention in the event of sickness. Legal Framework Indira Unninayar, 21/03/14 Advocate International Commitments • Alma Ata Declaration, 1978 – The need for urgent action by all governments, all health and development workers, and the world community to protect and promote the health of all the people of the world • Strong reaffirmation that health, which is a state of complete physical, mental and social wellbeing, and not merely the absence of disease or infirmity, is a fundamental human right and that the attainment of the highest possible level of health is a most important world-wide social goal whose realization requires the action of many • VI - Primary health care is essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and country can afford to maintain at every stage of their development in the spirit of self reliance and self-determination. It forms an integral part both of the country's health system, of which it is the central function and main focus, and of the overall social and economic development of the community. It is the first level of contact of individuals, the family and community with the national health system bringing health care as close as possible to where people live and work, and constitutes the first element of a continuing health care process. 21/03/14 Legal Framework Indira Unninayar, Advocate International Commitments • • • • • • • Alma Ata Declaration, 1978 - VII Primary health care: 1. reflects and evolves from the economic conditions and sociocultural and political characteristics of the country and its communities and is based on the application of the relevant results of social, biomedical and health services research and public health experience; 2. addresses the main health problems in the community, providing promotive, preventive, curative and rehabilitative services accordingly; … 5. requires and promotes maximum community and individual self-reliance and participation in the planning, organization, operation and control of primary health care, making fullest use of local, national and other available resources; and to this end develops through appropriate education the ability of communities to participate; 6. should be sustained by integrated, functional and mutually supportive referral systems, leading to the progressive improvement of comprehensive health care for all, and giving priority to those most in need; 7. relies, at local and referral levels, on health workers, including physicians, nurses, midwives, auxiliaries and community workers as applicable, as well as traditional practitioners as needed, suitably trained socially and technically to work as a health team and to respond to the expressed health needs of the community. VIII All governments should formulate national policies, strategies and plans of action to launch and sustain primary health care as part of a comprehensive national health system and in coordination with other sectors. To this end, it will be necessary to exercise political will, to mobilize the country's resources and to use available external resources rationally. 21/03/14 Legal Framework Indira Unninayar, Advocate International Commitments WHO/World Health Organization • • • • • • • • • • • • The ultimate goal of primary health care is better health for all. WHO has identified five key elements to achieving that goal: reducing exclusion and social disparities in health (universal coverage reforms); organizing health services around people's needs and expectations (service delivery reforms); integrating health into all sectors (public policy reforms); pursing collaborative models of policy dialogue (leadership reforms); and increasing stakeholder participation. Key facts The WHO Constitution enshrines the highest attainable standard of health as a fundamental right of every human being. The right to health includes access to timely, acceptable, and affordable health care of appropriate quality. Yet, a vast number suffer financial catastrophe annually, lakhs are pushed below the poverty line as a result of health care expenditure. The right to health means that States must generate conditions in which everyone can be as healthy as possible. It does not mean the right to be healthy. Vulnerable and marginalized groups in societies tend to bear an undue proportion of health problems. 