3M Health Information Systems, Inc.
Assessing the Financial Impact of MS-DRGs
Healthcare Financial Management Association-Utah Chapter
September 20, 2007
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Major Changes Proposed in the Final Rule
DRG Reclassification and Relative Weight Recalibration
Medicare Severity DRGs (MS-DRGs)
Hospital-acquired Conditions (per the Deficit Reduction Act)
Relative Weight Modifications
Behavioral Offset
Update to Long Term Care DRGs
Updates to payment related changes including:
Wage Index
Operating and GME costs
Capital related costs
Rates for excluded hospitals
© 2007 3MHealthOperating
Information Systems, Inc.
All Rights
Reserved.
and
Capital
Rates
2
3M Health Information Systems, Inc.
October 1, 2007
MS-DRGs will be used for
IPPS
New DRGs
New reimbursement
3
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
POA and other regulatory
changes
3M Health Information Systems, Inc.
How does a grouper work?
It is similar to a known recipe:
+
Identification of
diagnoses and
procedures
+
Coding the
diagnoses and
procedures
4
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
=
Grouping the
diagnoses and
procedures
DRG
3M Health Information Systems, Inc.
What’s driving severity documentation and coding today?
Severity based reimbursement: changes in hospital
payment by Medicare, Medicaid, and private payers
Provider profiling and performance transparency:
Patients are “sicker” and we need to demonstrate how this
impacts our ability to deliver quality care
Hospital report cards: Consumers want to compare
providers (and have more methods to do so today)
Aging population and increasing life expectancy: the
need to conserve limited resources for increasing demand
Quality focused care: providers need ways to measure and
improve their performance
5
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
6
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Key Regulatory Changes:
CMS adopts MS-DRGs:
Regulation:
Provider
Implications
Creates Major CC subclasses
Increases number of DRGs
from 538 to 745
Completely revised CC list
Must learn new DRG
system
Must learn new CC and
MCC lists
Must be ready by October 1
7
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
What are MS-DRGs?
Update to 1994 Severity DRGs
3 Step Process:
Consolidate current DRGs into base DRGs
Categorize each diagnosis as:
• Major CC (MCC)
• CC
• Non-CC
Subdivide each base DRG into subgroups based on CCs
• No Subgroups
• 3 groups (MCC, CC, non-CC)
• 2 groups (MCC/CC, non-CC)
• reserved.
2Systems,
groups
(MCC, CC/non-CC)
© 3M3M
2007.
All rights
© 2007
Health
Information
Inc. All Rights Reserved.
8
3M Health Information Systems, Inc.
Consolidation of DRGs:
115 pairs of DRGs that were subdivided based on presence of a
CC
Major cardiovascular conditions
3 pairs of burn DRGs
43 pediatric DRGs that were defined by age <=17
Several DRGs relating primarily to pediatric or adult population that
have very low volume in the Medicare population
Several elective surgery DRGs that have shifted to outpatient
settings
Some clinically related DRGs that had volume, but no difference in
resource use
MDC 14 & 15 were not consolidated due to low volume
9
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
MS DRGs Increases the Number of DRGs from 538 to
745
Subgroups
Number of Proposed
Base MS-DRGs
Number of
Proposed
MS-DRGs
No Subgroups
53
53
Three subgroups
152
456
Two subgroups: major CC and CC; non-CC
43
86
Two subgroups: non-CC and CC; major CC
63
126
Subtotal
311
721
MDC 14, 15
22
22
Error DRGs
2
2
335
745
Total
10
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
MS vs. current CMS DRG Groups:
Base Group, no splits
CMS V24 CMS DRG Descriptions
524
Transient ischemia
MS v25
069
MS-DRG Descriptions
Transient ischemia
MS vs. current CMS DRG Groups:
3 Groups - MCC, CC, non-CC
CMS V24 CMS DRG Descriptions
027
Traumatic Stupor & Coma,
coma > 1 hr
MS v25
082
083
084
11
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
MS-DRG Descriptions
Traumatic stupor & coma, coma >1
hr w MCC
Traumatic stupor & coma, coma >1
hr w CC
Traumatic stupor & coma, coma >1
hr w/o CC/MCC
3M Health Information Systems, Inc.
