Suprachoroidal Hemorrhage
advertisement

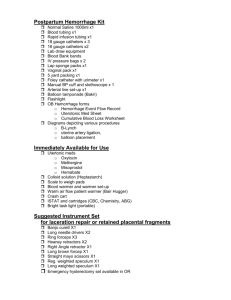
Grand Rounds Alejandro Leon, MD PGY-4 Vanderbilt Eye Institute August 24, 2007 Clinical presentation Painful loss of vision left eye. 58 year old male. Blunt trauma to left eye 3 days ago. Mild discomfort and blurred vision. No flashes, no floaters. Morning day of presentation: Intense pain in left eye. “My vision is now black”. Previous history PMH: Chronic sinusitis, s/p lumbar spinal fusion, HTN, hyperlipidemia. FHx: No glaucoma. SH: self employed truck driver. Denies smoking and alcohol use. Allergies: NKDA. Medications: BP medication, cholesterol pill, Travatan qHS OS. Physical exam VA cc: OD: 20/40OS: LP temporally. Motility: Full OU. CVF: Full OD, OS unable. IOP: OD: 9 OS: 3. External: unremarkable. Pupils: +rAPD OS. SLE: OD: 2+ NSC. Differential diagnosis Choroidal effusion. Suprachoroidal hemorrhage. Rhegmatogenous retinal detachment. Melanoma or metastatic tumor of choroid or ciliary body. Other exam findings. DFE: OD: WNL with 0.4 c/d OS: No view. Anything else you want to test? B-scan Diagnosis Traumatic dehiscence of clear corneal wound. Appositional suprachoroidal hemorrhage. Suprachoroidal Hemorrhage Suprachoroidal hemorrhage (SCH) Defined as Accumulation of blood between the choroid and the sclera. Suprachoroidal space is an almost virtual space. (10 microliters) One of the most dreaded complications. Could result in total loss of vision and phthisis. Suprachoroidal hemorrhage (SCH) Limited suprachoroidal hemorrhage. Massive suprachoroidal hemorrhage. Appositional (“kissing”). Expulsive. Pathophysiology Fragile vessels is exposed to Sudden compression and decompression events. Fluctuation in intraocular fluid dynamics and pressure. Hypotony may lead to suprachoroidal effusion and cause tension on the vessels. Pathophysiology Intact posterior capsule may tamponade against such intense intraocular decompression during surgery. Ocular manifestations Decreased vision. Pain. Shallow anterior chamber with mild cells and flare. Smooth, bullous, orange-brown elevation of the retina and choroid. Fundus findings Anterior to the equator Extends in an annular fashion Postequatorial unilobulated or multilobulated. Fundus findings Anterior to the equator Extends in an annular fashion Postequatorial unilobulated or multilobulated. Echography B-scan smooth, thick, dome-shaped membrane Little, if any, after movement on kinetic evaluation. Fresh blood clots. high-reflective, solid-appearing mass, with irregular internal structure and irregular shape. Serial ultrasonography for liquefaction of hemorrhage. low-reflective mobile opacities replacing clot. Treatment Delayed nonexpulsive limited choroidal hemorrhage Conservative. Generally good prognosis. Usually resolves spontaneously within 1–2 months. Use of cycloplegics and topical corticosteroids. Treatment Delayed, nonexpulsive massive choroidal hemorrhage Systemic corticosteroids (controversial). Posterior sclerotomy to release suprachoroidal blood. Treatment Intraoperative massive choroidal hemorrhage Tamponade. Rapid wound closure to prevent: Expulsion or loss of the intraocular contents. Incarceration of vitreous or retina in the surgical wound. Treatment Secondary Management Relieve vitreous or retinal incarceration. (to decrease risk of RD). Drainage of choroidal hemorrhage ideally is conducted after liquefaction of the suprachoroidal hemorrhage (serial echography). Drainage of choroidal hemorrhage Choroidal hemorrhage in trauma Intraocular structural damage. High likelihood of retinal detachment and associated proliferative vitreoretinopathy. B-scan choroidal hemorrhage tend to be more diffuse and less elevated. Wound Dehiscence in Pseudophakia Cataract wound dehiscence post trauma. 