New technology for
MRSA screening
Dr Richard Cunningham
Plymouth UK
Outline
Should we screen for MRSA?
What methods are available?
Why and how we introduced PCR
testing in Plymouth
What effect it has had
Should we screen?
Is MRSA an important problem?
Does colonisation precede infection?
Is the test sensitive and specific?
Is the yield enough to make it
worthwhile?
Are effective interventions available?
Is the cost reasonable?
Effect of MRSA surveillance on CCU
(Huang et al, CID Oct 2006)
Preemptive isolation
Harbarth et al
Critical Care 2006
Significant fall in
transmission rate on
medical ICU after
preemptive isolation
introduced
No change in
transmission rate on
surgical ICU
PCR
MRSA screening methods
Liquid culture
Chromagar
PCR
In house assays
IDI-MRSA/BD Geneohm
GenoQuick MRSA assay
Other rapid methods
Baclite (3M)
Other MRSA detection methods
Chromagar
We use as confirmatory test and at
weekends
Less sensitive, highly specific, much
cheaper
Takes 24-48 hours
BacLite
Selective broth, immunomagnetic
separation of MRSA, bioluminescent
detection
93.4% sensitive, 96.7% specific, cheaper
than PCR
Takes 5 hours
Genoquick MRSA assay
Holfelder et al Clin Micro Inf Dis 2006
242 patients, multiple body sites
Prevalence approx 5%, PPV 85%, NPV 99%
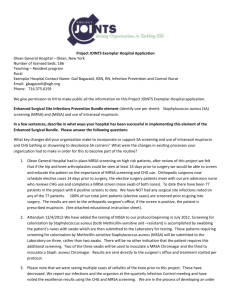
IDI-MRSA™ Assay
Nasal Swab
Specimen
Prep
Lysis - DNA
Extraction
Reconstitution Real-time PCR
Analysis on the
SmartCycler®
Instrument
Definitive
On-screen
Results
Results within 2 Hours
9
Copyright © 2005 GeneOhm, Inc. – All rights reserved
Junction Region
for Detection
SCCmec
Staphylococcal
Chromosomes
orfX
MRSA
orfX
MSSA
Primers
DNA detection of the SCCmec-orfX junction found only in
MRSA provides definitive identification of MRSA
Detects both HA-MRSA and CA-MRSA strains
Cell Lysis and DNA Preparation
Transfer entire cell
suspension
Add 50 µL
Sample Buffer
Centrifuge
5 min
Nasal
Swab
Remove
supernatant
Vortex in
Lysis
Sample Buffer Tube
1 min
4oC
DNA
Extra spin
95oC
2 min
Vortex
5 min &
Centrifuge
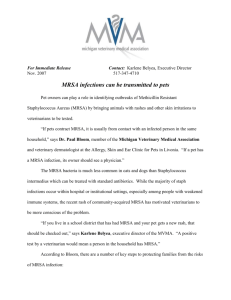
IDI-MRSA published test
performance
Number
Sensitivity %
Specificity %
Author
778
92.5
96.4
Manufacturers data
98.7
95.4
Huletsky
J Clin Micro 2004
287
96
96
Desjardins
J Clin Micro 2006
75
89
97
Davidson
J Hosp Inf 2006
1211
95
98.8
Wren
J Clin Micro 2006
1657
569
MRSA
MSSA
Derriford
Hospital
1000
bed Teaching Hospital
19 adult critical care beds*
Specialist units
Orthopaedic surgery*
Cardiac surgery*
Neurosurgery
Thoracic surgery
Plastic surgery
Renal transplant
Haematology/oncology
Public perception 2005
Quantifying our MRSA problem
Critical Care Unit
7%
Pre-operative assessment
Orthopaedic trauma
Orthopaedic elective
Elective vascular surgery
Elective general surgery
20% & 4%
2%
5.5%
4%
MRSA Bacteraemia
98 cases in 03/04
Solution - admission screening?