MS vs. current CMS DRG Groups:
2 Groups – with MCC, without MCC
CMS V24 CMS DRG Descriptions
103
Heart transplant or implant of
heart assist system
MS v25
001
002
MS-DRG Descriptions
Heart transplant or implant of heart
assist system w MCC
Heart transplant or implant of heart
assist system w/o MCC
MS vs. current CMS DRG Groups:
2 Groups – with CC/MCC, without CC/MCC
CMS V24 CMS DRG Descriptions
021
Viral meningitis
12
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
MS v25
075
076
MS-DRG Descriptions
Viral meningitis w CC/MCC
Viral meningitis w/o CC/MCC
3M Health Information Systems, Inc.
MS vs. current CMS DRG Groups:
Exception to rules:
CMS V24 CMS DRG Descriptions
480
Liver and/or Intestinal
Transplant
MS v25
005
006
13
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
MS-DRG Descriptions
Liver transplant w MCC or intestinal
transplant
Liver transplant w/o MCC
3M Health Information Systems, Inc.
Key Regulatory Changes:
Behavioral offset:
Regulation:
Provider
Implications
CMS anticipates improved
documentation and coding
Payments reduced 1.2% to
account for this
Blending of relative weights
MS-DRGs and CMS DRGs
Unless documentation and
coding is improved a
significant loss of payment will
occur impacting operating
margins
14
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Behavioral Offset
Proposed Rule was 2.4% in FY2008 and FY2009
Final Rule is 1.2% in FY2008 and 1.8% in FY2009
and FY2010
This compromise to the proposed rule includes a 2
year phase in of the impact of MS-DRGs by blending
the relative weights 50% base on CMS DRGs and
50% based on MS-DRGs
15
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Key Regulatory Changes:
MS-DRGs are designed for
payment of Medicare
patients:
Regulation:
Provider
Implications
Not applicable to other payers
Not applicable for quality
Other payers will likely adopt
other groupers
Hospitals need to maintain
multiple groupers
16
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
IPPS Applicability
“The focus of CMS’ efforts is in developing and
maintaining a DRG system that is appropriate for its
Medicare population.”
“We do not believe that Medicare should undertake
the effort and expense to maintain and update a
DRG system that will have no application for
Medicare beneficiaries.”
17
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Key Regulatory Changes:
Payment weight
methodology modified:
Regulation:
Provider
Implications
Second year of three year
transition to cost based
weights
Impact on aggregate payments
will vary by hospital
Relative profitability across
service line will change
18
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Relative Weights
CMS will continue to implement the cost-based DRG relative
weights under the 3-year transition period that began in FY2007
This year the relative weights will be recalibrated using a blend of
67 percent of the cost relative weight and 33 percent of the charge
relative weight
By FY 2009, the relative weights will be 100 percent cost-based
The 50/50% blend of MS-DRGs and CMS DRGs in calculating the
relative weight is on top of the transition to cost based weights
19
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Key Regulatory Changes:
Present on Admission
Indicator (POA):
Regulation:
Provider
Implications
New POA data element must
be submitted to Medicare
Must begin coding POA
Coder productivity will be
impacted
20
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Deficit Reduction Act Requirements
Deficit Reduction Act (DRA)—(Pub. L. 109-171)
Requires that the Present on Admission (POA) indicator be
collected for all Medicare patients— beginning Oct 1, 2007
Requires CMS to select two or more conditions that are high
cost/high volume.
Requires CMS to begin excluding those conditions from the
calculation of the DRG when they are identified as not present
on admission—beginning Oct 1, 2008.
21
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Implementation Date for POA Data Collection
Deficit Reduction Act of 2005 (DRA) requires the POA
indicator to be collected starting Oct. 1, 2007
Change Request #5499 instructs hospitals how to
submit this data
Current Form ASC X12N 837, v4010 does not have POA field
Segment K3 in the 2300 loop, data element K301 should be
used
Instructions on how to code the POA indicator are in the ICD9-CM Official Guidelines for Coding and Reporting
22
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Key Regulatory Changes:
8 Post admission
complications excluded
from DRG assignment:
Regulation:
Provider
Implications
Post admission
complications excluded
from DRG assignment
Model potential financial
impact and initiate
continual improvement
measures
Evaluate post admission
complication rates in your
facility
23
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M
Health Information Systems,
Inc.