11 patients None small incision (no phacoemulsification) Falling was the most frequent. 3 days to 1 year after surgery. 10/11 not wearing protective eyewear. 6/11 had 20/40 or better vision. 5/11 had 20/200 to LP vision. Johns KJ, et.al., Am J Ophthalmol. 1989. 108:535-39 Small incision trauma dehiscence Age (years) Surgery to trauma Event Wound Associated injury 72 3 years Fell Clear cornea Iris prolapse 92 3.5 years Fell Scleral tunnel Extrusion of IOL. 68 4 months Fell Clear cornea Expulsive iridodialysis 91 5 years 8 months Fell Clear cornea Expulsion IOL and iris 84 10 weeks Fell Clear cornea Expulsive iridodialysis SCH with wound dehiscence Report 3 previously aphakic eyes. Traumatic dehiscence wound. Massive SCH, uveal prolapse and retinal detachment. Initial visual acuity was LP in all patients. Drained when decrease of SCH seen in B-scan (average 14 days). SCH drainage with PPV and silicone oil. Final visual acuities varied from 20/70 to 1/200. Good anatomical result. Liggett PE, et al. Retina. 1990; 10 Suppl 1:S59-64. Back to our patient Surgical wound closure. Oral prednisone. Atropine, Vigamox, and PF. Followed every week with B-scan. 2 weeks after event choroids without apposition but no signs of liquefaction. 3 1/2 weeks later drained surgically. Back to our patient Best visual acuity after procedure: 2/200 “E” Required tube shunt placement for IOP control. Take home points Cataract wounds can dehisce even years after surgery with trauma. Management of suprachoroidal hemorrhage include: Recognize. Tamponade and closure of eye. Consider systemic steroids. Drain when signs of liquefaction in B-scan. References. Hurvitz LM. Late clear corneal wound failure after trivial trauma. J Cataract Refract Surg 1999; 25:283-284. Routsis P. Late traumatic wound dehiscence after phacoemulsification. J Cataract Refract Surg 2000; 26:1092-1093. Navon SE, Expulsive iridodialysis: an isolated injury after phacoemulsification. J Cataract Refract Surg 1997; 23:805-807. Blomquist PH, Expulsion of an intraocular lens through a clear corneal wound. J Cataract Refract Surg 2003; 29:592-594. Walker NJ, Foster A, Apel AJG. Traumatic expulsive iridodialysis after small-incision sutureless cataract surgery. J Cataract Refract Surg 2004; 30:2223-2224. Liggett PE, Mani N, Green RE, Cano M, Ryan SJ, et al. Management of traumatic rupture of the globe in aphakic patients. Retina. 1990; 10 Suppl 1:S59-64. Kuhn F, Morris R, Mester V. Choroidal detachment and expulsive choroidal hemorrhage. Ophthalmol Clin North Am. 2001 Dec;14(4):639-50. Scott IU, Flynn HW, Schiffman J, Smiddy WE, Ehlies F. Visual acuity outcomes among patients with appositional suprachoroidal hemorrhage. Ophthalmology 1997; 104:2029-2046. Meier P, Wiedemann, P. Massive suprachoroidal hemorrhage: secondary treatment and outcome. Graefe’s Arch Clin Exp Ophthalmol 2000. 238:28-32. Kapusta MA, Lopez PF. Choroidal hemorrhage. Yanoff: Ophthalmology. 2nd Edition. Chapter 138. 2004 Mosby Inc. Johns KJ, Sheils P, Parrish CM, Elliott JH, O’Day DM. Traumatic wound dehiscence in pseudophakia. Am J Ophthalmol 1989. 108:535-539.