A discussion of SIDS, bed-sharing, counting sheep, and baby sleep
advertisement

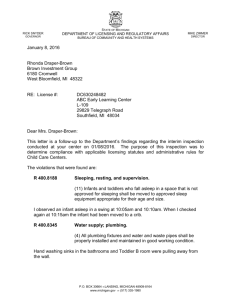
Counting sheep: Breastfeeding Infants and Sleep Safety Elizabeth A Fleming, MD Dean Clinic East Family Medicine Disclosures and Gratitude: I have no relevant personal financial relationships or any commercial interests. The content of this presentation was prepared by me and does not reflect the views and opinions of Dean, St. Mary’s Hospital or SSM. Thank you to Ildi Martonffy and Laura Berger for your guidance in preparing for this talk, to Daniel Stattelman-Scanlan who generously allowed me to share Dane Co Public Health data, and to those of you who took the time to fill out the survey. Objectives Define Sudden Infant Death syndrome and Sudden Unexplained Infant Death and review current recommendations. Discuss benefits of breastfeeding as they relate to risk of SUID/SIDS. Review existing evidence around co-sleeping, roomsharing, and bed-sharing. Discuss current symposium attendee practices regarding infant sleep and counseling. People are talking about this… Sudden unexplained infant death the death of a previously healthy infant, less than 365 old, that occurs suddenly and unexpectedly, and the cause of death is not immediately obvious prior to investigation. SUID can be attributed to: Suffocation Asphyxia Entrapment Infection Ingestions Metabolic disease Arrhythmia Trauma (accidental or non-accidental) Defining SIDS AAP Policy Statement 2011: “Sudden infant death syndrome (SIDS) is a cause assigned to infant deaths that cannot be explained after a thorough case investigation, including a scene investigation, autopsy, and review of the clinical history.” This is different than sudden unexplained infant death (SUID). Co-sleeping When an infant sleeps in close proximity with one or both parents. Room sharing: when an infant sleeps in the same bedroom as one or both parents Bed sharing: when an infant sleeps in the same bed as one or both parents SUID statistics According to the CDC, about 3,500 infants die suddenly of no immediately, obvious cause in the US every year. In 2013, about 1,500 deaths reported as SIDS 21 cases of SUID in Dane County from 2011 - 2014 Current AAP Guidelines Breastfeeding is recommended 2011 Meta-analysis of 18 case-control studies (n=2,810) Breastfeeding was protective against SIDS for all groups Any amount of breast milk for any duration (multivariable SOR 0.55 95% CI 0.44-0.69) Exclusive breastfeeding for any duration showed a greater reduction (univariable OR 0.27, 95% CI: 0.240.31) Sleep position The Supine Sleep Position Is Recommended for Infants to Reduce the Risk of SIDS; Side Sleeping Is Not Safe and Is Not Advised Once an Infant Can Roll From the Supine to Prone and From the Prone to Supine Position, the Infant Can Be Allowed to Remain in the Sleep Position That He or She Assumes Bedding Pillows, Quilts, Comforters, Sheepskins, and Other Soft Surfaces Are Hazardous When Placed Under the Infant or Loose in the Sleep Environment Wedges and Positioning Devices Are not Recommended Bumper Pads and Similar Products Are not Recommended Prenatal and Postnatal Exposures Pregnant Women Should Seek and Obtain Regular Prenatal Care Smoking During Pregnancy, in the Pregnant Woman's Environment, and in the Infant's Environment Should Be Avoided Avoid Alcohol and Illicit Drug Use During Pregnancy and After the Infant's Birth Other Recommendations Consider Offering a Pacifier at Nap Time And Bedtime Avoid Overheating and Head Covering in Infants Infants Should Be Immunized in Accordance With Recommendations of the AAP and Centers for Disease Control and Prevention Although Swaddling May Be Used as a Strategy to Calm the Infant and Encourage Use of Supine Position, There Is Not Enough Evidence to Recommend It as a Strategy for Reducing the Risk of SIDS Sleep Surfaces Infants Should Sleep in a Safety-Approved Crib, Portable Crib, Play Yard, or Bassinet Car Seats and Other Sitting Devices Are not Recommended for Routine Sleep at Home or in the Hospital, Particularly for Young Infants Co-sleeping Room-Sharing Without Bed-Sharing Is Recommended There Is Insufficient Evidence to Recommend Any BedSharing Situation in the Hospital or at Home as