Hospital-Acquired
Conditions
not POA will not be included in MS DRG
assignment beginning October 2008
Condition
Considered in
NPRM
Proposed in
NPRM
Selected in FY
2008 Final Rule
May Be
Considered in
Future
Rulemaking
1. Serious Preventable
Event- Object left in surgery
Yes
Yes
Yes
N/A
2. Serious Preventable
Event- Air embolism
Yes
Yes
Yes
N/A
3. Serious Preventable
Event- Blood
incompatibility
Yes
Yes
Yes
N/A
4. Catheter Associated
Urinary Tract Infections
Yes
Yes
Yes
N/A
Yes
Yes
Yes
N/A
No (No FY 2008
code)
Yes (Code
Created for FY
2008)
N/A
N/A
No (No unique
codes)
Yes (Comments
suggested
Mediastinitis
which has unique
code)
5. Pressure Ulcers
(Decubitus Ulcers)
6. Vascular Catheter
Associated Infection
7. Surgical Site InfectionMediastinitis after Coronary
Artery Bypass Graft
(CABG) surgery
8. Falls
Yes
Yes (All surgical
site infections, not
just Mediastinitis)
Yes
24
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
No (Coding not
unique)
Yes (Operational
difficulties will
be overcome by
FY 2009)
Expand to all
hospital acquired
injuries, adverse
events
3M Health Information Systems, Inc.
Summary
Regulation
Provider Implications
CMS adopts MS-DRGs on October 1,2007
Learn new DRG system, new CC and MCC lists
Ensure software solutions are MS DRG ready
Educate cross functional team on MS DRGs
1.2% Behavioral Offset in anticipation of coding and
documentation improvement
Educate HIM department about MS DRG coding implications
MS-DRGs are designed for payment of Medicare patients:
Other payers will likely adopt other groupers
Ensure most accurate documentation and coding processes in place
Hospitals need to maintain multiple groupers
Continued transition from charge to cost based relative weights
Analyze gap and impact analysis
Ensure software systems are ready for reimbursement calculations
Submit Present on Admission (POA) data to Medicare
Ensure software tools are ready for POA collection
Educate HIM department on POA coding guidelines
Consider operational improvements for coder workflow
8 Post Admission complications identified for exclusion from
DRG assignment (October 1, 2008)
Model potential financial impact, gap and initiate continual
improvement measures.
Evaluate post admission complication rates in your facility.
25
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Financial Changes in the next three years
26
2008
2009
2010
Behavioral
offset
1.2%
1.8%
1.8%
Cost vs
charge
67/33
100%
100%
Complication 0% impact
not calculated
in DRG
If not POA,
If not POA,
not calculated not calculated
CMS/MS
DRG weight
blend
50/50
50/50
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
Full MS DRG
3M Health Information Systems, Inc.
Complications/Comorbidities
Major CCs (MCC) were designated if:
they were a CC for CMS,
they were a Major CC in AP-DRGs
they were an APR DRG severity 3 (major) or severity 4
(extensive)
Non-CC:
non-CC diagnosis in CMS and in AP-DRGs
APR DRG default severity level 1 (minor)
CC:
any diagnosis that did not meet either of the above two criteria
27
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Summary of 3M™ APR DRGs
MDC/APR MDC
316 APR DRGs
Subdivide each APR DRG
into subclasses
Four Severity of Illness Subclasses
Four Risk of Mortality Subclasses
1.
Minor
1.
Minor
2.
Moderate
2.
Moderate
3.
Major
3.
Major
4.
Extreme
4.
Extreme
1,258 Subclass Cells
28
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
1,258 Subclass Cells
3M Health Information Systems, Inc.