21/03/14 Legal Framework Indira Unninayar, Advocate MDG 2000 • Reduce child mortality • Improve maternal health • Combat HIV/Aids, Malaria and other diseases • INDIA LAGS; BANGLADESH STORY – A REALITY CHECK 21/03/14 Legal Framework Indira Unninayar, Advocate NRHM 2005 • • • • • • Improve availability and access to quality health care by people, especially for those residing in rural areas, the poor, women and children ASHA (Accredited Social Health Activist) – with induction training of 23 days, spread over 12 months, and on the job training throughout the year, accountable to the village panchayat Efforts to improve skills of RMPs (Registered Medical Practitioners) Experiments and innovation to improve the position in Rural areas, given the current problems of availability of Healthcare providers "an ASHA in every village" in India, a target that translates into 250,000 ASHAs in 10 states. The grand total number of Ashas in India was reported in January 2013 to be 863,506 21/03/14 Legal Framework Indira Unninayar, Advocate Important case law • Right to health, right to life •Obligation of State to provide healthcare, medical services without plea of resource constraint 21/03/14 Legal Framework Indira Unninayar, Advocate Important case law • Right to health, right to life • Obligation of State to provide health without plea of resource constraint • Paschim Banga Khet Mazdoor Samity vs State of WB : (1996) 4 SCC 37: • Right to medical services under Art 21 • Every citizen looks to the State to perform its obligations with top priority •CERC vs UOI & Ors: (1995) 3 SCC 42: • In a developing society like ours steeped with unbridgeable and ever widening gaps of inequality in status and of opportunity, law, what is due cannot be ascertained by absolute standard which keeps changing depending on the time, place and circumstances. • Elastic, justice to all sections of society •State of Punjab vs Ram Lubhaya Bagga: (1998) 4 SCC 117 • The Right of the State to manage its policy from time to time, under changing circumstances, cannot be challenged. • The arbitrariness or violation of constitutional mandates can be challenged • Every individual right has to give way to the right of the public at large • Directive Principles have been read into the fundamental rights – to life, to live with dignity 21/03/14 Legal Framework Indira Unninayar, Advocate Important case law (2) • Khatri vs. State of Bihar: (1981) 1 SCC 627 • State cannot deny constitutional rights based on resource constraint. A time bound plan is necessary. • It is the joint obligation of the Centre and States to provide medical services, it is expected that the UOI would render the necessary assistance in improvement of medical services across the country 21/03/14 Legal Framework Indira Unninayar, Advocate Watch out for/Challenge Bad Laws •MCI vs State of Rajasthan: 1996 AIR 2073: 1996 Scale (1) 634 • Wrongly says that unless a person has qualified himself in medicine, he is not eligible to be registered as medical practitioner •Deliberate mischievous, misinterpretation of laws by the MCI, IMA, or Govt – vested interests 21/03/14 Legal Framework Indira Unninayar, Advocate Blocks • • • • MCI, IMA – turf war Ostensible reason – concern for quality But in reality, to protect turf interests Expose them – the referral system, the covert nexus, the real reason violative of right to health • Inheritance of a colonial system, designed to undermine indigenous systems and practices and perpetuate control centres Generates power centres through a false notion of what is ‘lawful’ Criminalizes those who do not tow the line But turns a blind eye to the reality of ‘lawlessness’ Similar state of illegality, vagueness, uncertainty, deliberate openings for extortion: Laws abused, not used • • • • • • • • • • • 21/03/14 NMVs Hawkers, street vendors Municipal cleaning, rag pickers Freedom of speech – book, film bans Judiciary – huge challenge Informal Providers – huge challenge Legal Framework Indira Unninayar, Advocate Important SC judgments (3) • Dr Mukhtiar Chand vs State of Punjab: (1998) 7 SCC: • If State law recognizes a qualification then the person is entitled to be medical practitioner • S 33 of the Drugs & Cosmetics Act confers wide powers on the Central Government to make rules • Rule 2(ee) of the Drugs & Cosmetics Rules allows the State to declare by a general or special order made by the State Government as a person practising the modern scientific system of medicine • To fulfill S 15(2) of the IMC Act, she/he should also be registered in a Medical Register of the State. No person other than a medical practitioner enrolled on a State Medical Register, (b) shall practise medicine in any State • Upheld in Subhasis Bakshi & Ors vs W.B. Medical Council & Ors (2003) 9 SCC 269 21/03/14 Legal Framework Indira Unninayar, Advocate Strategies • Use Drugs & Cosmetics Act & Rules • Make representations to Central Govt u/S 10 A for establishment of new medical college, new course of study • New University under Medical Degrees Act, 1916 • New laws including ordinances, delegated legislation • New laws for Healthcare professionals • Challenge some of the existing court rulings • Make representation seeking the realization of Right to Health and access to Healthcare • Invoke international conventions too • THROUGH REPEATED, PERSISTENT REPRESENTATIONS, CHALLENGES • THROUGH NGOS TOO 21/03/14 Legal Framework Indira Unninayar, Advocate