Safe; Devices Promoted to Make Bed-Sharing “Safe” Are Not Recommended (ie cosleepers or sidecars) There Are Specific Circumstances in Which Bed-Sharing Is Particularly Hazardous Infants May Be Brought Into the Bed for Feeding or Comforting but Should Be Returned to Their Own Crib or Bassinet When the Parent Is Ready to Return to Sleep ABM Recommendations Any recommendations for infant care that impede breastfeeding need to be carefully weighed against benefits. Do not assumed that all families are practicing one sleeping arrangement only. Parents need to be encouraged to express their views and seek information. “There is not currently enough evidence to support routine recommendations against co-sleeping. Parents should be educated about risks and benefits of cosleeping and unsafe co-sleeping practices and should be allowed to make their own decisions.” ABM Recommendations Some potentially unsafe practices to bed sharing: Environmental smoke exposure/maternal smoking Sharing sofas, couches, or daybeds Sharing water beds or use of soft bedding Sharing beds with adjacent spaces that could entrap an infant Prone or supine position Alcohol or mind altering drugs Bed sharing with other children Bed sharing with younger babies <8-14 weeks of age may be more strongly associated with SIDS ABM Safe Sleep Recommendations Place babies in the supine position. Room sharing appears to be protective against SIDS. Use a firm, flat surface. Avoid waterbeds, couches, sofas, pillows, soft materials, loose bedding. If blankets, they should be tucked around the mattress so the infant’s head is less likely to be covered. Ensure that the head will not be covered. In a cold room the infant could be kept in an infant sleeper to maintain warmth. Avoid the use of quilts, duvets, comforters, pillows and stuffed animals. ABM Safe Sleep Recommendations Never put an infant down to sleep on a pillow or adjacent to a pillow. Never leave an infant alone on an adult bed. Inform families that adult beds have potential risks and are not designed to meet federal safety standards for infants. Ensure there are no spaces between the mattress which may entrap the infant. Placement of a firm mattress directly on the floor away from walls may be a safe alternative. Another alternative I the use of an infant bed that attaches to the side of the adult bed. (No studies about this) In my professional opinion, bed sharing increases the risk of SIDS. Sorted by: If you have children, did your infant sleep in the same bed as you and your partner (ie. Bed sharing)? In my practice, I counsel parents: Sorted by: If you have children, did your infant sleep in the same bed as you and your partner (ie. Bed sharing)? Substance Use: Multicenter European Study 17 European countries and 20 centers included, data from 1992 to 1996 Case control study published in 2004 745 cases of SIDS and 2411 controls Multivariate analysis revealed increased risk of SUID if: Mother smoked and bed shared (OR 17.7, 95% CI 10.330.3) Maternal smoking, others in household smoking independent of bed sharing (>10 cigarettes per day) Maternal consumed 3+ drinks vs none in the last 24 hours (OR 2.36, 95% CI 1.18-4.71) Other Risk factors: Multicenter European Study History of ALTE (OR 2.76, 95% 1.76-4.32) Prone position (OR 13.1, 95% CI 8.51-20.2) Male gender (OR 1.49 (95% CI 1.11-1.99) Birth weight <3500 g Maternal age <30 Previous livebirths Marital status Employment status (OR 1.85, 95% CI 1.39-2.45) Decreased risk with room sharing usually (OR 0.48, 95% CI 0.34-0.69) and at last sleep (OR 0.32, 95% CI 0.19-0.55) Bed Sharing: Multicenter European Study The increased risk of SIDS if the mother did not smoke but shared a bed was not statistically significant (OR 1.56 95% CI 0.91-2.68) But there was a statistically significant increased risk if the infant was less than 8 weeks old. Chicago Infant Mortality Study Population-based case-controlled study 260 SIDS cases from Chicago, November 1993 - April 1996 Population: 75.0% black, 13.1 hispanic-white, 11.9% nonhispanic white Multivariate analysis revealed independent risk factors for SIDS prone sleeping position (aOR 2.3; 95% CI, 1.3-4.3) maternal smoking during pregnancy (OR 4.3; 95% CI, 2.1–8.9) soft sleep surfaces (OR 