Examples of 3M™ APR DRG Subclasses
1
2
3
4
Severity of Illness
Minor
Moderate
Major
Extreme
1
2
3
4
Risk of Mortality
Minor
Moderate
Major
Extreme
Secondary Diagnosis-Diabetes Mellitus
Uncomplicated Diabetes
Diabetes w Renal Manifestation
Diabetes w Ketoacidosis
Diabetes w Hyperosmolar Coma
Secondary Diagnosis-Cardiac Dysrhythmias
Premature Beats
Sinoatrial Node Dysfunction
Paroxysmal Ventricular Tachycardia
Ventricular Fibrillation
29
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Complications/Comorbidities
Reduced CC list from 3,326 to 2,583 diagnoses codes in 2006;
now there are 4,922 codes that are either a Major CC or a CC:
Major CC
CC
1,580 codes
3,342 codes
Patients under V 24 had at least one CC 77.6% of the time, under
the proposed MS-DRG system, this will be reduced to 40.34%.
Chronic diseases were removed from the CC list unless there was
a significant acute manifestation:
30
Mitral valve disorders
CHF
Stage I-II chronic renal failure
Chronic UTI
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
MS-DRG Categories
MS-DRGs with no qualifiers
Chest Pain
Chest Pain
CMS DRG 143
RW .5637
$2,749
31
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
Chest Pain
MS-DRG 313
RW .5550
$2,707
3M Health Information Systems, Inc.
MS-DRG Categories
MS-DRGs with 3 potential groups (MCC-CC-NCC)
MS-DRG 291
Heart Failure w MCC
RW 1.4760
$ 7,200
Congestive Heart Failure
(No qualifiers required)
CMS DRG 127
RW 1.0490
$5,117
MS-DRG 292
Heart Failure w CC
RW 1.0169
$4,960
MS-DRG 293
Heart Failure w/o MCC or CC
RW .7265
$3,544
32
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
MS-DRG Categories
MS-DRGs with MCC or w/o MCC
CABG with Cath w Major CV
CMS DRG 547
RW 6.1390
$29,946
CABG with Cath w MCC
MS-DRG 233
RW 7.1350
$34,805
CABG with Cath w/o Major CV
CMS DRG 548
RW 4.6440
$22,653
CABG with Cath w/o MCC
MS-DRG 234
RW 4.6211
$22,542
33
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
MS-DRG Categories
MS-DRGs with CC/MCC or w/o CC/MCC
Major Joint/Limb
Reattachment UE
CMS DRG 491
RW 1.7203
$8,392
Major Joint/Limb Reattachment UE w CC/MCC
MS-DRG 483
RW 2.1931
$10,698
Major Joint/Limb Reattachment UE w/o CC/MCC
MS-DRG 484
RW 1.6862
$8,225
34
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
MS-DRGs Demand Increased Coding Precision
“In determining the CC subclass assigned to a diagnosis, imprecise
codes were, in general, not assigned to the MCC or CC subclass.”
428.21
Acute Systolic Heart Failure
Major CC
428.41
Acute Systolic & Diastolic Heart Failure
Major CC
428.43
Acute On Chronic Systolic Heart Fail
Major CC
428.31
Acute Diastolic Heart Failure
Major CC
428.33
Acute On Chronic Diastolic Heart Failure
Major CC
428.1
Left Heart Failure
CC
428.20
Systolic Heart Failure NOS
CC
428.22
Chronic Systolic Heart Failure
CC
428.32
Chronic Diastolic Heart Failure
CC
428.40
Systolic & Diastolic Heart Failure
CC
428.0
Congestive Heart Failure NOS
Non CC
428.9
Heart Failure NOS
Non CC
35
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Why is documentation and coding improvement so critical?
Example: In MS DRGs the precise type of heart failure dramatically impacts payment
With CC
Without CC or
MCC
Payment
Payment
Weight
$14,732
(1.8415)
With MCC
$23,148
$36,047
(2.8935)
(4.5059)
Major Small & Large Bowel Procedures
MS-DRG 331
36
MS-DRG 330
MS-DRG 329
428.
0
Congestive Heart Failure Not
Otherwise Specified
428.1
Left Heart Failure
428.21
Acute Systolic Heart Failure
428.20
Systolic Heart Failure NOS
428.23
Acute on Chronic Systolic Heart Failure
428.