Culture based
Elective vascular surgery
Elective orthopaedics
PCR based
Critical care admissions
Cardiac surgery
Emergency orthopaedics
Implementation
Setting up laboratory
aspects of PCR testing
is easy
Convincing clinicians is
straighforward
Persuading managers
to fund it is difficult
Example business case
3000 tests/yr
Critical Care admissions
Elective cardiac surgery
Emergency orthopaedic surgery
Costs
Capital
Consumables
Staffing
£30,000
£50,000
£25,000
Business case
Assume prevention of;
5 bacteremias
3 mediastinitis
5 sternotomy infections
4 orthopaedic implant infections
pre-op prophylaxis
Predicted net savings
£145,000/yr
£37,500
£60,000
£50,000
£40,000
£32,500
Antibiotic savings
Cardiac surgery prophylaxis (1000 cases, 3% prevalence)
With MRSA
PCR
Without
MRSA PCR
Teicoplanin
doses
(£34/dose)
Cefuroxime
doses
(£1/dose)
Total cost
30
1000
£1,962
1000
1000
£34,670
Saving
£32,708
Critical Care MRSA PCR screening
693 CCU patients between September
2005 and February 2006
Weekdays only
Positive cases decolonised
Patients not routinely isolated
Confirmed by culture
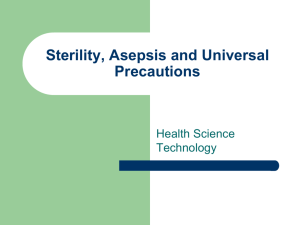
Results
25%
Culture screening
PCR screening
20
20%
15
15%
10
10%
5
5%
0
0%
Ap
0
ril
5
M
ay
05
ne
u
J
05
ly
Ju
05
A
u
ug
0
st
5
pt
e
S
b
m
e
05
r
e
c
O
be
o
t
5
0
r
em
v
No
05
r
be
em
c
De
05
r
be
n
Ja
ry
a
u
06
MRSA positive on admission %
Number of transmissions/1000 patient days
25
Results
(transmissions per 1000 patient/days)
Culture screening phase
PCR screening phase
13.9
4.9 (p<0.05)
Relative risk reduction 65%
Cunningham et al J Hosp Infect 2007
Critical Care Unit associated
MRSA bacteraemia
MRSA status unknown
MRSA pos on admission
MRSA neg on admission
Screening
introduced
18
16
14
12
10
8
6
4
2
0
4
/
3
0
20
5
/
4
0
20
6
/
5
0
20
/7
6
0
20
Predictive value on CCU*
1st Generation test 2nd Generation test
Sensitivity 96.8%
97.2%
Specificity 97.3%
99.4%
PPV
70.4%
94.7%
NPV
99.7%
99.7%
*1026 patients, considered true positive if MRSA culture
positive within 1 week of PCR result
Good negative predictive value!
Orthopaedic surgery
Always a challenge!
Problems
multiple teams
multiple wards
incomplete adherence to screening and
antibiotic policies
short timeframe between admission and
surgery
very low baseline infection rates make it
difficult to assess impact of testing
Savings
Predicted
reduction
Bacteraemia
5
Observed
reduction
8
Sternotomy
5
12
Antibiotic
prophylaxis
Saving
£120,000
£60,000
£32,000
£212,000
Better press this year!
MRSA cases fall at Devon
hospital
In the last year the hospital has been screening some patients
before they are admitted to hospital for surgery.
Those found to be carrying the bug are given eradication therapy
to get rid of the bacteria before it becomes a problem for them or
anyone else in the hospital.
Derriford is also using a new state-of-the-art screening system,
which reduces the detection of MRSA from five days to three
hours, minimising the risk of infection.
Derriford Hospital is on course to hit
its target for reducing bloodstream
infections from MRSA, new figures
show.Director of infection control
Dr Peter Jenks has told councillors
that Plymouth Hospitals Trust was
two cases below its target for the
financial year with just a couple of
weeks to go.
Cases of the antibiotic-resistant superbug MRSA
have fallen at the South West's biggest hospital.
The figures are contained in a report to be
discussed by Plymouth Hospitals Trust, which runs
Derriford Hospital.
The unconfirmed figures show a fall in both
numbers and rates of cases. In the year to April
Derriford had 88 cases - a fall of 10 from the
previous year.
Future plans
From April 2007 expanded MRSA screening
PCR
Culture
Neurosurgery
Thoracic surgery
Plastic surgery
Haematology & Oncology admissions
Acute medical admissions >60yrs
Acute surgical admissions >60yrs
Elective surgical pre-assessment
Weekend service
Conclusion
Is MRSA an important problem? - Yes
Does colonisation precede infection?- Yes
Is the test sensitive and specific?- Yes
Does the yield make it worthwhile?- Yes
Are effective interventions available?- Yes
Is the cost reasonable?- Yes
Thank you for your attention
Any questions?