5.2; 95% CI, 2.6-10.2) pillow use (OR 2.8; 95% CI, 1.3-6.2). not using a pacifier (OR 2.9, 95% CI, 1.4-6.0) bed sharing in combinations other than the parents alone (OR 3.6; 95% CI, 1.4–9.4) bed sharing by infants with mothers or mother and father did not significantly increase SIDS risk (OR 1.4; 95% CI, 0.7–2.8) Breastfeeding was found to be protective (Adjusted univariate analysis, OR 0.4, CI 0.2-0.7) The German Sudden Infant Death Syndrome Study Population-based case control study from 1998-2001 333 SIDS cases and 998 matched controls Detailed questionnaire filled out with parent, autopsy using standard protocol, multidisciplinary panel to determine SIDS vs SUID. Demonstrated increased risk via multivariate analysis if: Bed sharing (OR 2.73, 95% CI 1.34-5.55) Sleeping at a friend’s or relative’s (OR 4.39, 95% CI 1.11-17.38) Sleeping in the living room (OR 2.41, 95% CI 1.06-5.51) Prone sleeping position (OR 7.08, 95% CI 8.93-50.73) Duvets (OR 2.20, 95% CI 1.21-4.00 thick, OR 1.92, 95% CI 1.07-3.45 light) Decreased risk if: Pacifier use (OR 0.39, OR 0.25-0.59) Scotland Case Control Study 123 infants who died of SIDS and 263 controls between 1996 to 2000 Sharing a sleep surface was associated with SIDS (multivariate OR 2.89, 95% CI 1.40, 5.97). The largest risk was associated with couch sharing (OR 66.9, 95% CI 2.8, 1597). Of 46 SIDS infants who bedshared during their last sleep, 40 (87%) were found in the parents' bed. Sharing a bed when <11 weeks (OR 10.20, 95% CI 2.99, 34.8) was associated with a greater risk, P=.010, compared with sharing when older (OR 1.07, 95% CI 0.32, 3.56). The association remained if: Mother did not smoke (OR 8.01, 95% CI 1.20, 53.3) The infant was breastfed (OR 13.10, 95% CI 1.29, 133). Individual level analysis of five case-control studies: Individual data from five major case-control studies were combined to estimate the risk associated with bed sharing. 1472 cases, 4679 controls of a similar age. Bed sharing - defined as when one or both parents slept with the baby in their bed so that they woke to find the baby dead in bed with them. Breastfed – infant was being partially or completely breastfed at the time of death or interview. Peak incidence rate between 7 and 10 weeks. Individual level analysis of five case-control studies: For room sharing, breast-fed babies placed supine whose parents do not smoke and have no other risk factors the SIDS rate is predicted to be 0.08 (0.05 to 0.14)/1000 live births. For bed sharing, breast-fed babies placed supine whose parents do not smoke and have no other risk factors, the SIDS rate is predicted to be 0.23 (0.11 to 0.49)/1000 live births. This is a 2.7 fold increase in risk (CI 1.4 to 5.3 p=0.0027). There is a 5.1 fold increase in risk for the first 3 months of life (CI 2.3 to 11.4 p=0.00006). Adjusted ORs (AORs; log scale) for Sudden Infant Death Syndrome by age for bed sharing breast-fed infants, when neither parent smokes and both smoke versus comparable infants sleeping supine in the parents’ room. Robert Carpenter et al. BMJ Open 2013;3:e002299 ©2013 by British Medical Journal Publishing Group Bedsharing Promotes Breastfeeding 35 Latina mother-infant pairs, 20 routinely bed sharing, 15 solitary sleeping Observed for 3 consecutive nights in a sleep center For the routinely bed-sharing group on the bed-sharing night vs the routinely solitary sleeping on the solitary night: There were twice as many episodes of breastfeeding (p<.001) Total duration of episodes was nearly three times greater (P<.001) Mean duration of episodes was 39% greater (p=.039) For the routinely bed-sharing group, the number (p=.006) and total duration of breastfeeding episodes (p<.001) were significantly greater on the bed-sharing night than the solitary night with no significant difference in the time in bed or total sleep time Bedsharing Promotes Breastfeeding Replicated by Gettler and McKenna with 52 motherinfant pairs Mother-infant pairs engaged in a greater number of feeds while bed sharing than room sharing (p<.001) There was a lower interval between feeds (<0.05) Breastfeeding, Bed-Sharing and Infant Sleep 253 families completed the study, July 1998-February 2000 1-month and 3-month sleep logs and interview Breastfed and formula-fed