9
Heart Failure Not Otherwise
Specified
428.22
Chronic Systolic Heart Failure
428.31
Acute Diastolic Heart Failure
428.30
Unspecified Diastolic Heart Failure
428.33
428.32
Chronic Diastolic Heart Failure
Acute on Chronic Diastolic Heart
Failure
428.40
Systolic & Diastolic Heart Failure
428.41
Acute Systolic & Diastolic Heart Failure
428.42
Chronic combined Systolic and
Diastolic Heart Failure
428.43
Acute on Chronic Systolic Heart Failure
In prior versions of the CMS DRGs all heart failure codes were a CC so distinctions related to the type of heart failure did not
impact DRG assignment
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
Some conditions that are no longer CCs
CHF
Chronic blood loss
anemia
Chronic Renal
Failure Stage I-III
Seizure Disorder
Dehydration
Angina (stable)
COPD
Atrial Fibrillation
Hyperkalemia
37
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
3M Health Information Systems, Inc.
UTI vs. Septicemia Example
CMS DRG 320
PDx: Urosepsis
SDx: Dehydration
COPD
DRG
With CC
RW .8769
$4,278
MS-DRG 688
PDx: Urosepsis
SDx: Dehydration
COPD
No longer
CCs
RW .7018
$3,423
APR DRG 463
No change
SOI Subclass 2
RW .5973
ROM Subclass 2
Peer Mortality: .8%
38
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
MS-DRG 871
PDx: Septicemia
SDx: Dehydration
COPD
UTI
Malnutrition
Major CC,
but only if
site
specified
Decubitus Hip
Shock
RW 1.8632
$9,089
APR DRG 720
SOI Subclass 4
RW 3.3739
ROM Subclass 4
Peer Mortality: 42.4%
In current
CMS system,
Septicemia
was
reimbursed at
$7,803
3M Health Information Systems, Inc.
The Challenge
Physician
Documentation
is recorded in
CLINICAL terms
Breakdown
between the two
languages
39
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
Documentation for
coding, profiling &
compliance must
contain specific
DIAGNOSTIC terms
3M Health Information Systems, Inc.
Common Documentation Issues
Unable to Code
Acceptable to Code
LUL Infiltrate
LUL Pneumonia
Hgb 5.2; Transfused
Acute or Chronic Blood Loss Anemia
Emaciated; Total Protein/Albumin Low; Nutrition
Malnutrition
Supplements Started
ABG 7.22/68/44; Will Treat Accordingly
Respiratory Failure, Acidosis, Alkalosis, Etc.
Will Rehydrate Patient
Dehydration
BP 70/40 on Dopamine for Support
Shock
Cardiac Enzymes Elevated; EKG Positive
Acute MI
No Overt CHF; Will Continue Lasix and Lanoxin Compensated CHF
Unable to Void; Cathed for 600 cc
Urinary Retention
Sputum Gram Stain with Large Amount GramNegative Rods; Will Cover with Rocephin
Questionable Gram-Negative Pneumonia
40
© 3M3M
2007.
All rights
reserved.
© 2007
Health
Information
Systems, Inc. All Rights Reserved.
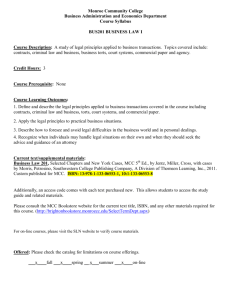
3M Health Information Systems, Inc.
Gender: Female
Disposition: Died
Age: 55
LOS: 11 Days
Principal Diagnosis: 431
Secondary
Diagnoses
Intracerebral hemorrhage
Case 1
Case2
LOS
Case 3
Case 4
Description
78729
42731
78729
42731
2867
78729
42731
2867
5070
78729
42731
2867
5070
Other dysphagia
Atrial fibrillation
Acquired coagulation factor def
Pneumonitis due to inhalation
of food or vomitus (MCC)
Coma
78001
MS-DRG
66 w/o CC/MCC
Reimbursement $5,025
41
65 w/CC
64 w/MCC
64 w/MCC
$5,805
$7,546
$7,546
APR SOI
2
2
3
4
APR ROM
2
2
3
4
39%
76%
Expected
14%
14%
Mortality
Rate
© 2007 3M Health Information Systems, Inc. All Rights Reserved.
Intracranial hemorrhage or
cerebral infarction
3M Health Information Systems, Inc.
Questions
42
© 2007 3M Health Information Systems, Inc. All Rights Reserved.