infants exhibited different sleepwake patterns Formula-fed, but not breastfed infants had a significant reduction in frequency of night feeds between the first and third months 65% of infants who had “ever breastfed” slept in their parent’s bed (at least occasionally) as compared with 33% of formula-fed infants (p<0.000001) Breastfeeding, Bed-Sharing and Infant Sleep There was an association between bed-sharing at 1 month and breastfeeding to at least 16 weeks (p=0.02) Among mothers who were unemployed or had unskilled occupations, there was a significantly longer duration of breastfeeding among bed-sharing mothers as compared with those who were not (p=0.032) SUID Case Registry Pilot Program Collaboration between the CDC and the National Center for the Review and Prevention of Child Deaths (NCRPCD) Funded by the Health Resources and Services Administration Objectives: Collect accurate and consistent population-based data about the circumstances and events associated with SUID cases To improve the completeness and quality of SUID case investigations Use a decision making algorithm with standard definitions to categorize SUID cases. States: AZ, CO, LA, MI, MN, NJ, NM, NH, WI References Academy of Breastfeeding Medicine Protocol Committee. ABM Clinical protocol #6: guideline on Co-Sleeping and Breastfeeding. Breastfeed Med. 2008 Mar;3(1)38-42. Ball HL. Breastfeeding, bed-sharing, and infant sleep. Birth 2003; 30: 181–88. Bradley B et al. Potential Asphyxia and Brainstem Abnormalities in Sudden and Unexplained Death in Infants. Pediatrics. 2013. 132(6) e1616-25. Carpenter RG, et al. Sudden unexplained infant death in 20 regions in Europe: case control study. Lancet. 2004; 363(9404):185–191. Carpenter R, McGarvey C, Mitchell EA, et al. Bed sharing when parents do not smoke: is there a risk of SIDS? An individual level analysis of five major case– control studies. BMJ Open 2013;3:e002299. doi:10.1136/bmjopen-2012- 002299 Fleming, Peter et al. Bed-sharing and unexpected infant deaths: what is the relationship? Paediatric Respiratory Reviews. 16(1) 62-67. Gettler LT and McKenna JJ. Evolutionary Perspectives on Mother-Infant Sleep Proximity and Breastfeeding in a Laboratory Setting.American Journal of Physical Anthropology 144: 454-462. 2011. Hauck FR, et al. Breastfeeding and reduced risk of sudden infant death syndrome: a meta-analysis. Pediatrics. 2011; 128(1): 103–110. Hauck FR, et al. Sleep Environment and the Risk of Sudden Infant Death Syndrome in an Urban Population: The Chicago Infant Mortality Study. Pediatrics. 2003; 111(5 pt 2): 1207–1214. Infant Mortality. City of Milwaukee Health Department. 11/18/13: http://city.milwaukee.gov/Infant-Mortality Kinney HC, Thach BT. The sudden infant death syndrome. N Engl J Med. 2009;361(8): 795–805. Lee JJ and Martonffy AI. What sleeping arrangements are safe for infants and at what age are these precautions no longer needed? Evidenced Based Practice. March 2013. p6. McKenna JJ et al. Bedsharing Promotes Breastfeeding. Pediatrics. 1997; 100(2):214-219. McKenna JJ and McDade T. Why babies should never sleep alone: A review of the co-sleeping controversy in relation to SIDS, bedsharing and breast feeding. Pediatric Respiratory Reviews. 2005; 6: 134-152. Moreno, MA. The controversial but common practice of bed sharing. JAMA pediatrics. 2013. 167(11)1088. Ostfeld et al, Concurrent Risks in Sudden Infant Death Syndrome. Pediatrics 2010, 125 (3)447-453. Shapiro-Mendoza, CK et al. The sudden unexpected infant death case registry: a method to improve surveillance. Pediatrics. 2012. 129(2)486-93. Sudden Unexpected Infant Death and Sudden Infant Death Syndrome. CDC. Accessed 10/18/15: http://www.cdc.gov/sids/ Tappin D, Ecob R, Brooke H. Bedsharing, roomsharing, and sudden infant death syndrome in Scotland: a case-control study. J Pediatr. 2005;147(1):32–37. Task Force on Sudden Infant Death Syndrome. Pediatrics. 2011; 128(5): 1030–1039. Vennemann MM, Findeisen M, Butterfass-Bahloul T, et al. Modifiable risk factors for SIDS in Germany: results of GeSID. Acta Paediatr. 2005;94(6):655–660. Vennemann MM et al. Sleep Environment Risk Factors for Sudden Infant Death Syndrome: The German Sudden Infant Death Syndrome Study. Pediatrics. 2009; 123(4): 1162-1170.